Increased Medical Risks, Critical Medical Mistakes & Grievous Medical Harms
"Medical error—the third leading cause of death in the US"
"Patient harm from medical error can occur at the individual or system level."
"Medical error is not included on death certificates or in rankings of cause of death."
"Medical error leading to patient death is under-recognized in many other countries, including the UK and Canada. 20 21"
(Source: "Medical error—the third leading cause of death in the US" Martin A Makary & Michael Daniel. BMJ 2016;353:i2139; or the PDF version)
[Note: The 12-minute BMJ interview with Martin A. Makary is worth the time (below).]
"Patient harm from medical error can occur at the individual or system level."
"Medical error is not included on death certificates or in rankings of cause of death."
"Medical error leading to patient death is under-recognized in many other countries, including the UK and Canada. 20 21"
(Source: "Medical error—the third leading cause of death in the US" Martin A Makary & Michael Daniel. BMJ 2016;353:i2139; or the PDF version)
[Note: The 12-minute BMJ interview with Martin A. Makary is worth the time (below).]
|
|
Medical Error: An International Problem
"We have estimated that medical error is the third biggest cause of death in the US and therefore requires greater attention. Medical error leading to patient death is under-recognized in many other countries, including the UK and Canada. 20 21 According to WHO, 117 countries code their mortality statistics using the ICD system as the primary indicator of health status. 22 The ICD-10 coding system has limited ability to capture most types of medical error. At best, there are only a few codes where the role of error can be inferred, such as the code for anticoagulation causing adverse effects and the code for overdose events. When a medical error results in death, both the physiological cause of the death and the related problem with delivery of care should be captured." (Source: "Medical error—the third leading cause of death in the US" Martin A Makary and Michael Daniel. BMJ 2016;353:i2139; p. 2. Also, the PDF version)
"We have estimated that medical error is the third biggest cause of death in the US and therefore requires greater attention. Medical error leading to patient death is under-recognized in many other countries, including the UK and Canada. 20 21 According to WHO, 117 countries code their mortality statistics using the ICD system as the primary indicator of health status. 22 The ICD-10 coding system has limited ability to capture most types of medical error. At best, there are only a few codes where the role of error can be inferred, such as the code for anticoagulation causing adverse effects and the code for overdose events. When a medical error results in death, both the physiological cause of the death and the related problem with delivery of care should be captured." (Source: "Medical error—the third leading cause of death in the US" Martin A Makary and Michael Daniel. BMJ 2016;353:i2139; p. 2. Also, the PDF version)
Harm = Adverse Event = (Event Risk x Event Consequences)
Risk Mitigation
While there may not be effective crosschecks to mitigate the risk of "a miscalculation in the given dose of a particular drug," there are highly accurate crosschecks available to mitigate the risk of a miscalculation in the given fetal age of a particular fetus. Incredulously, medical evidence of known, proven efficacy which could be used, easily, and at no cost, to crosscheck the given fetal age of a particular fetus for reasonableness, accuracy and efficacy is systematically obviated from all medical evidence and, thereby, from all medical thinking, medical decision-making and medical actions via a government-mandated protocol of evidence-obviated medicine; a protocol of unilateral reliance on ultrasound-based assignments of fetal & gestational age for pregnancies and abortions in Norway, no matter what! This is Directorate of Health's knowledge-obviated, medically & ethically flawed, willfully reckless, grossly negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized and misused Hutchon Method of PDEE).
In stark contrast, Bergen Group's protocol includes all available information, in conjunction with ultrasound data, in the practice of evidence-based medicine to establish the best possible fetal age (and gestational age) for a particular fetus to ensure optimal obstetric & fetal awareness to ensure optimal obstetric & fetal management.
- "Human error is inevitable. Although we cannot eliminate human error, we can better measure the problem to design safer systems mitigating its frequency, visibility, and consequences." (Source: ibid., p. 2)
- "Very often, the observed consequence (effect) of an event is mixed with the adverse event, making it difficult to separate the two. As an example, if the adverse event is a miscalculation in the given dose of a particular drug, the consequences could range from no event (most likely) to death (very infrequent), but the initial adverse event remains the same." (Source: "Adverse events and in-hospital mortality: an analysis of all deaths in a Norwegian health trust during 2011" Hans Flaatten, Guttorm Brattebø, Bjørn Alme, Kjersti Berge, Jan H. Rosland, Asgaut Viste, Bjørn Bertelsen, Stig Harthug and Sidsel Aardal. BMC Health Services Research (2017), 17:465, p.2) DOI 10.1186/s12913-017-2417-7. Published online 2017 Jul 6. PDF version)
- "Very often, the observed consequence (effect) of an event is mixed with the adverse event, making it difficult to separate the two. As an example, if the adverse event is" an unnecessary grossly erroneous calculation or estimation in the given gestational age an fetal age of a particular pregnancy and fetus, respectively, "the consequences could range from no event (most likely) to death (very infrequent), but the initial adverse event remains the same."
- "Very often, the observed consequence (effect) of an event is mixed with the adverse event, making it difficult to separate the two. As an example, if the adverse event is" a government-mandated protocol of evidence-obviated medicine, "the consequences could range from no event (most likely) to death (very infrequent), but the initial adverse event remains the same."
- "Very often, the observed consequence (effect) of an event is mixed with the adverse event, making it difficult to separate the two. As an example, if the adverse event is" "to cross the street with a blindfold and earmuffs on," "the consequences could range from no event (most likely) to death (very infrequent), but the initial adverse event remains the same."
- "There are many reasons a previous action may not have led to ruin while still having the potential to do so. If you attempt to cross the street with a blindfold and earmuffs on, you may make it across, but this is not evidence that such an action carries no risk." (Source: "The Precautionary Principle (with Application to the Genetic Modification of Organisms)" p. 11. Nassim Nicholas Taleb, Rupert Read, Raphael Douady, Joseph Norman, Yaneer Bar-Yam. EXTREME RISK INITIATIVE —NYU SCHOOL OF ENGINEERING WORKING PAPER SERIES. https://arxiv.org/pdf/1410.5787.pdf)
Risk Mitigation
While there may not be effective crosschecks to mitigate the risk of "a miscalculation in the given dose of a particular drug," there are highly accurate crosschecks available to mitigate the risk of a miscalculation in the given fetal age of a particular fetus. Incredulously, medical evidence of known, proven efficacy which could be used, easily, and at no cost, to crosscheck the given fetal age of a particular fetus for reasonableness, accuracy and efficacy is systematically obviated from all medical evidence and, thereby, from all medical thinking, medical decision-making and medical actions via a government-mandated protocol of evidence-obviated medicine; a protocol of unilateral reliance on ultrasound-based assignments of fetal & gestational age for pregnancies and abortions in Norway, no matter what! This is Directorate of Health's knowledge-obviated, medically & ethically flawed, willfully reckless, grossly negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized and misused Hutchon Method of PDEE).
In stark contrast, Bergen Group's protocol includes all available information, in conjunction with ultrasound data, in the practice of evidence-based medicine to establish the best possible fetal age (and gestational age) for a particular fetus to ensure optimal obstetric & fetal awareness to ensure optimal obstetric & fetal management.
Directorate of Health Were Warned
Directorate of Health were warned or the risks and consequences of their selection of the NCFM eSnurra Group (or Trondheim Group) eSnurra "method" to estimate EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse, for all pregnancies and abortions in Norway. Most vocal in their warnings were Norwegian Society of Gynecology & Obstetrics (Norsk gynekologisk forening) (NGF) who stated Directorate of Health's selection of NCFM eSnurra Group's "method" was "highly reprehensible" and "can be directly dangerous" (see: NGF dissociates from Directorate of Health's recommendation). In addition to NGF, a group of five venerated doctor-scientists who comprise Bergen Group warned Directorate of Health:
Included below are excerpts that make it clear a government-mandated protocol of evidence-obviated medicine has been an NCFM Snurra/eSnurra Group agenda item for decades which was reaffirmed in Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. Following are excerpts which demonstrate a focus on, and an adherence to, a protocol of evidence-obviated medicine with respect to a pregnant woman's key pregnancy dates without her prior, informed, voluntary, explicit consent.
Jakob Nakling & Evidence-based Medicine
In addition to NGF and Bergen Group there are other knowledgeable medical researchers/practitioners such as Jakob Nakling, MD, PhD, Department of Obstetrics and Gynecology, Central Hospital of Lillehammer, Norway, who has published on the topic of evidence-based medicine instead of evidence-obviated medicine with respect to obstetric and fetal medicine. Contrast the research-guided, evidence-based medicine thinking and practices of Jakob Nakling with the flawed thinking embedded within Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine or authority-based medicine (below).
"From the study population of 19,823 deliveries it was possible to answer some of the questions raised at the two consensus conferences of ultrasound in pregnancy.
Moreover, Nakling's work catalyzed an incredibly interesting, informative and pithy 2002 Editorial in Dagens Medisin which addresses the issues raised 13-years later within this public interest disclosure website: LailasCase.com.
Critical Mistakes: EDD & GA Reasonableness Testing
Ironically, it is the LMPD that is used by NCFM eSnurra Group and NCFM-trained doctors and midwives to schedule a pregnant woman for her routine 18wUSE, but as soon as the 18wUSE is scheduled, LMPD/OTPD/SCID and all other key pregnancy dates are obviated, without the pregnant woman's prior, informed, voluntary, explicit consent. Consequently, there is no medical evidence, whatsoever, to test the assigned NCFM eSnurra BPD-based EDD & GA values for reasonableness, accuracy or efficacy, nor is there any medical evidence to identify a potential fetal pathology masked by an inaccurate or grossly inaccurate NCFM eSnurra EDD & GA. As a result, and not surprisingly, some estimates of NCFM eSnurra BPD-based EDD are grossly inaccurate (i.e., < -14 days or > 14 days), which are reported to account for 12.8% of all NCMF eSnurra BPD-based EDD assignments (Figure 3 of NCFM eSnurra Group's Gjessing et al. 2007, p. 23). And, since NCFM eSnurra GA is calculated directly from NCFM eSnurra BPD-based EDD using the equivalent of Naegele's rule, in reverse, GA, too, is grossly inaccurate while, at the same time, a smaller (or larger) than accurately average BPD measurement could be medical evidence of fetal pathology. However, a smaller or larger than accurately average BPD measurement is always assumed to be evidence of an accurately average BPD measurement by NCFM eSnurra Group's eSnurra "method" and, thereby, a correspondingly inaccurate or grossly inaccurate GA is calculated from an NCFM eSnurra BPD-based EDD website, mobile APP or the eSnurra circular slide rule (or pregnancy wheel). Laila's NCFM eSnurra BPD-based GA and fetal age remained grossly inaccurate throughout Laila's entire pregnancy despite Laila & Edward's multiple attempts to correct it. This caused additional critical medical mistakes which were silently and invisibly written off, unattributed, undocumented and unreported, as acceptable collateral damage of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. In fact, Laila's baby's grossly inaccurate GA at birth was included in her national medical birth record at the Medical Birth Registry of Norway (MBRN) without ever having been identified as a grossly inaccurate GA, a critical medical mistake, an adverse event which caused increased medical risks, critical medical mistakes and grievous medical harms to Laila and her baby. This fact alone demonstrates the systemic, institutionalized nature of this insidious problem. In Laila's case, a potentially serious fetal pathology was masked, and remained masked throughout Laila's entire pregnancy, by a grossly inaccurate NCFM eSnurra BPD-based EDD from which a grossly inaccurate GA was calculated. Remember, Laila's factual LMPD/OTPD/SCID-based GA evidence which could have been used to test NCFM eSnurra BPD-based EDD & GA values for reasonableness, accuracy and efficacy, or to unmask potential fetal pathology, had been obviated according to Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra's "method" within a government-mandated protocol of evidence-obviated medicine at the scheduling of the routine 18wUSE, without Laila's prior, informed, voluntary, explicit consent. Ergo, and not surprisingly, increased medical risks and critical medical mistakes were the consequences; consequences which caused grievous harms to Laila and her baby, and other women and their fetuses/babies. Moreover, and again, Directorate of Health had been clearly and explicitly warned by Norway's best medical experts (i.e., NGF and Bergen Group) that critical medical mistakes would be the consequences.
