Background: OTPD, LMPD, etc.
Systemic, Institutionalized Problem of Evidence-obviated Medicine
As a direct result of Directorate of Health's medically & ethically flawed 2014 Recommendation (i.e., national medical policy) all medical thinking, medical decision-making and medical actions for a woman's pregnancy for which time is a factor (i.e., almost all) are required to be based, exclusively, on the temporal frame of reference established by the estimated date of delivery (EDD) and, therefrom, a calculated gestational age (GA), using Naegele's rule, in reverse, established by an exclusive, national provider and exclusive method, NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) against the clear and explicit warnings of the risks and consequences by Norway's medical experts in obstetric medicine, fetal medicine and obstetric clinical care. Specifically, the "exclusive, national provider and exclusive method" qualification is implemented as follows:
GA Variances & Ovulation-Test-Positive Date (OTPD)
There are variances that come into play when directly estimating GA from ultrasound-based measurements of fetal metrics, or when directly estimating EDD from ultrasound-based measurements of fetal metrics. These widely reported GA variances from various studies, include:
Gestational Age Variance Components 1978 1991
Gestational age [ovulation & insemination] 52% 50%
Individual random [fetal growth velocity] 31% 30%
Measurement accuracy (ultrasound) 11% 20%
Lack of measurement reliability (ultrasound) 6%
Total: 100% 100%
Today's over-the-counter, home ovulation tests and test systems (e.g., Clearblue Fertility Monitor) are highly accurate (i.e. high sensitivity (low false positives) with high specificity (low false negatives)) with sophisticated, lab-on-a-chip technologies using monoclonal antibodies as reagents. Some urinary ovulation tests are reported to be more accurate than blood serum tests. Consequently, by tracking the profiles of two hormones, i.e., estrogen ramp-up and luteinizing hormone (LH) rise & surge, ovulation tests provide women with:
As a direct result of Directorate of Health's medically & ethically flawed 2014 Recommendation (i.e., national medical policy) all medical thinking, medical decision-making and medical actions for a woman's pregnancy for which time is a factor (i.e., almost all) are required to be based, exclusively, on the temporal frame of reference established by the estimated date of delivery (EDD) and, therefrom, a calculated gestational age (GA), using Naegele's rule, in reverse, established by an exclusive, national provider and exclusive method, NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) against the clear and explicit warnings of the risks and consequences by Norway's medical experts in obstetric medicine, fetal medicine and obstetric clinical care. Specifically, the "exclusive, national provider and exclusive method" qualification is implemented as follows:
- obviating all other ultrasound-based methods and models of estimating GA or EDD and, depending on the other method, the calculation of their complement EDD or GA, respectively
- at the scheduling of the "routine" 18wUSE, all of a pregnant woman's personal medical information in the form of her factual key pregnancy dates (e.g., LMPD, OTPD, SCID, menstrual cycle history and, until recently, in vitro fertilization date (IVFD)) are obviated from all medical evidence and any and all consideration in medical thinking, medical decision-making and medical actions; personal medical evidence is obviated without the pregnant woman's prior, informed voluntary consent; medical evidence a pregnant women uses to establish: 1) the beginning of her pregnancy, 2) her GA and, therefrom, 3) her calculated EDD using the equivalent of Naegele's rule (i.e. simply adding 280 (or 282) days to her LMPD, or by adding 266 (or 268) days to her OTPD or SCID)
- at the the "routine" 18wUSE the only fetal biometry measurements taken and recorded on the ultrasound report by NCFM eSnurra Group's protocol are those measurements for which NCFM eSnurra Group has a corresponding model to predict EDD. For example, NCFM eSnurra measures the BPD and, from their EDD prediction/estimation model for BPD measurements, assigns an NCFM eSnurra BPD-based EDD and, therefrom, a calculated GA using the equivalent of Naegele's rule, to a pregnancy as NCFM eSnurra BPD-based EDD & GA. However, NCFM eSnurra will not measure the more robust fetal head circumference (HC) and include this measurement on the ultrasound report because NCFM eSnurra Group does not have a corresponding EDD prediction/estimation model for HC measurements, even though an HC measurement can be used, easily, with publicly accessible models and HC reference charts of proven efficacy to establish EDD & GA which could be used to cross-check NCFM eSnurra BPD-based EDD & GA for reasonableness, errors or efficacy, and to identify potential fetal pathology masked by an inaccurate or grossly inaccurate NCFM eSnurra BPD-based EDD & GA. Moreover, BPD is recognized, internationally, as a problematic, unreliable measurement for predicting/estimating EDD or GA during routine ultrasound exams, and the more robust HC measurement should be used instead, or in conjunction with BPD, but BPD should not be used alone.