Contrast Directorate of Health and NCFM eSnurra Group's government-mandated protocol of evidence-obviated medicine with the protocol of evidence-based medicine as practiced, promoted and published by Drs. Synnøve Lian Johnsen and Torvid Kiserud, two members of Bergen Group (Terminhjulet or Term wheel), in the excerpt below.
Directorate of Health were warned or the risks and consequences of their selection of the NCFM eSnurra Group (or Trondheim Group) eSnurra "method" to estimate EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse, for all pregnancies and abortions in Norway. Most vocal in their warnings were Norwegian Society of Gynecology & Obstetrics (Norsk gynekologisk forening) (NGF) who stated Directorate of Health's selection of NCFM eSnurra Group's "method" was "highly reprehensible" and "can be directly dangerous" (see: NGF dissociates from Directorate of Health's recommendation). In addition to NGF, a group of five venerated doctor-scientists who comprise Bergen Group warned Directorate of Health:
- "We hold the opinion that this recommendation is medically flawed and that the Directorate has conducted a muddled investigation process."
- "We argue that critical mistakes may follow from the failure to include all available information when fetal age is assessed." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
Included below are excerpts that make it clear a government-mandated protocol of evidence-obviated medicine has been an NCFM Snurra/eSnurra Group agenda item for decades which was reaffirmed in Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. Following are excerpts which demonstrate a focus on, and an adherence to, a protocol of evidence-obviated medicine with respect to a pregnant woman's key pregnancy dates without her prior, informed, voluntary, explicit consent.
- "If the LMP is used only for scheduling of the dating examination, all questions where the length of gestation influences the answer will relate to the ultrasound-based GA/EDD after the examination is performed." (Source: NCFM eSnurra Group member Inger Økland 2012 dr.philos. NTNU Thesis: Biases in second-trimester ultrasound dating related to prediction models and fetal measurements, p.35)
- "It appears evident that the LMP should be used only in the scheduling of the dating scan (Gardosi et al. 1997, Bottomley and Bourne 2009)." (Source: ibid.)
- "Moreover, at least in Europe, it became common practice to use the EDD determined at the ultrasound examination, no matter how ‘certain’ the reported LMP might be (Taipale and Hiilesmaa 2001, Bottomley and Bourne 2009, Verburg et al. 2008b)." (Source: ibid).
- "The model [NCFM eSnurra (i.e., the plagiarized Hutchon Method)] obviates the dependence on last menstrual period found in standard methods for term prediction, and allows an immediate assessment of prediction quality in a population setting." (Source: Ultrasound Obstet Gynecol 2007; 30: 19–27, "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, DOI: 10.1002/uog.4053)
Jakob Nakling & Evidence-based Medicine
In addition to NGF and Bergen Group there are other knowledgeable medical researchers/practitioners such as Jakob Nakling, MD, PhD, Department of Obstetrics and Gynecology, Central Hospital of Lillehammer, Norway, who has published on the topic of evidence-based medicine instead of evidence-obviated medicine with respect to obstetric and fetal medicine. Contrast the research-guided, evidence-based medicine thinking and practices of Jakob Nakling with the flawed thinking embedded within Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine or authority-based medicine (below).
- "Conclusion The biologic variation associated with start of pregnancy is large, and this knowledge has implications for how we should interpret a pregnant woman's information about the LMP. There is no reason to distrust or write off a pregnant woman's report about LMP as unlikely. The large biologic variation explains why reliable information about LMP is not equivalent with reliable information about start of pregnancy [19]. Also, the biologic variation of gestational length is large and the day of spontaneous labour cannot be predicted with high precision. The expected term of delivery should rather be expressed as an interval than a specific day." (Source: "The biologic error in gestational length related to the use of the first day of last menstrual period as a proxy for the start of pregnancy" Jakob Nakling, Harald Buhaug, Bjorn Backe. Early Human Development (2005) 81, 833-839, p. 837) [Note: To avoid the paywall, this publication is include in Jacob Nakling's 2006 NTNU PhD Thesis beginning on PDF-page 44.]
- "Also, I will emphasize the point that the women’s information about LMP is not disregarded or ignored. This information should be respected and may contain valuable information." (Source: Jakob Nakling, 2008 NTNU PhD Thesis (p. 25). "Results and consequences of routine ultrasound screening in pregnancy: A geographic based population study" Norwegian University of Science and Technology, Faculty of Medicine, Department of Laboratory Medicine, Children’s and Women’s Health. ISBN: 82-471-8006-5, ISSN: 1503-8181)
- Thus, we can conclude that gestational age discrepancy is an important risk factor affecting about 7 % of the pregnancies, and this risk factor carries a considerable proportion of perinatal morbidity and mortality. Still, we do not know how to manage pregnant women where the EDDs differ with more than two weeks. If effective 30 interventions were identified this would be an important contribution. This may be an effect of early growth restriction. Routinely, in cases with two weeks discrepancy we do now offer a follow up examination with ultrasound fetometry in week 25. (Source: ibid., p. 29-39)
"From the study population of 19,823 deliveries it was possible to answer some of the questions raised at the two consensus conferences of ultrasound in pregnancy.
- Foetuses that are smaller than expected at the second-trimester ultrasound corresponding to a discrepancy of more than 14 days, have an increased risk for adverse obstetric outcome.
- Expectant management of post term pregnancies allowing pregnancies to continue up to week 43 still carries a risk for perinatal mortality and morbidity, despite intensified observation from week 42+2. The risk increases already from gestational week 41.
- Mid second trimester ultrasound examination in district hospitals can achieve a detection rate of congenital anomalies comparable with tertiary centres, without few false positives that were clinically of minor importance.
- Even when the last menstrual period is reliable, the biological variation of the time from last menstrual period to the real start of pregnancy is substantial. Reliable information about last menstrual period is not equivalent to reliable information about the time of onset of pregnancy. [Ergo, the efficacy of ovulation tests to reduce, even eliminate, this variation.]
- Using the new BPD reference values [Terminhjulet] gives a better prediction of spontaneous labor and provides a more reliable assessment of gestational age than the old method."
Moreover, Nakling's work catalyzed an incredibly interesting, informative and pithy 2002 Editorial in Dagens Medisin which addresses the issues raised 13-years later within this public interest disclosure website: LailasCase.com.
- "Pregnant women's own information about the term must be taken seriously, states a major Norwegian study. - If the ultrasound examination shifts the term two weeks or more, women should be closely monitored. They are at higher risk of various complications, says chief physician Jakob Nakling. Annually this applies to approximately 4000 women."
("Gravides egne opplysninger om termin må tas alvorlig, fastslår en stor norsk studie. - Hvis ultralydundersøkelse forskyver terminen to uker eller mer, bør kvinnene følges nøye opp. De har høyere risiko for ulike komplikasjoner, sier overlege Jakob Nakling. Årlig gjelder dette cirka 4000 kvinner.") - Must apologize "We have looked at the meaning of the term shift for the fetus. It turns out that this group is quite special. The morbidity is higher and there is greater risk of perinatal mortality before, during or immediately after birth," said Jakob Nakling. He has been head doctor at Oppland Central Hospital at Lillehammer and is currently a special adviser to Helse Øst. The study is funded by the Research Council of Norway, and he was a PhD student at the Norwegian University of Science and Technology in Trondheim from 2000 to 2001. We who do ultrasound have been very assertive: "We can best find the term." We must give women an apology and redress because we have been arrogant and superior, says head doctor Nakling."
Må unnskylde - Vi har sett på hvilken betydning terminforskyvning har for fosteret. Det viser seg at denne gruppen er ganske spesiell. Sykeligheten er høyere, , under eller rett etter fødsel, sier Jakob Nakling. Han har vært overlege ved Oppland sentralsykehus på Lillehammer og er for tiden spesialrådgiver i Helse Øst. Studien er finansiert av Norges Forskningsråd, og han var doktorgradsstipendiat ved Norges teknisk-naturvitenskapelige universitet i Trondheim fra 2000 til 2001. - Vi som driver med ultralyd, har vært veldig påståelige: «Vi klarer best å finne terminen». Vi må gi kvinnene unnskyldning og oppreisning for at vi har vært arrogante og overlegne, mener overlege Nakling.
(Source: "Risky to ignore mother's term" ("Risikabelt å overse mors termin") Editorial by Hilde Kari Nylund. Dagens Medisin, Publisert: 2002-10-10 00.00 Skrevet av: Redaktionen)
Critical Mistakes: EDD & GA Reasonableness Testing
Ironically, it is the LMPD that is used by NCFM eSnurra Group and NCFM-trained doctors and midwives to schedule a pregnant woman for her routine 18wUSE, but as soon as the 18wUSE is scheduled, LMPD/OTPD/SCID and all other key pregnancy dates are obviated, without the pregnant woman's prior, informed, voluntary, explicit consent. Consequently, there is no medical evidence, whatsoever, to test the assigned NCFM eSnurra BPD-based EDD & GA values for reasonableness, accuracy or efficacy, nor is there any medical evidence to identify a potential fetal pathology masked by an inaccurate or grossly inaccurate NCFM eSnurra EDD & GA. As a result, and not surprisingly, some estimates of NCFM eSnurra BPD-based EDD are grossly inaccurate (i.e., < -14 days or > 14 days), which are reported to account for 12.8% of all NCMF eSnurra BPD-based EDD assignments (Figure 3 of NCFM eSnurra Group's Gjessing et al. 2007, p. 23). And, since NCFM eSnurra GA is calculated directly from NCFM eSnurra BPD-based EDD using the equivalent of Naegele's rule, in reverse, GA, too, is grossly inaccurate while, at the same time, a smaller (or larger) than accurately average BPD measurement could be medical evidence of fetal pathology. However, a smaller or larger than accurately average BPD measurement is always assumed to be evidence of an accurately average BPD measurement by NCFM eSnurra Group's eSnurra "method" and, thereby, a correspondingly inaccurate or grossly inaccurate GA is calculated from an NCFM eSnurra BPD-based EDD website, mobile APP or the eSnurra circular slide rule (or pregnancy wheel). Laila's NCFM eSnurra BPD-based GA and fetal age remained grossly inaccurate throughout Laila's entire pregnancy despite Laila & Edward's multiple attempts to correct it. This caused additional critical medical mistakes which were silently and invisibly written off, unattributed, undocumented and unreported, as acceptable collateral damage of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. In fact, Laila's baby's grossly inaccurate GA at birth was included in her national medical birth record at the Medical Birth Registry of Norway (MBRN) without ever having been identified as a grossly inaccurate GA, a critical medical mistake, an adverse event which caused increased medical risks, critical medical mistakes and grievous medical harms to Laila and her baby. This fact alone demonstrates the systemic, institutionalized nature of this insidious problem. In Laila's case, a potentially serious fetal pathology was masked, and remained masked throughout Laila's entire pregnancy, by a grossly inaccurate NCFM eSnurra BPD-based EDD from which a grossly inaccurate GA was calculated. Remember, Laila's factual LMPD/OTPD/SCID-based GA evidence which could have been used to test NCFM eSnurra BPD-based EDD & GA values for reasonableness, accuracy and efficacy, or to unmask potential fetal pathology, had been obviated according to Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra's "method" within a government-mandated protocol of evidence-obviated medicine at the scheduling of the routine 18wUSE, without Laila's prior, informed, voluntary, explicit consent. Ergo, and not surprisingly, increased medical risks and critical medical mistakes were the consequences; consequences which caused grievous harms to Laila and her baby, and other women and their fetuses/babies. Moreover, and again, Directorate of Health had been clearly and explicitly warned by Norway's best medical experts (i.e., NGF and Bergen Group) that critical medical mistakes would be the consequences.
Contrast Directorate of Health and NCFM eSnurra Group's government-mandated protocol of evidence-obviated medicine with the protocol of evidence-based medicine as practiced, promoted and published by Drs. Synnøve Lian Johnsen and Torvid Kiserud, two members of Bergen Group (Terminhjulet or Term wheel), in the excerpt below.
- "Pregnancy where there is a large discrepancy (e.g. > 10 days) between EDD based on ultrasound and EDD based on certain last menstrual period, should be perceived as a risk pregnancy." (Source: "Fosterbiometri: Fosteralder, størrelse og vekst - Referanseverdier for ultralydmålinger" Seksjon for fostermedisin & ultralyd, Kvinneklinikken, Haukeland Universitetssykehus og Seksjon for obstetrikk og gynekologi, Institutt for Klinisk Medisin, Universitetet i Bergen, Synnøve Lian Johnsen & Torvid Kiserud, Oktober 2006. p. 42. . ISBN-13:978-82-990918-7-9)
- The American College of Obstetricians and Gynecologists (ACOG)
- American Institute of Ultrasound in Medicine (aium)
- Society for Maternal · Fetal Medicine (SMFM).
(Source: COMMITTEE OPINION Number 700, May 2017. p. 2. Consensus opinion of: 1) The American College of Obstetricians and Gynecologists (ACOG), 2) American Institute of Ultrasound in Medicine (aium) & 3) Society for Maternal - Fetal Medicine)
Strangely, NCFM Snurra Group's Tunón et al. 2000 is cited as reference 13 among the 4 cited references "(11-14)" associated with the excerpt taken from COMMITTEE OPINION Number 700, May 2017. p. 2. Consensus opinion (below).
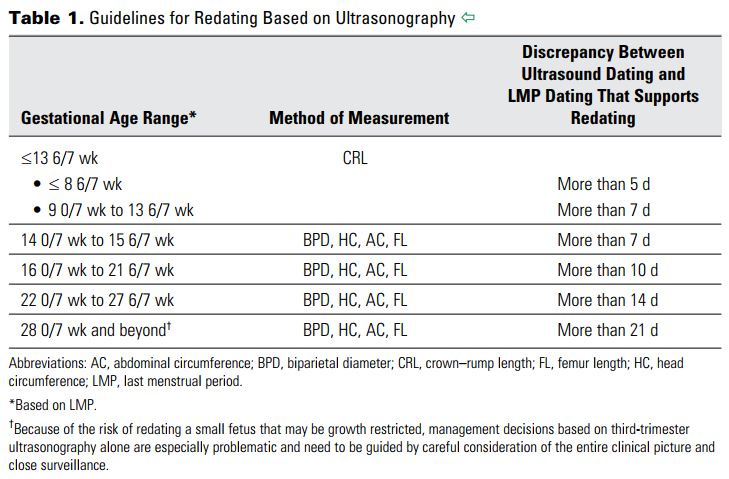
- "Up to and including 13 6/7 weeks of gestation, gestational age assessment based on measurement of the crown-rump length (CRL) has an accuracy of +/- 5-7 days (11-14)." [Note: Reference: 13. Tunon K, Eik-Nes SH, Grottum P, Von During V, Kahn JA. Gestational age in pregnancies conceived after in vitro fertilization: a comparison between age assessed from oocyte retrieval, crown–rump length and biparietal diameter. Ultrasound Obstet Gynecol 2000;15:41–6. [PubMed] [Full Text]]
Moreover, the document "Methods for Estimating the Due Date" ACOG Committee Opinion Number 700, May 2017 cited and referenced Wisser et al. 1994 as reference 16 in the excerpt below.
- "Measurements of the CRL are more accurate the earlier in the first trimester that ultrasonography is performed (11, 15–18)." [Note: Reference: 16. Wisser J, Dirschedl P, Krone S. Estimation of gestational age by transvaginal sonographic measurement of greatest embryonic length in dated human embryos. Ultrasound Obstet Gynecol 1994;4:457–62. [PubMed] [Full Text]]
- "The measurement of greatest length was preferred to crown-rump length [CRL] because of difficulties in defining the cranial reference point in the embryo before 42 days after the last menstrual period 17." (p. 458) (Source: "Estimation of gestational age by transvaginal sonographic measurement of greatest embryonic length in dated human embryos" Wisser J, Dirschedl P, Krone S. Ultrasound Obstet Gynecol, 1994)
- "Ultrasound measurement of the embryo or fetus in the first trimester (up to and including 13 6/7 weeks of gestation) is the most accurate method to establish or confirm gestational age (3, 4, 7–10)." [Note: Reference: 7. Taipale P, Hiilesmaa V. Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol 2001;97:189–94. [PubMed] [Obstetrics & Gynecology]]
See: Academic Ethos > NTNU & NCFM ETHOS
Critical Medical Mistakes Summary
There were 3 fundamental critical medical mistakes in Laila's case:
Critical Medical Mistakes: Just How Critical?
The excerpt below from Tunón et al. 1999a (p. 21), authored by NCFM Snurra Group members K. Tunón, S. H. Eik-Nes and P. Grøttum, stated a BPD at 18-weeks that is at least 6 mm (or 14%) smaller than it should be was "probably outside the physiological range, and cannot be considered compatible with continuous normal development."
There were 3 fundamental critical medical mistakes in Laila's case:
- Laila's key pregnancy dates, including her combined, fully corroborating, factual LMPD/OTPD/SCID, were obviated, without Laila's prior, informed, voluntary, explicit consent, in accordance with Directorate of Health's selection and implementtion of NCFM eSnurra Group's eSnurra "method" (i.e., the appropriated, plagiarized, intentionally misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine to estimate EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse, for all pregnancies and abortions in Norway.
- Without Laila's combined, fully corroborating, factual LMPD/OTPD/SCID for reasonableness testing, NCFM eSnurra Group's "method" used the measurements from the 18wUSE to assign grossly inaccurate EDD & GA values to Laila's pregnancy, with BPD-based eSnurra EDD & GA lagging 15 and 12 days, respectively, behind Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD & GA. Unfortunately, NCFM eSnurra Group's "method" relied exclusively on the problematic, unreliable biparietal diameter (BPD).
- Due to the government-mandated, unilateral reliance on the grossly inaccurate NCFM eSnurra BPD-based EDD & GA, Laila's baby was not turned from breech to vertex in time for a normal deliver and, therefore, Laila was denied the opportunity to: a) have the natural delivery she had always wanted and planned, b) avoid an unnecessary, unwanted Cesarean section surgery delivery with inherent complications and c) Laila and her baby were denied their respective, many natural health benefits infused by a normal, natural delivery.
Critical Medical Mistakes: Just How Critical?
The excerpt below from Tunón et al. 1999a (p. 21), authored by NCFM Snurra Group members K. Tunón, S. H. Eik-Nes and P. Grøttum, stated a BPD at 18-weeks that is at least 6 mm (or 14%) smaller than it should be was "probably outside the physiological range, and cannot be considered compatible with continuous normal development."