- Consequently, without an HC measurement or a woman's combined, fully corroborating, factual LMPD/OTPD/SCID (i.e., the woman's obviated medical evidence) there is no medical evidence, whatsoever, with which to cross-check NCFM eSnurra BPD-based EDD & GA for reasonableness, errors or efficacy, or to identify potential fetal pathology masked by an inaccurate or grossly inaccurate NCFM eSnurra BPD-based EDD & GA. This unnecessary situation creates completely unnecessary risks; risks which are proven to cause critical medical mistakes which result in grievous harms, as was the case for Laila and her baby, and other women and their babies.
GA Variances & Ovulation-Test-Positive Date (OTPD)
There are variances that come into play when directly estimating GA from ultrasound-based measurements of fetal metrics, or when directly estimating EDD from ultrasound-based measurements of fetal metrics. These widely reported GA variances from various studies, include:
- ovulation variances: up to 50% of total gestational variance in pregnancies
- random fetal growth velocity variances: 30% of total gestational variance
- random ultrasound measurement errors & accuracy variances: 20% of total gestational variance
Gestational Age Variance Components 1978 1991
Gestational age [ovulation & insemination] 52% 50%
Individual random [fetal growth velocity] 31% 30%
Measurement accuracy (ultrasound) 11% 20%
Lack of measurement reliability (ultrasound) 6%
Total: 100% 100%
- 1978: (Source: "Normal Range Curves for the Intrauterine Growth of the Biparietal Diameter" P.-H. Persson, L. Grennert, G. Gennser, B. Gullberg, Acta Obstricia et Gynecologica Scandinavia Volume 57, Issue S78, January 1978, Pages 15–20)
- 1991: (Source: "Ultrasound instead of last menstrual period as the basis of gestational age assignment" R.T. Geirsson, Ultrasound Obstet. Gynecol. 1 (1991) 212-219)
Today's over-the-counter, home ovulation tests and test systems (e.g., Clearblue Fertility Monitor) are highly accurate (i.e. high sensitivity (low false positives) with high specificity (low false negatives)) with sophisticated, lab-on-a-chip technologies using monoclonal antibodies as reagents. Some urinary ovulation tests are reported to be more accurate than blood serum tests. Consequently, by tracking the profiles of two hormones, i.e., estrogen ramp-up and luteinizing hormone (LH) rise & surge, ovulation tests provide women with:
- precise fertility awareness,
- peak fertility days,
- rising EG3 & LH and peak LH surge for optimal fertility awareness
- elimination of ovulation variance from total gestational variance for her pregnancy
- "Contact a midwife or your doctor
As soon as a reliable test has confirmed that you are pregnant, contact a midwife or your regular GP. They will give you essential information from the very start of your pregnancy." (Source: "Pregnancy and maternity care in Norway" Directorate of eHealth, Helsenorge.no. Content provided by Directorate of Health)
- "17-19 weeks pregnant - Ultrasound
Your midwife or doctor will give you information about the ultrasound scan that will take place at 17-19 weeks. The purpose of the ultrasound is to estimate when your baby is due (date), check the number of babies (twins, triplets), and check the position of the placenta and the physical development of the baby. The ultrasound is usually performed at an outpatient clinic at the hospital where you will be having your baby." (Source: ibid.)
- "In summary, we have described the fertile days of the menstrual cycle for a group of healthy women. By analyzing data on the day of ovulation (identified by means of hormone assays of daily urine specimens) and daily records of sexual intercourse, we found that all conceptions resulted from intercourse that occurred during a six-day interval ending on the day of ovulation. The sex of the baby was not related to the timing of intercourse in relation to ovulation." (Source: "Timing of Sexual Intercourse in Relation to Ovulation — Effects on the Probability of Conception, Survival of the Pregnancy, and Sex of the Baby" Allen J. Wilcox, M.D., Ph.D., Clarice R. Weinberg, Ph.D., and Donna D. Baird, Ph.D. New England Journal of Medicine 1995; 333:1517-1521 December 7, 1995. DOI: 10.1056/NEJM199512073332301)
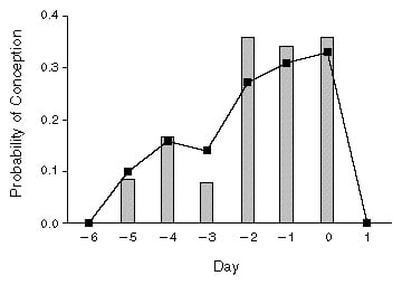
Figure 2
Probability of Conception on Specific Days near the Day of Ovulation. The bars represent probabilities calculated from data on 129 menstrual cycles in which sexual intercourse was recorded to have occurred on only a single day during the six-day interval ending on the day of ovulation (day 0). The solid line shows daily probabilities based on all 625 cycles, as estimated by the statistical model. |
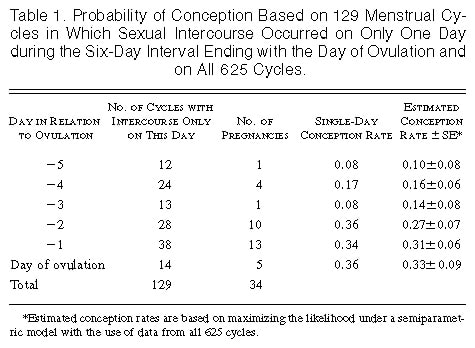
Table 1
Probability of Conception Based on 129 Menstrual Cycles in Which Sexual Intercourse Occurred on Only One Day during the Six-Day Interval Ending with the Day of Ovulation and on All 625 Cycles. |
Given Laila's OTPD and the results of Wilcox et al. 1995 (and other studies, e.g., Jukic et al. 2013), there was zero probability of conception resulting from coitus the day after ovulation. Combine this knowledge with the knowledge of Laila's factual SCID (i.e., which was also the 'actual ovulation' date or OTPD + 1) was evidence of the beginning of her pregnancy and her: GA = 2w+1 = OTPD +1 = SCID. No routine ultrasound-based estimation (or calculation) of GA is more accurate. This is a fact, not an opinion. It is also a fact that combining ultrasound-data with all available information, including LMPD/OTPD/SCID-based GA & EDD provide optimal obstetric and fetal awareness to enable optimal obstetric and fetal management to prevent unnecessary increased medical risks, critical medical mistakes and grievous medical harms. Finally, it is a fact home-use, urinary ovulation tests entered the mass market in 1989, 4-years after home-use, urinary pregnancy tests, in 1985. Home use ovulation tests are highly reliable (high sensitivity (i.e., low false positives) & high specificity (i.e., low false negatives)). As a statement of fact, Laila relied on Clearblue brand ovulation tests and pregnancy tests, to good effect. Following are links which describe, in detail, the Clearblue ovulation tests and test system, respectively. Laila's medical professionals were aware of the capabilities of pregnancy tests, but they were not aware of the capabilities of today's ovulation tests and test systems. Moreover, they did not know how to use ovulation tests to:
- signal rising E3H & LH and then peak LH for high and then peak fertility awareness, respectively,
- coitus timing for conception,
- conception probabilities by coitus day(s),
- establishing the beginning of pregnancy and fetal age
- the dating of the pregnancy's gestational period (gestational age or GA),
- the elimination of ovulation variance from total gestational variance,
- the identification of grossly inaccurate ultrasound-based GA & EDD
- the identification of fetal pathology which, otherwise, would remain masked by grossly inaccurate ultrasound-based GA & EDD
- "Our data emphasize the importance of identifying the growth-restricted infants in the prolonged and post-term phase of pregnancy due to their increased perinatal mortality risk. However, one of the most important clinical implications of our study is that these growth restricted infants should probably not have their gestational age determined solely by ultrasound." (Source: "Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study" Nils-Halvdan Morken, Kari Klungsøyr and Rolv Skjaerven. BMC Pregnancy and Childbirth 2014 14:172. https://doi.org/10.1186/1471-2393-14-172. Received: 20 January 2014, Accepted: 7 May 2014, Published: 22 May 2014)
The warnings of the above by Bergen Group to Directorate of Health were clear and explicit regarding critical medical mistakes and the need of optimal obstetric and fetal awareness via accurate assessments of fetal age and GA.