- "However, at 18 weeks an early growth restriction that results in changing the estimated day of delivery to a date 2-3 weeks later in accordance with the ultrasound estimate means that the BPD is at least 6 mm smaller than it should be, i.e. the width of the BPD is already 14% less than expected for the age. This indicates an extensive restriction that is probably outside the physiological range, and cannot be considered compatible with continuous normal development. Such a severe and highly pathological growth restriction will be most likely to continue and make itself manifest later in pregnancy even if it is (mistakenly) corrected for at 18 weeks." (Source: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" K. Tunon, S. H. Eik-Nes and P. Grattum, Ultrasound Obstet Gynecol 1999;14:17-22, p. 21)
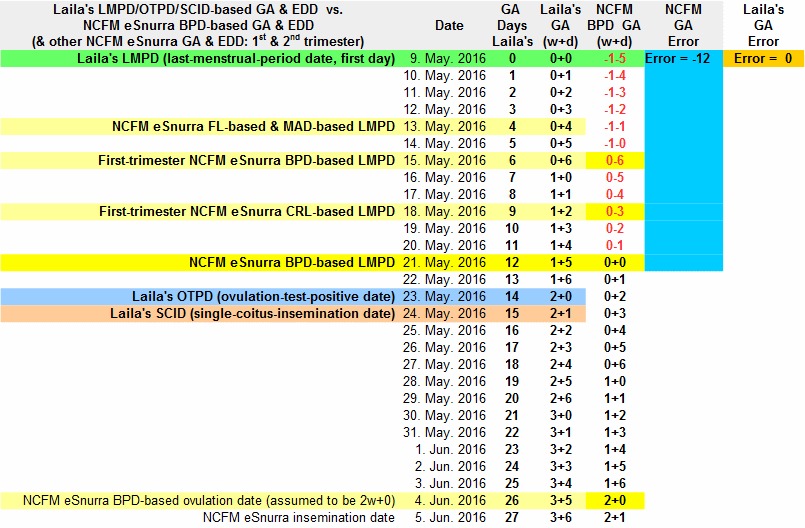
The image below was taken from Laila's Pregnancy Spreadsheet. It shows the beginning of Laila's pregnancy from 2 different temporal frames of reference based on:
- Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD temporal frame of reference; the only more accurate method of establishing the beginning of Laila's pregnancy would be if she were to have had an in vitro fertilization date (IVFD)
- the grossly inaccurate NCFM eSnurra BPD-based GA & EDD; using the problematic, unreliable BPD measurement instead of the more robust, 2-spacial-dimensions head circumference (HC) measurement
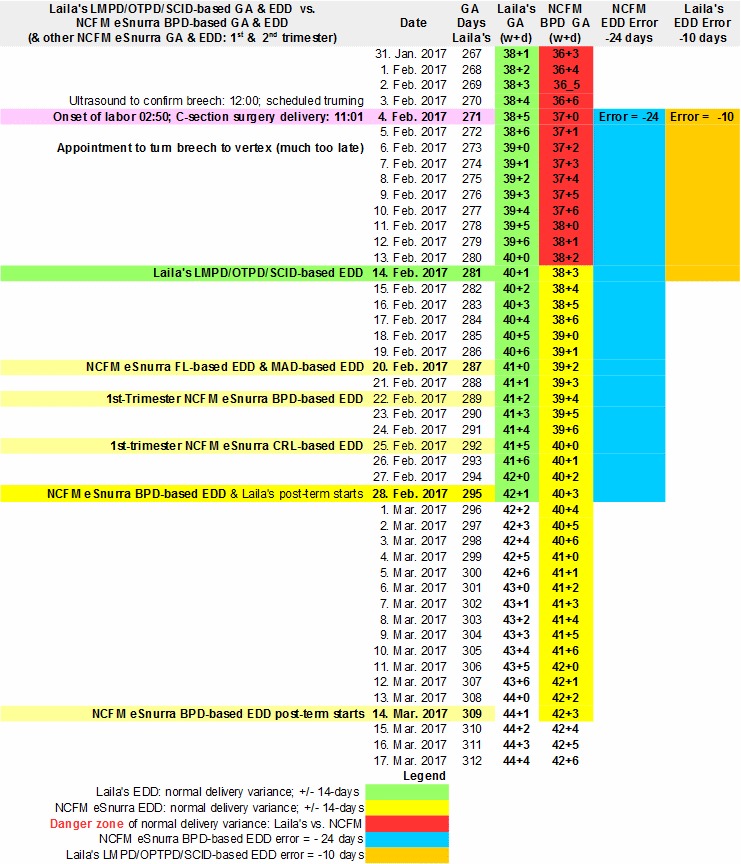
The image included below was also taken from Laila's Pregnancy Spreadsheet. It shows the end of Laila's pregnancy from 2 different temporal frames of reference based on:
- Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD temporal frame of reference; the only more accurate method of establishing the beginning of Laila's pregnancy would be if she were to have had an in vitro fertilization date (IVFD)
- the grossly inaccurate NCFM eSnurra BPD-based GA & EDD; using the problematic, unreliable BPD measurement instead of the more robust, 2-spacial-dimensions head circumference (HC) measurement
Critical Medical Mistakes: Laila Delivered Early
First, one must fully appreciate the phrase "even if it is (mistakenly) corrected for at 18 weeks." in the excerpt above. This phrase alone speaks volumes. It makes it clear that there is a presupposition that a woman's factual, key pregnancy dates always need to be "corrected" with ultrasound GA & EDD values when the phrase which should be used is "obviated and replaced." The word "corrected" (and this is not a translation issue) requires a comparison with a reference standard for truth or actual, such as IVFD-based GA or OTPD-based GA, both of which are used as GA reference standards in research studies. This "(mistakenly) corrected" thinking is found among the conditioned minds in which confirmation bias has already built a warm, cozy nest to enable institutionalized doublethink to operate at maximum capacity. To take this point further, consider the statement of Laila's midwife in the excerpt below.
Moreover, Laila was breech for her entire pregnancy and this was known to all. Consequently, the ultrasound exam was scheduled much too late to: 1) confirm breech and 2) upon confirmation of breech, schedule the routine manual turning of Laila's baby from breech to vertex for a natural delivery. Laila & Edward emphatically and repeatedly warned Laila's midwife & doctor that the ultrasound exam and the necessary turning procedure had been scheduled much too late and that it should be moved up because Laila's factual LMPD/OTPD/SCID GA & EDD put the scheduled ultrasound date and turning procedure under the umbrella of normal variance of birth/delivery for Laila's factual LMPD/OTPD/SCID-based EDD. However, there was no discussing nor arguing this point with either logic or basic gestational mathematics because all discussions and arguments with Laila's medical professionals ended with either "this is how we do it in Norway" or "this is The Rule" or the Norwegian guidelines were cited (i.e., the mandate). At the ultrasound exam to confirm breech, Laila was confirmed breech (big surprise, one could easily feel Laila's baby's head) and the routine turning procedure was scheduled for the following Monday, 3 days later. However, what Laila's medical professionals had been warned by Laila & Edward, repeatedly, could happen, happened. Laila went into labor 15-hours after her breech-confirming ultrasound exam, still breech, and with the routine turning of her baby from breech to vertex no longer possible. Consequently, Laila was forced onto the horns of a dilemma. She had to choose either of two unwanted, unfavorable alternatives: 1) a risky, breech delivery or 2) a Cesarean section surgery delivery. However, a required hospital CT-scan eliminated Laila's dilemma, leaving Laila with no choice; Laila had to endure a Cesarean section surgery delivery because the CT-scan established Laila's pelvis: 1) met all the criteria for a safe, normal, vertex, vaginal delivery and 2) did not meet all the criteria for a safe, breech, vaginal delivery (breech delivery safe?). As a result, a Cesarean section surgery team (an excellent team) delivered Laila's baby, Helen; and, Laila, Helen & Edward spent 11 days in hospital while Laila endured a cascade of Cesarean section complications including postpartum preeclampsia and other complications while Helen's head looked like a football, an American football, elongated or dolichocephalic (more commonly "long head" or "breech head"), the direct result of an unnecessary, unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head which could easily have been a more serious fetal pathology.
Critical Medical Mistakes: Laila as Post-term (hypothetical)
Laila went into labor early under the umbrella of normal variance according to her factual LMPD/OTPD/SCID-based GA & EDD, but Laila was technically defined as preterm by NCFM eSnurra BPD-based EDD & GA. However, consider if Laila were to have been post-term instead of early. Since NCFM eSnurra BPD-based EDD was lagging Laila's factual LMPD/OTPD-based EDD by 14 days, how many days would Laila's medical professionals have let her go into post-term gestation while believing, without any doubts, because doubts of NCFM eSnurra BPD-based EDD & GA are not allowed? Remember, all the medical evidence needed to test NCFM eSnurra BPD-based EDD & GA for reasonableness, errors or efficacy had been obviated at the scheduling of Laila's routine 18wUSE, without Laila's prior, informed, voluntary, explicit consent. The start of post-term as defined by NCFM eSnurra is EDD + 14 days. One could reasonably hypothesize Laila would have been allowed to go into post-term for 3 days before she would have been induced at what would have been NCFM eSnurra BPD-based GA = 42w+6, but relative to Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA = 44w+4 (or 312 days) of "real" gestation time, or (312 - 280) = 32 days, more than 1 month past her factual LMPD/OTPD/SCID-based EDD before inducing Laila into labor would have been considered. The conclusion in the Norwegian study Nakling et al. 2006 makes this point.
Critical Medical Mistakes: Abortion (hypothetical scenario)
Hypothetically, consider if Laila were to have needed or wanted an abortion and assume she were to have had the very same grossly inaccurate NCFM eSnurra BPD-based GA lagging her combined, fully corroborating, factual LMPD/OTPD/SCID-based GA by 12 days; and, with Laila knowing this 12-day discrepancy to be a stone-cold fact. Would Laila be committing a crime, a felony, for knowingly having an abortion at 23w+4, 12 days over the legal limit in Norway, if all of her medical professionals were assuring her they were absolutely certain she was not over the legal limit of 21-weeks + 6 days (grossly wrong) because the NCFM eSnurra BPD-based EDD (grossly inaccurate) used to calculate the GA medical age evidence (grossly inaccurate) for her abortion's legality indicated she was at the legal limit, not over it (grossly wrong) and, therefore, her abortion would be completely legal ? Again, in this hypothetical situation, with the very same grossly inaccurate NCFM eSnurra BPD-based GA, Laila knows for a stone-cold fact her pregnancy has exceeded Norway's legal limit of 21w+6 and that "the statutory requirements for such an operation have not been fulfilled" because her combined, fully corroborating, factual LMPD/OTPD/SCID-based GA is 23w+4, 12 days (or 1w+5) over the legal limit of 21w+6 in Norway. Now, consider the Norwegian law (below).
What is there to stop this same scenario from happening today or tomorrow? The answer is: Nothing, yet. Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Right Evidence, Wrong Evidence Messenger
Usually, at least 2 fetal metrics, the biparietal diameter (BPD) and the femur length (FL), are measured via ultrasound for NCFM eSnurra Group's "method" to estimate and calculate two separate sets of NCFM eSnurra EDD & GA values: NCFM eSnurra BPD-based EDD & GA and NCFM eSnurra FL-based EDD & GA. On the date of Laila's routine 18wUSE, Laila's factual LMPD/OTPD/SCID-based GA was 19w+4d (or 137 days), when the BPD and FL fetal metrics were measured: BPD = 41 mm and FL = 29 mm, from which NCFM eSnurra BPD-based EDD = 28.02.2017 and NCFM eSnurra FL-based EDD = 20.02.2017 were estimated and, therefrom, by using Naegele's rule, in reverse, NCFM eSnurra BPD-based GA = 17w+6d (or 125 days) and NCFM eSnurra FL-based GA = 19w+0d (or 133 days) were calculated, respectively. There was an obvious 8 day discrepancy between NCFM eSnurra BPD-based GA and NCFM eSnurra FL-based GA. This 8 day discrepancy was ignored by NCFM, Laila's doctor and her midwife, likely due to systemic, institutionalized confirmation bias and doublethink because the problematic, unreliable BPD measurement is NCFM eSnurra Group's premier, preferred predictor of EDD and, therefrom, their calculated GA, using Naegele's rule, in reverse. So, even when the 8 day discrepancy was pointed out by Laila & Edward, a discrepancy based, entirely, on NCFM eSnurra-based FL evidence, NCFM eSnurra Group's own evidence, Laila & Edward were ignored, thus confirming Directorate of Health's government-mandated protocol of evidence-obviated medicine not only obviates non-NCFM eSnurra evidence, but also obviates NCFM's own evidence when delivered by non-NCFM eSnurra messengers, i.e., Laila & Edward.
Dimensions of the BPD Problem
It is well known, internationally, BPD is a problematic, unreliable predictor of EDD and GA. The more robust head circumference (HC) should be used instead. Moreover, using HC instead of BPD is patently intuitive given the fact BPD is a diameter, a linear measurement in 1 spacial dimension, while HC is a measurement, which includes 2 perpendicular diameters in 2 spacial dimensions. Most ultrasound machines have a digital ellipse function which sonographers use to fit a digital ellipse to the contour of the fetal skull, otherwise 2 diameters are measured (i.e., BPD & OFD). Consequently, because HC is a measurement in 2 spacial dimensions it will always included more information about fetal head size than a BPD measurement in 1 spacial dimension. Additionally, HC is nearly insensitive to fetal head shape while BPD is highly sensitive to head shape and, therefore, is prone to generate grossly inaccurate EDD & GA values for non-standard head shapes and sizes, e.g., dolichocephaly and SGA, respectively. Moreover, if HC diameters (i.e., BPD & OFD) are measured, they can be used in a ratio to calculate a cephalic index (CI = BPD/OFD x 100) to provide information about head shape which can be used to identify a grossly inaccurate NCFM eSnurra BPD-based EDD & GA and to screen for fetal pathology, which begs the question: Why doesn't NCFM eSnurra Group measure the OFD to compute HC, or to at least calculate a CI to ensure BPD is not used to estimate a grossly inaccurate EDD & GA which is then assigned, irretrievably, as the "official" EDD & GA to a pregnancy?