Included below, again, is an excerpt from the "Conclusion" section of NCFM eSnurra Group's Gjessing et al. 2007 that explicitly touts that NCFM eSnurra obviates LMPD at the scheduling of the 18wUSE (i.e., along with all other factual, key pregnancy dates from medical evidence as an NCFM eSnurra product feature. Please note the use of the word "obviates" in the excerpt.
Models to Predct/Estimate EDD with The Hutchon Method of PDEE
The number of days from the ultrasound date to actual birth/delivery is calculated and used as a dependent variable (i.e., what is to be predicted/estimated) often referred to as the interval to delivery (ITD) or days remaining (RE). The fetal metric measurements are used as independent variables (the predictor variables). In general, a separate regression model (line/curve) is constructed for each fetal metric by regressing ITD/RE on each fetal metric measurement, such as HC, BPD & FL, to create a separate regression model (line/curve) for each fetal metric to predict/estimate ITD/RE for individual pregnancies. Sometimes, fetal metrics are combined in multiple regression models. A key advantage of the Hutchon Method of PDEE is the only bias or error in the model is random ultrasound measurement error and random fetal growth velocity variances. These 2 sources of random error exist in all ultrasound fetal biometry measurements, with fetal growth velocity variances increasing, naturally, with gestational age.
Advantages & Benefits of The Hutchon Method of PDEE
Not surprisingly, all of the benefits of the Hutchon Method of PDEE relate to EDD, none relate to GA, as Dr. Hutchon explained in his seminal Hutchon 1998, website and his other publications. These EDD benefits were parroted in NCFM eSnurra Group's Gjessing et al. 2007
Background: Bergen Group: Estimation of GA (Terminhjulet or Forward wheel):
The use of factual LMPD/OTPD/SCID and other dates e.g., ID, IVF, ICSI, ZIFT, etc. can eliminate up to 50% of total GA variance in individual pregnancies, thus enabling:
Background: Trondheim Group: Direct EDD Estimation (NCFM eSnurra)
In contrast, the method that estimates the days remaining from the ultrasound date until actual delivery date in order to generate an estimate of EDD (Trondheim Group, NCFM eSnurra) will neither acknowledge nor utilize patient-specific key pregnancy dates such as LMPD/OTPD or other dates. In fact, at the scheduling of the "routine" 18wUSE all of a woman's key pregnancy dates are obviated (i.e., LMPD, OTPD, SCID, IVF, ICSI, ZIFT, etc.), without the pregnant woman's prior, informed, voluntary consent. At the "routine" 18wUSE exam, fetal metric measurements are made and used to directly estimate the number of days remaining to date of delivery in order to establish the "official" NCFM eSnurra EDD, and this EDD is then used to calculate the GA by subtracting the estimated number of days remaining to date of delivery from 283 days (NCFM eSnurra's established median gestation period) to establish the GA on the date of the ultrasound exam. Ironically, this calculation uses a "virtual" version of the obviated LMPD, because LMPD is the zero-day at the other end the 283 days NCFM eSnurra uses as their median gestation period. The problem with the NCFM eSnurra method is that it also obviates: 1) the ability to eliminate of up to 50% of total GA variance for individual pregnancies, 2) ability to improve the determination of GA by considering LMPD/OTPD in conjunction with direct estimates of EDD used to calculate GA and 3) the ability to identify potential fetal pathology from being masked by an otherwise too young or too old GA calculated from an inaccurate direct estimate of EDD from fetal metric ultrasound measurements alone. Nevertheless, and according to Directorate of Health's 2014 Recommendation, the "official" NCFM eSnurra EDD & GA are assigned as the "official" temporal frame of reference to a woman's pregnancy for the duration of her pregnancy, whether she wants this or not because all the medical evidence necessary to test NCFM eSnurra EDD & GA for reasonableness, errors or efficacy is "routinely" obviated. The practice of intentionally obviating medical evidence of proven medical value and efficacy is the practice of evidence-obviated medicine. Directorate of Health's government-mandated protocol of obviating all key pregnancy dates has caused, and will continue to cause, increased medical risks, critical medical mistakes and grievous medical harms as a result of suboptimal medical thinking, medical decision-making and medical actions in the delivery of medical care to Norway's women and their fetuses/babies; critical medical mistakes which are proven to cause grievous medical harms, including perinatal death. Moreover, there is absolutely nothing to stop this insidious, systemic problem created by Directorate of Health and NCFM eSnurra Group, yet.
Background: Ultrasound vs. Reliable LMPD: 6% Difference, Ergo Use Both
In the study excerpt below, the authors (NCFM Snurra Group members) concluded ultrasound was "the significantly better predictor of day of delivery" over reliable LMPD, 52% to 46% (apparently 2% tied). Sure, in a political election a 6% margin is considered "significantly better," maybe even a landslide, but for obviating medical evidence that could unmask fetal pathology and enable timely medical intervention, not so much. This 52% to 46% comparison is more like having 9 guests in one's living room who were served coffee and 5 requested sugar and 4 requested cream, so it was decided sugar was the significantly better coffee enhancer for all 9 and the cream option was summarily obviated. Ultrasound, 52% vs. reliable LMPD, 46% is not at all significant, especially from a patient's perspective. From a patient's perspective this 6% difference screams: "use both ultrasound & reliable LMPD," especially when one considers the cost of an ultrasound exam vs. the cost of using a reliable LMPD (free). This is where the words "significantly better" make more sense because it costs nothing more than some thinking to use both ultrasound and reliable LMPD to deliver both a better GA and better obstetric care. One cannot help but wonder how an LMPD/OTPD combination would compare against ultrasound if this same study were repeated today because a reliable LMPD does not eliminate ovulation variance, but an ovulation test does. Let's at least start out by considering both LMPD/OTPD and ultrasound-based estimations when assigning fetal and gestational age and, especially since potential fetal pathology can be masked by an inaccurate ultrasound-based GA, which is exactly what happened to Laila and our baby, and other women and their fetuses/babies.
Background: Ultrasound-based EDD Not Better Than LMPD-based EDD
- "We argue that critical mistakes may follow from the failure to include all available information when fetal age is assessed." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age", Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "However, the issue at stake is not the accuracy of the predicted date of a normal delivery, it is the accuracy of the fetal age, which is an essential factor in clinical situations throughout the pregnancy." (Source: ibid.)
Included below, again, is an excerpt from the "Conclusion" section of NCFM eSnurra Group's Gjessing et al. 2007 that explicitly touts that NCFM eSnurra obviates LMPD at the scheduling of the 18wUSE (i.e., along with all other factual, key pregnancy dates from medical evidence as an NCFM eSnurra product feature. Please note the use of the word "obviates" in the excerpt.
- "The model [NCFM eSnurra] obviates the dependence on last menstrual period found in standard methods for term prediction, and allows an immediate assessment of prediction quality in a population setting." (Source: Ultrasound Obstet Gynecol 2007; 30: 19–27, "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, DOI: 10.1002/uog.4053)
- By adopting this approach we do not need to concern ourselves about the length of the cycle nor the certainty of the dates. Provided the fetus can be assessed as normal using other criteria, this chart can be used to provide the best estimate of the date of delivery (EDD)." (Source: 'Back to the Future' for Hermanni Boerhaave or 'A rational way to generate ultrasound scan charts for estimating the date of delivery, Hutchon DJR, ObGyn Ultrasound, Obgyn.net 1998: Back to the Future' for Hermanni Boerhaave or 'A rational way to generate ultrasound scan charts for estimating the date of delivery [Note: URL since updated by ObGyn.net])
- "Just as Boerhaave was not actually measuring the length of pregnancy, and the word "gestation" is used to describe the measurement of time from the last menstrual period to reflect this, so also there is no pretence that this method is determining fetal age." (Source: ibid.)