LMPD: Virtual vs. Real
NCFM eSnurra GA is calculated by using Naegele's rule in reverse. Subtract 283 days from the NCFM eSnurra EDD date to calculate a virtual LMPD (GA day 0, or 0w+0). Or, to calculate GA on the date of the ultrasound exam, simply subtract the NCFM-eSnurra estimated number of days remaining on the ultrasound date to delivery date from 283 days. So, 283 days from what? The answer, of course, is a virtual LMPD. Consequently, all ultrasound-based NCFM eSnurra calculated GA values are indirect estimates of LMPD. However, Laila knew her factual LMPD (09.05.2016), because Laila had documented this date when it presented in her pregnancy spreadsheet and her LMPD fully corroborated her factual OTPD. Consequently, NCFM eSnurra could not have calculated Laila's LMPD (real or virtual) from an estimated NCFM eSnurra BPD-based EDD any more accurately than Laila's factual LMPD. And, with the addition of Laila's SCID for a combined, full corroborating, factual LMPD/OTPD/SCID, the only method that could have been more accurate at establishing the beginning of Laila's pregnancy (i.e., in hours, not days) would have been if Laila were to have had an in vitro fertilization date (IVFD). This is a fact, not an opinion.
Corrected from Right to Wrong via Doublethink
If NCFM eSnurra BPD-based EDD & GA were to have been believed, all of Laila's factual, spreadsheet-recorded dates had to be wrong and, therefore, "corrected" by pushing all of Laila's key pregnancy dates forward (to the future) 12 days (or 1w+5) to conform with the grossly inaccurate NCFM eSnurra BPD-based EDD & GA temporal frame of reverence assigned to Laila's pregnancy; a grossly inaccurate temporal frame of reference. This is where it became indisputably clear Norwegian Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Groups "method" within a government-mandated protocol of evidence-obviated medicine required Laila's medical professionals to fully engage in doublethink. Norway's medical professionals must, via government-mandate, use NCFM eSnurra EDD & GA, exclusively, without question, no matter what fact-based evidence of proven efficacy is used to prove NCFM eSnurra EDD & GA values to be grossly inaccurate. None of Laila's medical professionals would listen to the arguments for using Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD as a reasonableness test for the NCFM eSnurra BPD-based EDD & GA assigned to Laila's pregnancy. Consequently, and despite repeated warnings with fact-based evidence, the routine procedure to turn Laila's baby from breech to vertex, it time, before the onset of labor, had been scheduled much too late, thus requiring Laila to endure an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications, and her baby to endure an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head which easily could have been a more serious fetal pathology.
BPD & Confirmation Bias with Doublethink
Interestingly, a third fetal metric, the mean abdominal diameter (MAD), was measured during Laila's 18wUSE on 23.09.2016, MAD = 46 mm (yellow highlighted values in the "Fetal Metric Measurements with GA & EDD" table, below), and was included in the same NCFM eSnurra ultrasound report along with the BPD and FL measurements. However, and strangely, the normally associated NCFM eSnurra EDD & GA values for MAD were withheld from the ultrasound report. A Google Search on the words "eSnurra" and "MAD" identified the NCFM eSnurra Group's website with NCFM eSnurra EDD & GA calculators and lookup tables, which begs the question: Why were the NCFM eSnurra MAD-based EDD & GA values withheld from the ultrasound report when these values were available to the public on the NCFM eSnurra Group's website? The MAD table on the NCFM eSnurra website showed 2 entries for MAD = 41 mm: 1) 150.4 days-remaining and 2) GA estimate of 19w+0d (or 133 days), which was then calculated into a MAD-based eSnurra EDD of 20.02.2017 = (ultrasound date + 150.4 days) = (23.09.2016 + 150.4 days), which, maybe not surprisingly, turned out to be the exact same EDD as NCFM eSnurra FL-based EDD. Consequently, both the NCFM eSnurra FL-based EDD and MAD-based EDD were the exact same date; and, both only lagged Laila's factual LMPD/OTPD/SCID-based EDD by 4 days, well under the normal variance umbrella of Laila's LMPD/OTPD/SCID-based EDD. Even if MAD were not to have been regarded as a particularly strong predictor/estimator, it had to be acknowledge that 2 separate measurements of 2 separate fetal metrics, FL & MAD, converging on the same EDD date and, consequently, the same calculated GA, would be overwhelming and compelling medical evidence that Laila's "official" NCFM eSnurra BPD-based EDD was grossly inaccurate, problematic and unreliable. In fact the 12 day lag and 4 day lag in NCFM eSnurra BPD-based GA and NCFM eSnurra FL & MAD-based GA, respectively, relative to Laila's LMPD/OTPD/SCID-based GA were important medical evidence of potential fetal pathology, such as a fetal growth restriction/malformation of Laila's baby's head or SGA or much worse. What should have been crystal clear is that NCFM eSnurra BPD-based EDD & GA were evidence of fetal pathology and not evidence of an accurate EDD & GA. This is a textbook example of confirmation bias (i.e., the tendency to interpret new evidence as confirmation of one's existing beliefs or theories). Consequently, and obviously, the "official" NCFM eSnurra BPD-based EDD of 28.02.20 was grossly inaccurate and, therefor, so was the NCFM eSnurra GA calculated from the grossly inaccurate EDD using the equivalent of Naegele's rule, in reverse. Therefore, it was clear NCFM eSnurra EDD & GA should not have been trusted in medical thinking, medical decision-making and medical actions; medical actions such as scheduling time-constrained medical procedures, especially time-critical procedures such as the turning of a fetus/baby from breech to vertex, in time, for normal delivery before the onset of labor to prevent an unwanted, unnecessary, risky breech delivery or an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications and, a baby who endured an unidentified, prolonged, undiagnosed, untreated fetal pathology such as an FGR/malformation of the head or much worse. But, again, it was confirmation bias for NCFM eSnurra BPD-based EDD & GA that kept Laila's medical professionals from accepting evidence that proved NCFM eSnurra BPD-based EDD & GA were grossly inaccurate when compared to NCFM eSnurra FL- & MAD-based EDD & GA and, therefore, the NCFM eSnurra BPD-based EDD & GA should have been identified as evidence of fetal pathology, not evidence of an accurately average EDD & GA. Again, no logic was allowed to penetrate Directorate of Health's 2014 Recommendation of evidence-obviated medicine, "the rule" of NCFM eSnurra Group or the oft-cited Norwegian national guidelines (i.e., the mandate). Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Symphysis-fundus Height (SFH): Evidence of grossly inaccurate NCFM eSnurra BPD-based EDD & GA
Laila's midwife measured Laila's SFH at each appointment beginning 27.10.2016 (Laila's GA = 24+3) for a total of 6 measurements which were plotted against NCFM eSnurra BPD-based GA (below). Notice how Laila's GA vs. SFH plots were tracking above the 90th centile, with 2 measurement above the 97.5 centile. This was evidence of:
First, one must fully appreciate the phrase "even if it is (mistakenly) corrected for at 18 weeks." in the excerpt above. This phrase alone speaks volumes. It makes it clear that there is a presupposition that a woman's factual, key pregnancy dates always need to be "corrected" with ultrasound GA & EDD values when the phrase which should be used is "obviated and replaced." The word "corrected" (and this is not a translation issue) requires a comparison with a reference standard for truth or actual, such as IVFD-based GA or OTPD-based GA, both of which are used as GA reference standards in research studies. This "(mistakenly) corrected" thinking is found among the conditioned minds in which confirmation bias has already built a warm, cozy nest to enable institutionalized doublethink to operate at maximum capacity. To take this point further, consider the statement of Laila's midwife in the excerpt below.
- Excerpts from the midwife's statements
"There was some dissent about the term date. The first day of the last menstrual period is usually assumed, but is corrected by ultrasound in week 18. This is in accordance with the guidelines for pregnancy care in Norway." ("Det er en viss dissens om termindato. Siste mens første dag legges til grunn vanligvis, men korrigeres etter ultralyd i uke 18. Dette er etter retningslinjene for vangerskapsomsorg i Norge.") (Source: Correspondence from Røros kommune, Kommuneoverlegen, 07.04.2017, to Laila & Edward) - While Laila was recovering from her postpartum preeclampsia and Cesarean section surgery complications at the Tynset Hospital Fødestua, Laila's midwife paid Laila an unexpected visit. Laila's midwife was asked: given what she knows now, that NCFM eSnurra BPD-based EDD & GA were grossly inaccurate relative to Laila's factual key pregnancy dates (i.e., Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD) and given that this caused increased medical risks, critical medical mistakes and grievous medical harms to Laila and her baby, what would she do if she were presented with the same set of circumstances and evidence in the future. Laila's midwife replied, unhesitatingly, "I would follow the rule." When asked if this meant doing the exact same thing, she replied in the affirmative. After Laila & Edward exchanged mouths-agape looks, the question was repeated, more fully, to ensure it had been completely understood. Unfortunately, the question had been completely understood. The midwife was then asked if she believed Laila's key pregnancy dates were indeed factual. The midwife replied, unhesitatingly, in the affirmative. Ergo, the midwife was fully engaged in doublethink (defintion below). Laila's midwife, doctor, ultrasound technicians and NCFM specialists had collectively executed the government-mandated protocol of evidence-obviated medicine exactly as they had been told, taught and trained. Moreover, they confirmed they would do the same thing again given the same scenario and evidence, thereby causing another unnecessary case of increased medical risks, critical medical mistakes and grievous medical harms. Moreover, and as if somehow to console Laila, the midwife stated, "This happens sometimes." The midwife went on to tell Laila that she was not the only person for whom this has happened. Again, Laila & Edward exchanged mouths-agape looks. The midwife was completely oblivious to the fact that in the process of making her apparent misery-loves-company-consolation statement, she was making Laila & Edward's argument for them. This serves as but one example of the level of inculcation into government-mandated doublethink which is used to silently and invisibly relegate unnecessary, easily preventable (and at no additional cost) critical medical mistakes and grievous medical harms as acceptable collateral damage to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation.
- On a prior occasion in the midwife's office, the midwife stated because she had been employed by NCFM in Trondheim for 6 years she knew for a fact NCFM would not change the schedule for the turning of Laila's baby from breech to vertex based on Laila's factual, key pregnancy dates. Again, doublethink had been fully engaged by the midwife to the point where she flat-out refused to communicate the evidence of Laila's "official," assigned NCFM eSnurra BPD-based EDD and, therefrom, calculated GA lagging Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD & GA by 14 and 12 days, respectively.