- "However, the issue at stake is not the accuracy of the predicted date of a normal delivery, it is the accuracy of the fetal age, which is an essential factor in clinical situations throughout the pregnancy." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" & ("Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder") Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "Fetal age, fetal size, length of pregnancy and date of delivery are obviously all related data. However, it is impossible to deduce fetal age routinely from the predicted date of delivery. Only 4 per cent of women give birth at their estimated due date; in order to determine gestational age, it is clearly necessary to take account of the time of conception. The Directorate of Health have demonstrated their lack of understanding of these differences, and they have failed to appreciate that the Trondheim Group looked only at term prediction (3)." (Source: ibid.)
- "What exactly are we doing when we date a pregnancy by ultrasound? Clearly if no reliable menstrual data are available, there is no alternative to ultrasound dating. However, when apparently reliable menstrual data are available, it is not expected that the scan size should always fall precisely on the mean for that gestation. Nor does the way the ultrasound charts are generated support this expectation. It would be nonsense to suggest that all fetuses with a BPD of, say 35 mm, are all at precisely the same gestational age. If ultrasound dating is more accurate, then we are essentially proposing that the interval to delivery from the ultrasound scan of some specific value (e.g. 35mm) is less variable than the last menstrual period to delivery interval. Fetal size is being used as the predictor of the delivery interval. If using ultrasound size is the most accurate way to predict the date of delivery, then the ultrasound charts should be generated using these same principles." (Source: CORRESPONDENCE Re: "Routine ultrasound is the method of choice for dating pregnancy" David J. R. Hutchon, 11 November 1998, Br J Obstet Gynuecol 106, 610-616, p 616)
- date of the ultrasound exam for a pregnancy when fetal metric measurements were taken; if recorded correctly, contains no bias; the date for which all time begins for a pregnancy for the Hutchon Method of PDEE is the ultrasound date; therefore, nothing prior to the ultrasound date is considered, which is why Dr. Hutchon cautioned about using his method to determine fetal age
- fetal metric measurements taken (e.g., CRL, HC, BPD, FL, MAD etc.) on the ultrasound exam date are subject to random ultrasound measurement error and random fetal growth velocity variances, as is the case with all ultrasound fetal biometry measurements, with growth velocity variances increasing with GA
- actual date of birth/delivery for the pregnancy; if recorded correctly, contains no bias
Models to Predct/Estimate EDD with The Hutchon Method of PDEE
The number of days from the ultrasound date to actual birth/delivery is calculated and used as a dependent variable (i.e., what is to be predicted/estimated) often referred to as the interval to delivery (ITD) or days remaining (RE). The fetal metric measurements are used as independent variables (the predictor variables). In general, a separate regression model (line/curve) is constructed for each fetal metric by regressing ITD/RE on each fetal metric measurement, such as HC, BPD & FL, to create a separate regression model (line/curve) for each fetal metric to predict/estimate ITD/RE for individual pregnancies. Sometimes, fetal metrics are combined in multiple regression models. A key advantage of the Hutchon Method of PDEE is the only bias or error in the model is random ultrasound measurement error and random fetal growth velocity variances. These 2 sources of random error exist in all ultrasound fetal biometry measurements, with fetal growth velocity variances increasing, naturally, with gestational age.
Advantages & Benefits of The Hutchon Method of PDEE
Not surprisingly, all of the benefits of the Hutchon Method of PDEE relate to EDD, none relate to GA, as Dr. Hutchon explained in his seminal Hutchon 1998, website and his other publications. These EDD benefits were parroted in NCFM eSnurra Group's Gjessing et al. 2007
- does not depend on the lengthy or regularity of a woman's menstrual cycle
- does not depend of LMPD
- observations to construct the model do not require studies of women with regular cycles or reliable LMPD
- historical database records of the 3 required inputs are plentiful among different populations
- the models can be updated continuously with new observations as they present
- the large numbers of observations will yield narrow confidence intervals
- co-factors such as parity, smoking, gender, other fetal metrics, etc. are easy to add to create customized EDD charts
- etc.