- For a doublethink memory refresher: "DOUBLETHINK means the power of holding two contradictory beliefs in one’s mind simultaneously, and accepting both of them. The Party intellectual knows in which direction his memories must be altered; he therefore knows that he is playing tricks with reality; but by the exercise of DOUBLETHINK he also satisfies himself that reality is not violated. The process has to be conscious, or it would not be carried out with sufficient precision, but it also has to be unconscious, or it would bring with it a feeling of falsity and hence of guilt" (Source: George Orwell, "1984," Part Two, Chapter 9)
Moreover, Laila was breech for her entire pregnancy and this was known to all. Consequently, the ultrasound exam was scheduled much too late to: 1) confirm breech and 2) upon confirmation of breech, schedule the routine manual turning of Laila's baby from breech to vertex for a natural delivery. Laila & Edward emphatically and repeatedly warned Laila's midwife & doctor that the ultrasound exam and the necessary turning procedure had been scheduled much too late and that it should be moved up because Laila's factual LMPD/OTPD/SCID GA & EDD put the scheduled ultrasound date and turning procedure under the umbrella of normal variance of birth/delivery for Laila's factual LMPD/OTPD/SCID-based EDD. However, there was no discussing nor arguing this point with either logic or basic gestational mathematics because all discussions and arguments with Laila's medical professionals ended with either "this is how we do it in Norway" or "this is The Rule" or the Norwegian guidelines were cited (i.e., the mandate). At the ultrasound exam to confirm breech, Laila was confirmed breech (big surprise, one could easily feel Laila's baby's head) and the routine turning procedure was scheduled for the following Monday, 3 days later. However, what Laila's medical professionals had been warned by Laila & Edward, repeatedly, could happen, happened. Laila went into labor 15-hours after her breech-confirming ultrasound exam, still breech, and with the routine turning of her baby from breech to vertex no longer possible. Consequently, Laila was forced onto the horns of a dilemma. She had to choose either of two unwanted, unfavorable alternatives: 1) a risky, breech delivery or 2) a Cesarean section surgery delivery. However, a required hospital CT-scan eliminated Laila's dilemma, leaving Laila with no choice; Laila had to endure a Cesarean section surgery delivery because the CT-scan established Laila's pelvis: 1) met all the criteria for a safe, normal, vertex, vaginal delivery and 2) did not meet all the criteria for a safe, breech, vaginal delivery (breech delivery safe?). As a result, a Cesarean section surgery team (an excellent team) delivered Laila's baby, Helen; and, Laila, Helen & Edward spent 11 days in hospital while Laila endured a cascade of Cesarean section complications including postpartum preeclampsia and other complications while Helen's head looked like a football, an American football, elongated or dolichocephalic (more commonly "long head" or "breech head"), the direct result of an unnecessary, unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head which could easily have been a more serious fetal pathology.
- "CONCLUSION: Slow growth of the fetal biparietal diameter between the first and second trimesters of pregnancy is a strong predictor of perinatal death before 34 weeks." (Source: "Early fetal size and growth as predictors of adverse outcome" Pedersen NG, Figueras F, Wøjdemann KR, Tabor A, Gardosi J. Obstet Gynecol. 2008 Oct;112(4):765-71. doi: 10.1097/AOG.0b013e318187d034.)
Critical Medical Mistakes: Laila as Post-term (hypothetical)
Laila went into labor early under the umbrella of normal variance according to her factual LMPD/OTPD/SCID-based GA & EDD, but Laila was technically defined as preterm by NCFM eSnurra BPD-based EDD & GA. However, consider if Laila were to have been post-term instead of early. Since NCFM eSnurra BPD-based EDD was lagging Laila's factual LMPD/OTPD-based EDD by 14 days, how many days would Laila's medical professionals have let her go into post-term gestation while believing, without any doubts, because doubts of NCFM eSnurra BPD-based EDD & GA are not allowed? Remember, all the medical evidence needed to test NCFM eSnurra BPD-based EDD & GA for reasonableness, errors or efficacy had been obviated at the scheduling of Laila's routine 18wUSE, without Laila's prior, informed, voluntary, explicit consent. The start of post-term as defined by NCFM eSnurra is EDD + 14 days. One could reasonably hypothesize Laila would have been allowed to go into post-term for 3 days before she would have been induced at what would have been NCFM eSnurra BPD-based GA = 42w+6, but relative to Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA = 44w+4 (or 312 days) of "real" gestation time, or (312 - 280) = 32 days, more than 1 month past her factual LMPD/OTPD/SCID-based EDD before inducing Laila into labor would have been considered. The conclusion in the Norwegian study Nakling et al. 2006 makes this point.
- "Conclusions Our results indicate that expectant management of post-term pregnancies allowing pregnancies to continue up to week 43 carries a risk for perinatal mortality and morbidity." (Source: "Pregnancy risk increases from 41 weeks of gestation" Jakob Nakling, Bjørn Backe. Acta Obstetrica et Gynecolobica Scandinavica, Volume 85, Issue 6, June 2006, Pages 663–668. p. 663. DOI: 10.1080/00016340500543733)
- "Our data emphasize the importance of identifying the growth-restricted infants in the prolonged and post-term phase of pregnancy due to their increased perinatal mortality risk. However, one of the most important clinical implications of our study is that these growth restricted infants should probably not have their gestational age determined solely by ultrasound." (Source: "Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study" Nils-Halvdan Morken, Kari Klungsøyr and Rolv Skjaerven. BMC Pregnancy and Childbirth 2014 14:172. https://doi.org/10.1186/1471-2393-14-172. Received: 20 January 2014, Accepted: 7 May 2014, Published: 22 May 2014)
- "In cases of early growth restriction, gestational age may be underestimated, leading to misclassification of size at birth (24). Data from the Iowa Health in Pregnancy Study indicate an underestimation of small-for-gestational-age (SGA) births by 13% when ultrasound-based pregnancy dating is used (25). An underestimation of gestational age could also lead to a delay in induction of pregnancies that have entered the post-term period, which could adversely affect perinatal and neonatal mortality (21,26). Misclassification of gestational age is expected to be more pronounced when ultrasound dating is performed in the second trimester, at which time fetal growth differences are even greater than in the first trimester." (Source: "Systematic misclassification of gestational age by ultrasound biometry: implications for clinical practice and research methodology in the Nordic countries" ALKISTIS SKALKIDOU, MERIT KULLINGER, MARIOS K. GEORGAKIS , HELLE KIELER & ULRIK S. KESMODEL. Acta Obstetricia et Gynecologica Scandinavica 97 (2018) 440–444. SPECIAL THEMED ISSUE: Methodology in Clinical Epidemiological Research in Obstetrics and Gynecology, April 2018. DOI: 10.1111/aogs.13300. Received: 18 December 2017 Accepted: 12 January 2018)
Critical Medical Mistakes: Abortion (hypothetical scenario)
Hypothetically, consider if Laila were to have needed or wanted an abortion and assume she were to have had the very same grossly inaccurate NCFM eSnurra BPD-based GA lagging her combined, fully corroborating, factual LMPD/OTPD/SCID-based GA by 12 days; and, with Laila knowing this 12-day discrepancy to be a stone-cold fact. Would Laila be committing a crime, a felony, for knowingly having an abortion at 23w+4, 12 days over the legal limit in Norway, if all of her medical professionals were assuring her they were absolutely certain she was not over the legal limit of 21-weeks + 6 days (grossly wrong) because the NCFM eSnurra BPD-based EDD (grossly inaccurate) used to calculate the GA medical age evidence (grossly inaccurate) for her abortion's legality indicated she was at the legal limit, not over it (grossly wrong) and, therefore, her abortion would be completely legal ? Again, in this hypothetical situation, with the very same grossly inaccurate NCFM eSnurra BPD-based GA, Laila knows for a stone-cold fact her pregnancy has exceeded Norway's legal limit of 21w+6 and that "the statutory requirements for such an operation have not been fulfilled" because her combined, fully corroborating, factual LMPD/OTPD/SCID-based GA is 23w+4, 12 days (or 1w+5) over the legal limit of 21w+6 in Norway. Now, consider the Norwegian law (below).
- The General Civil Penal Code
"Chapter 22. Felonies against another person's life, body and health
Section 245. Any person who terminates a pregnancy, or who aids and abets thereto, when the statutory requirements for such an operation have not been fulfilled, or an administrative decision for such termination has not been made by any person authorized to do so, is guilty of criminal abortion and shall be liable to imprisonment for a term not exceeding three years. If the act is committed for the purpose of gain or under especially aggravating circumstances, the penalty shall be imprisonment for a term not exceeding six years. If the offender has acted without the woman's consent, imprisonment for a term not exceeding 15 years shall be imposed, but not exceeding 21 years if she dies as a result of the felony.
The penal provision in the first sentence of the first paragraph shall not apply to women who themselves terminate their own pregnancy or aid and abet thereto." (Source: "Act of 22 May 1902 No. 10, The General Civil Penal Code" With subsequent amendments, the latest mady by Act of 21 December 2005 No. 131. Det Kongelige Justis- Og Politidepartment, Ministry of Justice and the Police. p. 90)
- The General Civil Penal Code
"Part I. General Provisions
Introductory Provisions
Section 4. Wherever this code uses the word act, it thereby also includes omission to act unless it is otherwise expressly provided or evident from the context.: (Source: ibid., p. 6)
What is there to stop this same scenario from happening today or tomorrow? The answer is: Nothing, yet. Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Right Evidence, Wrong Evidence Messenger
Usually, at least 2 fetal metrics, the biparietal diameter (BPD) and the femur length (FL), are measured via ultrasound for NCFM eSnurra Group's "method" to estimate and calculate two separate sets of NCFM eSnurra EDD & GA values: NCFM eSnurra BPD-based EDD & GA and NCFM eSnurra FL-based EDD & GA. On the date of Laila's routine 18wUSE, Laila's factual LMPD/OTPD/SCID-based GA was 19w+4d (or 137 days), when the BPD and FL fetal metrics were measured: BPD = 41 mm and FL = 29 mm, from which NCFM eSnurra BPD-based EDD = 28.02.2017 and NCFM eSnurra FL-based EDD = 20.02.2017 were estimated and, therefrom, by using Naegele's rule, in reverse, NCFM eSnurra BPD-based GA = 17w+6d (or 125 days) and NCFM eSnurra FL-based GA = 19w+0d (or 133 days) were calculated, respectively. There was an obvious 8 day discrepancy between NCFM eSnurra BPD-based GA and NCFM eSnurra FL-based GA. This 8 day discrepancy was ignored by NCFM, Laila's doctor and her midwife, likely due to systemic, institutionalized confirmation bias and doublethink because the problematic, unreliable BPD measurement is NCFM eSnurra Group's premier, preferred predictor of EDD and, therefrom, their calculated GA, using Naegele's rule, in reverse. So, even when the 8 day discrepancy was pointed out by Laila & Edward, a discrepancy based, entirely, on NCFM eSnurra-based FL evidence, NCFM eSnurra Group's own evidence, Laila & Edward were ignored, thus confirming Directorate of Health's government-mandated protocol of evidence-obviated medicine not only obviates non-NCFM eSnurra evidence, but also obviates NCFM's own evidence when delivered by non-NCFM eSnurra messengers, i.e., Laila & Edward.