Background: Bergen Group: Estimation of GA (Terminhjulet or Forward wheel):
The use of factual LMPD/OTPD/SCID and other dates e.g., ID, IVF, ICSI, ZIFT, etc. can eliminate up to 50% of total GA variance in individual pregnancies, thus enabling:
- highly accurate estimates of when a pregnancy begins,
- improved determination of fetal age and GA by considering LMPD/OTPD/SCID and other dates in conjunction with direct estimates of GA from fetal ultrasound measurements while, at the same time,
- helping to identify potential fetal pathology from being masked by an erroneous too-young or too-old GA directly estimated from ultrasound measurements alone.
Background: Trondheim Group: Direct EDD Estimation (NCFM eSnurra)
In contrast, the method that estimates the days remaining from the ultrasound date until actual delivery date in order to generate an estimate of EDD (Trondheim Group, NCFM eSnurra) will neither acknowledge nor utilize patient-specific key pregnancy dates such as LMPD/OTPD or other dates. In fact, at the scheduling of the "routine" 18wUSE all of a woman's key pregnancy dates are obviated (i.e., LMPD, OTPD, SCID, IVF, ICSI, ZIFT, etc.), without the pregnant woman's prior, informed, voluntary consent. At the "routine" 18wUSE exam, fetal metric measurements are made and used to directly estimate the number of days remaining to date of delivery in order to establish the "official" NCFM eSnurra EDD, and this EDD is then used to calculate the GA by subtracting the estimated number of days remaining to date of delivery from 283 days (NCFM eSnurra's established median gestation period) to establish the GA on the date of the ultrasound exam. Ironically, this calculation uses a "virtual" version of the obviated LMPD, because LMPD is the zero-day at the other end the 283 days NCFM eSnurra uses as their median gestation period. The problem with the NCFM eSnurra method is that it also obviates: 1) the ability to eliminate of up to 50% of total GA variance for individual pregnancies, 2) ability to improve the determination of GA by considering LMPD/OTPD in conjunction with direct estimates of EDD used to calculate GA and 3) the ability to identify potential fetal pathology from being masked by an otherwise too young or too old GA calculated from an inaccurate direct estimate of EDD from fetal metric ultrasound measurements alone. Nevertheless, and according to Directorate of Health's 2014 Recommendation, the "official" NCFM eSnurra EDD & GA are assigned as the "official" temporal frame of reference to a woman's pregnancy for the duration of her pregnancy, whether she wants this or not because all the medical evidence necessary to test NCFM eSnurra EDD & GA for reasonableness, errors or efficacy is "routinely" obviated. The practice of intentionally obviating medical evidence of proven medical value and efficacy is the practice of evidence-obviated medicine. Directorate of Health's government-mandated protocol of obviating all key pregnancy dates has caused, and will continue to cause, increased medical risks, critical medical mistakes and grievous medical harms as a result of suboptimal medical thinking, medical decision-making and medical actions in the delivery of medical care to Norway's women and their fetuses/babies; critical medical mistakes which are proven to cause grievous medical harms, including perinatal death. Moreover, there is absolutely nothing to stop this insidious, systemic problem created by Directorate of Health and NCFM eSnurra Group, yet.