Dimensions of the BPD Problem
It is well known, internationally, BPD is a problematic, unreliable predictor of EDD and GA. The more robust head circumference (HC) should be used instead. Moreover, using HC instead of BPD is patently intuitive given the fact BPD is a diameter, a linear measurement in 1 spacial dimension, while HC is a measurement, which includes 2 perpendicular diameters in 2 spacial dimensions. Most ultrasound machines have a digital ellipse function which sonographers use to fit a digital ellipse to the contour of the fetal skull, otherwise 2 diameters are measured (i.e., BPD & OFD). Consequently, because HC is a measurement in 2 spacial dimensions it will always included more information about fetal head size than a BPD measurement in 1 spacial dimension. Additionally, HC is nearly insensitive to fetal head shape while BPD is highly sensitive to head shape and, therefore, is prone to generate grossly inaccurate EDD & GA values for non-standard head shapes and sizes, e.g., dolichocephaly and SGA, respectively. Moreover, if HC diameters (i.e., BPD & OFD) are measured, they can be used in a ratio to calculate a cephalic index (CI = BPD/OFD x 100) to provide information about head shape which can be used to identify a grossly inaccurate NCFM eSnurra BPD-based EDD & GA and to screen for fetal pathology, which begs the question: Why doesn't NCFM eSnurra Group measure the OFD to compute HC, or to at least calculate a CI to ensure BPD is not used to estimate a grossly inaccurate EDD & GA which is then assigned, irretrievably, as the "official" EDD & GA to a pregnancy?
- "CI refers to the ratio of the BPD and the occipitofrontal diameter (OFD) multiplied by 100 [25]. The standard CI range for normal-shaped craniums approximates one standard deviation from the mean (>74 or <83) [72]. Therefore, if the CI measurement approaches the outer limits of the normal range, the use of the BPD for estimation of gestational age is not accurate [72,73]. In these cases, HC (discussed below) is recommended for cranial assessment because it provides a good estimate of gestational age despite the fetus' irregular cranial structure [72]." (Source: "Prenatal assessment of gestational age and estimated date of delivery" Andrew P MacKenzie, MD, Courtney D Stephenson, DO, Edmund F Funai, MD, Deborah Levine, MD, Vanessa A Barss, MD, FACOG. UpToDate: Literature review current through: Sep 2017. | This topic last updated: Jun 26, 2017. https://www.uptodate.com/contents/prenatal-assessment-of-gestational-age-and-estimated-date-of-delivery)
- "...failing to account for the inclusion of fetuses with an elongated head whose biparietal diameter was adjusted based on the longitudinal axis of the skull." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "The midwives trained at the center in Trondheim have been recommended to measure the fronto-occipital diameter in fetuses considered to be dolichocephalic, and to use this information in order to assign an expanded virtual BPD for the calculation of gestational age and day of confinement. We cannot see that the authors have given any account of these fetuses or how this procedure influenced the statistics." (Source: Correspondence, Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, Ultrasound Obstet Gynecol 2008; 31: 225–228:)
- “We are in a serious situation. Science is supposed to be based on data/evidence. But, what if there is no data or no evidence fo [sic] the existence of raw data supporting the results of scientific papers? It is like a tower built on the sand.” (Source: Tsuyoshi Miyakawa: Twitter via Nature Briefing, Friday 21 February 2020)
"Abstract
A reproducibility crisis is a situation where many scientific studies cannot be reproduced. Inappropriate practices of science, such as HARKing, p-hacking, and selective reporting of positive results, have been suggested as causes of irreproducibility. In this editorial, I propose that a lack of raw data or data fabrication is another possible cause of irreproducibility.
As an Editor-in-Chief of Molecular Brain, I have handled 180 manuscripts since early 2017 and have made 41 editorial decisions categorized as “Revise before review,” requesting that the authors provide raw data. Surprisingly, among those 41 manuscripts, 21 were withdrawn without providing raw data, indicating that requiring raw data drove away more than half of the manuscripts. I rejected 19 out of the remaining 20 manuscripts because of insufficient raw data. Thus, more than 97% of the 41 manuscripts did not present the raw data supporting their results when requested by an editor, suggesting a possibility that the raw data did not exist from the beginning, at least in some portions of these cases.
Considering that any scientific study should be based on raw data, and that data storage space should no longer be a challenge, journals, in principle, should try to have their authors publicize raw data in a public database or journal site upon the publication of the paper to increase reproducibility of the published results and to increase public trust in science." (Source: "No raw data, no science: another possible source of the reproducibility crisis" Miyakawa, T. Molecular Brain 13, 24 (2020). https://doi.org/10.1186/s13041-020-0552-2)
"Researchers are under pressure to publish papers in ruthless competition. What if researchers who produce beautiful results based on non-existing data win against the ones who struggle with true data? Unfortunately, that is what is happening in science nowadays, I am afraid." (Source: Tsuyoshi Miyakawa: Twitter)
LMPD: Virtual vs. Real
NCFM eSnurra GA is calculated by using Naegele's rule in reverse. Subtract 283 days from the NCFM eSnurra EDD date to calculate a virtual LMPD (GA day 0, or 0w+0). Or, to calculate GA on the date of the ultrasound exam, simply subtract the NCFM-eSnurra estimated number of days remaining on the ultrasound date to delivery date from 283 days. So, 283 days from what? The answer, of course, is a virtual LMPD. Consequently, all ultrasound-based NCFM eSnurra calculated GA values are indirect estimates of LMPD. However, Laila knew her factual LMPD (09.05.2016), because Laila had documented this date when it presented in her pregnancy spreadsheet and her LMPD fully corroborated her factual OTPD. Consequently, NCFM eSnurra could not have calculated Laila's LMPD (real or virtual) from an estimated NCFM eSnurra BPD-based EDD any more accurately than Laila's factual LMPD. And, with the addition of Laila's SCID for a combined, full corroborating, factual LMPD/OTPD/SCID, the only method that could have been more accurate at establishing the beginning of Laila's pregnancy (i.e., in hours, not days) would have been if Laila were to have had an in vitro fertilization date (IVFD). This is a fact, not an opinion.
Corrected from Right to Wrong via Doublethink
If NCFM eSnurra BPD-based EDD & GA were to have been believed, all of Laila's factual, spreadsheet-recorded dates had to be wrong and, therefore, "corrected" by pushing all of Laila's key pregnancy dates forward (to the future) 12 days (or 1w+5) to conform with the grossly inaccurate NCFM eSnurra BPD-based EDD & GA temporal frame of reverence assigned to Laila's pregnancy; a grossly inaccurate temporal frame of reference. This is where it became indisputably clear Norwegian Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Groups "method" within a government-mandated protocol of evidence-obviated medicine required Laila's medical professionals to fully engage in doublethink. Norway's medical professionals must, via government-mandate, use NCFM eSnurra EDD & GA, exclusively, without question, no matter what fact-based evidence of proven efficacy is used to prove NCFM eSnurra EDD & GA values to be grossly inaccurate. None of Laila's medical professionals would listen to the arguments for using Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD as a reasonableness test for the NCFM eSnurra BPD-based EDD & GA assigned to Laila's pregnancy. Consequently, and despite repeated warnings with fact-based evidence, the routine procedure to turn Laila's baby from breech to vertex, it time, before the onset of labor, had been scheduled much too late, thus requiring Laila to endure an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications, and her baby to endure an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head which easily could have been a more serious fetal pathology.
BPD & Confirmation Bias with Doublethink
Interestingly, a third fetal metric, the mean abdominal diameter (MAD), was measured during Laila's 18wUSE on 23.09.2016, MAD = 46 mm (yellow highlighted values in the "Fetal Metric Measurements with GA & EDD" table, below), and was included in the same NCFM eSnurra ultrasound report along with the BPD and FL measurements. However, and strangely, the normally associated NCFM eSnurra EDD & GA values for MAD were withheld from the ultrasound report. A Google Search on the words "eSnurra" and "MAD" identified the NCFM eSnurra Group's website with NCFM eSnurra EDD & GA calculators and lookup tables, which begs the question: Why were the NCFM eSnurra MAD-based EDD & GA values withheld from the ultrasound report when these values were available to the public on the NCFM eSnurra Group's website? The MAD table on the NCFM eSnurra website showed 2 entries for MAD = 41 mm: 1) 150.4 days-remaining and 2) GA estimate of 19w+0d (or 133 days), which was then calculated into a MAD-based eSnurra EDD of 20.02.2017 = (ultrasound date + 150.4 days) = (23.09.2016 + 150.4 days), which, maybe not surprisingly, turned out to be the exact same EDD as NCFM eSnurra FL-based EDD. Consequently, both the NCFM eSnurra FL-based EDD and MAD-based EDD were the exact same date; and, both only lagged Laila's factual LMPD/OTPD/SCID-based EDD by 4 days, well under the normal variance umbrella of Laila's LMPD/OTPD/SCID-based EDD. Even if MAD were not to have been regarded as a particularly strong predictor/estimator, it had to be acknowledge that 2 separate measurements of 2 separate fetal metrics, FL & MAD, converging on the same EDD date and, consequently, the same calculated GA, would be overwhelming and compelling medical evidence that Laila's "official" NCFM eSnurra BPD-based EDD was grossly inaccurate, problematic and unreliable. In fact the 12 day lag and 4 day lag in NCFM eSnurra BPD-based GA and NCFM eSnurra FL & MAD-based GA, respectively, relative to Laila's LMPD/OTPD/SCID-based GA were important medical evidence of potential fetal pathology, such as a fetal growth restriction/malformation of Laila's baby's head or SGA or much worse. What should have been crystal clear is that NCFM eSnurra BPD-based EDD & GA were evidence of fetal pathology and not evidence of an accurate EDD & GA. This is a textbook example of confirmation bias (i.e., the tendency to interpret new evidence as confirmation of one's existing beliefs or theories). Consequently, and obviously, the "official" NCFM eSnurra BPD-based EDD of 28.02.20 was grossly inaccurate and, therefor, so was the NCFM eSnurra GA calculated from the grossly inaccurate EDD using the equivalent of Naegele's rule, in reverse. Therefore, it was clear NCFM eSnurra EDD & GA should not have been trusted in medical thinking, medical decision-making and medical actions; medical actions such as scheduling time-constrained medical procedures, especially time-critical procedures such as the turning of a fetus/baby from breech to vertex, in time, for normal delivery before the onset of labor to prevent an unwanted, unnecessary, risky breech delivery or an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications and, a baby who endured an unidentified, prolonged, undiagnosed, untreated fetal pathology such as an FGR/malformation of the head or much worse. But, again, it was confirmation bias for NCFM eSnurra BPD-based EDD & GA that kept Laila's medical professionals from accepting evidence that proved NCFM eSnurra BPD-based EDD & GA were grossly inaccurate when compared to NCFM eSnurra FL- & MAD-based EDD & GA and, therefore, the NCFM eSnurra BPD-based EDD & GA should have been identified as evidence of fetal pathology, not evidence of an accurately average EDD & GA. Again, no logic was allowed to penetrate Directorate of Health's 2014 Recommendation of evidence-obviated medicine, "the rule" of NCFM eSnurra Group or the oft-cited Norwegian national guidelines (i.e., the mandate). Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Symphysis-fundus Height (SFH): Evidence of grossly inaccurate NCFM eSnurra BPD-based EDD & GA
Laila's midwife measured Laila's SFH at each appointment beginning 27.10.2016 (Laila's GA = 24+3) for a total of 6 measurements which were plotted against NCFM eSnurra BPD-based GA (below). Notice how Laila's GA vs. SFH plots were tracking above the 90th centile, with 2 measurement above the 97.5 centile. This was evidence of:
- NCFM eSnurra BPD-based GA being grossly inaccurate, clearly lagging Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA by 12 days; however, if one were to shift all GA vs. SFH plot points forward by 12 days (1w+5), all plot points would be closer to the 50th centile curve/line.