Background: Ultrasound vs. Reliable LMPD: 6% Difference, Ergo Use Both
In the study excerpt below, the authors (NCFM Snurra Group members) concluded ultrasound was "the significantly better predictor of day of delivery" over reliable LMPD, 52% to 46% (apparently 2% tied). Sure, in a political election a 6% margin is considered "significantly better," maybe even a landslide, but for obviating medical evidence that could unmask fetal pathology and enable timely medical intervention, not so much. This 52% to 46% comparison is more like having 9 guests in one's living room who were served coffee and 5 requested sugar and 4 requested cream, so it was decided sugar was the significantly better coffee enhancer for all 9 and the cream option was summarily obviated. Ultrasound, 52% vs. reliable LMPD, 46% is not at all significant, especially from a patient's perspective. From a patient's perspective this 6% difference screams: "use both ultrasound & reliable LMPD," especially when one considers the cost of an ultrasound exam vs. the cost of using a reliable LMPD (free). This is where the words "significantly better" make more sense because it costs nothing more than some thinking to use both ultrasound and reliable LMPD to deliver both a better GA and better obstetric care. One cannot help but wonder how an LMPD/OTPD combination would compare against ultrasound if this same study were repeated today because a reliable LMPD does not eliminate ovulation variance, but an ovulation test does. Let's at least start out by considering both LMPD/OTPD and ultrasound-based estimations when assigning fetal and gestational age and, especially since potential fetal pathology can be masked by an inaccurate ultrasound-based GA, which is exactly what happened to Laila and our baby, and other women and their fetuses/babies.
- "In women with a reliable menstrual history and spontaneous onset of labor, the ultrasound estimate was the significantly better predictor of the day of delivery in 52% of cases, and the last menstrual period estimate was the better predictor in 46% of cases." (Source: A comparison between ultrasound and a reliable last menstrual period as predictors of the day of delivery in 15,000 examinations., Tunón K, Eik-Nes SH, Grøttum P., Ultrasound Obstet Gynecol. 1996 Sep;8(3):178-85.)
- "It is concluded that ultrasound measurement of the biparietal diameter between 15 and 22 weeks of pregnancy is the best method for estimation of the day of delivery and should be used as a routine procedure." p. 178
- "It is in the interests of the obstetricians to estimate a day which is as close as possible to the actual day of delivery, for as many women as possible. We have shown that the variation of the births around the estimated day of delivery is significantly smaller for the ultrasound method than for the last menstrual period method." p. 184
- "For those with discrepancy between the last menstrual period estimate and the ultrasound estimate, the ultrasound estimate was a better predictor of the day of delivery for most of the deliveries. p. 184 (Again, this could mean 7,501 vs. 7,499)"
- "The ultrasound method for predicting day of delivery can therefore be recommended as the method of choice." p. 184
Background: Ultrasound-based EDD Not Better Than LMPD-based EDD
- Introduction
"In a leaflet issued by The Midwives Information and Resource Service (MIDIRS) and the National Health Service Centre for Reviews and Dissemination, pregnant women are informed that the expected day of delivery determined on the basis of an ultrasound scan “is more accurate than using a calendar and the date of your last period”’. The information is supported by reference to the Cochrane review Routine ultrasound in early pregnancy 2. Two questions arise, however: 1. Is the statement based on the best available evidence? 2. Is the statement correct? p. 1221
Other evidence
A change of the definition of the term from a last menstrual period of 280 days to one of 283 days is supported by the largest published cohort study, comprising 427,582 singleton pregnancies with a reliable last menstrual period. The authors conclude that the “average duration from last menstrual period to vaginal birth was 282 days (median), 281 days (mean) and 283 days (mode) 5." ( p. 1221)
Conclusion
We conclude that the statement in the MIDRS leaflet regarding accuracy is not based on the best available evidence and that it may be wrong in women who have regular cycles and known first day of the last menstrual period. p. 1222
Future research
"A consequence of the above observations is that the reduced incidence of induction of labour for apparent post-term pregnancy in the routinely scanned groups presumably does not result from better gestational dating but is due to a shift of the distribution curve leaving fewer pregnancies under the tail of the curve to be labelled ‘post-term’. Furthermore, it may even be possible that a more elaborate clinical method of predicting the day of delivery based on Nagele’s old rule may be better than dating based on an ultrasound scan." (p. 1222) (Source: "Routine ultrasound dating has not been shown to be more accurate than the calendar method" Olsen, O. and Aaroe Clausen, J. (1997), BJOG: An International Journal of Obstetrics & Gynaecology, 104: 1221–1222. doi:10.1111/j.1471-0528.1997.tb10965.x)