- Laila's baby was breech, which was known and, not surprisingly, breech is known to increase SFH
- Laila is of relatively short stature which is also known to increases SFH
- Laila would be 38-years of age at delivery, with maternal age known to increase SFH
- Confirmed NCFM eSnurra FL-based GA and MAD-based GA, both lagging Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA by only 4 days were more accurate than NCFM eSnurra BPD-based GA lagging same by 12 days
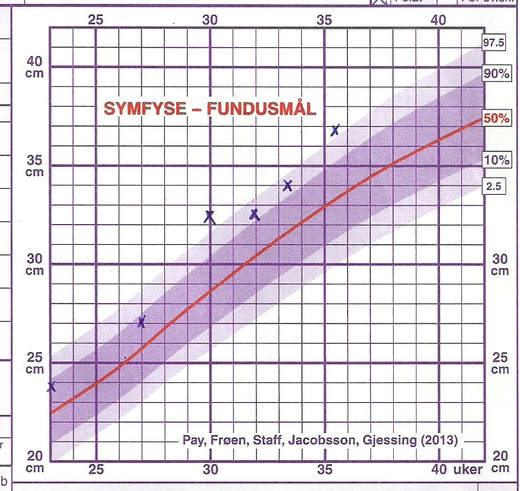
BPD: Known, Problematic, Unreliable Predictor of GA & EDD
Consider the excerpts below from NCFM eSnurra Group's publications. The first 2 excerpts make it clear BPD is NCFM eSnurra Group's premier, preferred predictor of EDD, and, therefrom, their calculated GA using the equivalent of Naegele's rule, in reverse. However, the second excerpt states "the predictive quality of the FL measurement was nearly as high as that of BPD." Also, the second excerpt mentions FL taking over in "cases where the BPD is ineligible for measurement," such as an "abnormal or non-standard head shape." And, the third excerpt states FL "has the same predictive capacity as BPD..." Therefore, why was FL-based NCFM eSnurra EDD & GA not compared or "quality assured" against NCFM eSnurra BPD-based EDD & GA given that FL and BPD have "the same predictive capacity?" The answer is: Because of confirmation bias and/or doublethink, which results in the use of NCFM eSnurra BPD-based EDD & GA even when overwhelming, contradictory evidence is presented in the form of NCFM eSnurra's own NCFM eSnurra FL-based EDD & GA. Also, notice the first excerpt (below) states: "(BPD) and/or the femur length (FL)" which, at the risk of stating the obvious, means use either BPD & FL, or use FL, do not use BPD alone, when "dating the pregnancy in mid-trimester." Salomon et al. 2011 state this in their "Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan" which recognizes BPD is problematic and unreliable.
Following the rule, no matter the evidence, no matter what, is clearly articulated in NCFM eSnurra Group member Inger Økland's 2012 NTNU dr.philos. Thesis which was (and remains) the only publicly available document purported by Directorate of Health to be independent, academic justification to support their selection of NCFM eSnurra Group's "method." These excerpts (below) from Økland's 2012 NTNU dr.philos. Thesis make this point abundantly clear. The last excerpt is the protocol of donning blindfolds & earmuffs to cross the street, i.e., the protocol of evidence-obviated medicine.
The excerpts below make it clear other researchers take a different approach regarding large discrepancies between LMPD/OTPD/SCID-based GA relative to ultrasound-based GA. This serves to demonstrate the difference between a government-mandated protocol of evidence-obviated medicine and the ethical practice of evidence-based medicine which includes all available evidence in the determination of GA and fetal age.
Consider the excerpts below from NCFM eSnurra Group's publications. The first 2 excerpts make it clear BPD is NCFM eSnurra Group's premier, preferred predictor of EDD, and, therefrom, their calculated GA using the equivalent of Naegele's rule, in reverse. However, the second excerpt states "the predictive quality of the FL measurement was nearly as high as that of BPD." Also, the second excerpt mentions FL taking over in "cases where the BPD is ineligible for measurement," such as an "abnormal or non-standard head shape." And, the third excerpt states FL "has the same predictive capacity as BPD..." Therefore, why was FL-based NCFM eSnurra EDD & GA not compared or "quality assured" against NCFM eSnurra BPD-based EDD & GA given that FL and BPD have "the same predictive capacity?" The answer is: Because of confirmation bias and/or doublethink, which results in the use of NCFM eSnurra BPD-based EDD & GA even when overwhelming, contradictory evidence is presented in the form of NCFM eSnurra's own NCFM eSnurra FL-based EDD & GA. Also, notice the first excerpt (below) states: "(BPD) and/or the femur length (FL)" which, at the risk of stating the obvious, means use either BPD & FL, or use FL, do not use BPD alone, when "dating the pregnancy in mid-trimester." Salomon et al. 2011 state this in their "Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan" which recognizes BPD is problematic and unreliable.
- "Today, the predominant method of dating the pregnancy in mid-trimester is to use ultrasound biometric measurements, in particular the biparietal diameter (BPD) and/or the femur length (FL)" (Source: Ultrasound Obstet Gynecol 2007; 30: 19–27, "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," p. 19, H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, DOI: 10.1002/uog.4053)
- "The predictive quality of the FL measurement was nearly as high as that of the BPD, providing an alternative prediction in cases where the BPD is ineligible for measurement." (Source: ibid,p. 27)
- "Our results shows that FL has the same predictive capacity as BPD at the same gestational age. We still believe that BPD ought to be the prime parameter for predicting term, but FL may be used in cases of abnormal cephalic shapes and to quality-assess the BPD-values." (Source: OP08: FETAL BIOMETRY: OP08.01: A new population-based term prediction method – evaluation of the BPD-based predictions, I. Økland, H. K. Gjessing, P. Grøttum, T. M. Eggebø, S. H. Eik-Nes, Ultrasound in Obstetrics & Gynecology 2007; 30: 456–546, p. 478 http://onlinelibrary.wiley.com/doi/10.1002/uog.4468/pdf)
- "From a clinical perspective, our study shows that if a practitioner decides not to use the BPD measurement for a given fetus, femur length (FL) is fully on a par with BPD in terms of predictive quality. FL is thus a simple and desirable replacement in situations in which head measurements are not trusted." (Source: Correspondence Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, H. K. Gjessing*, P. Grøttum and S. H. Eik-Nes, Ultrasound Obstet Gynecol 2008; 31: 225–228., p. 226)
- "We found the FL predictions to have nearly the same quality as the BPD predictions." (Source: A new population-based term prediction model vs. two traditional sample-based models: validation on 9046 ultrasound examinations, I. ØKLAND, H. K. GJESSING, P. GRØTTUM, T. M. EGGEBØ and S. H. EIK-NES, Ultrasound Obstet Gynecol 2011; 37: 207–213, DOI: 10.1002/uog.7728)
- "Calculation of growth. Valid from week 26/0. Growth is calculated using BPD and MAD. In priciple [sic] use BPD. With abnormal head shape, use FL, which provides an approximately equal estimation as BPD." (Source: NCFM eSnurra website: http://www.nsfm.no/esnurra/3.php (© 2007 Eik-Nes, Grøttum og Gjessing))
- "Calculation of due date by routine ultrasound exam. Valid from week 15/6 to week 22/6. In principle use BPD. Under abnormal head shape use FL which gives as precise a due date as BPD. BPD and FL quality assure each other and therefore both should be filled in." (Source: NCFM eSnurra website: http://www.nsfm.no/esnurra/2.php (© 2007 Eik-Nes, Grøttum og Gjessing))
- "From week 15/6 to 22/6, FL can be used to quality assure the BPD measurement." (Source: eSnurra website: http://www.esnurra.com/how-to-use-esnurra/)
Following the rule, no matter the evidence, no matter what, is clearly articulated in NCFM eSnurra Group member Inger Økland's 2012 NTNU dr.philos. Thesis which was (and remains) the only publicly available document purported by Directorate of Health to be independent, academic justification to support their selection of NCFM eSnurra Group's "method." These excerpts (below) from Økland's 2012 NTNU dr.philos. Thesis make this point abundantly clear. The last excerpt is the protocol of donning blindfolds & earmuffs to cross the street, i.e., the protocol of evidence-obviated medicine.
- "The data that were collected from fetal examinations in Trondheim were used by Eik-Nes et al. to introduce the phrase ‘TUL‘ — Term according to ULtrasound — which for 25 years has been a fixed Norwegian term, resulting in a uniform dating system from ultrasound, regardless of whether the LMP was reliable or not. Even the Medical Birth Registry of Norway, founded in 1967, from 1999 records the ultrasound-based EDD. In 1984, Eik-Nes and Grøttum developed an ultrasound form, called ‘the blue form’. This was soon used nationally as a standard form for registration of the ultrasound findings throughout pregnancy, and it became part of the pregnant woman's medical journal until delivery." (Source: Økland's 2012 NTNU dr.philos. Thesis, p. 21)
- "In Norway, this study supported the established policy of using the term according to ultrasound, ‘TUL’, independent of the LMP term date." (Source: Økland's 2012 NTNU dr.philos. Thesis, p. 30)
- "If the LMP is used only for scheduling of the dating examination, all questions where the length of gestation influences the answer will relate to the ultrasound-based GA/EDD after the examination is performed." (Source: Økland's 2012 NTNU dr.philos. Thesis, p.35).
- "Irrespective of the applied prediction model, recognizing early intrauterine growth restriction is a challenge when dating pregnancies with ultrasonography, because the biological variation in growth is being ‘reset’ to a mean level for all fetuses. Significant discrepancies between reliable LMP-based and ultrasound-based predicted dates need to be acknowledged." (Source: "Biases of traditional term prediction models: results from different sample-based models evaluated on 41 343 ultrasound examinations" I. ØKLAND, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2010; 36: 728–734, p. 733. DOI: 10.1002/uog.7707)
- "The population-based model will better predict the date of delivery for fetuses with intrauterine growth restriction (IUGR). However, identification of early IUGR fetuses cannot be performed from one single ultrasound examination, irrespective of the prediction model 27. Any significant difference between reliable LMP-based and ultrasound-based EDD dates indicates a need for further evaluations 27 –29." (Source: Advantages of the population-based approach to pregnancy dating: results from 23 020 ultrasound examinations, I. ØKLAND, J. NAKLING, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2012; 39: 563–568, p. 567 DOI: 10.1002/uog.10081)
- "The identification of a small for gestational age (SGA) fetus may follow from a significant discrepancy between a reliable LMP-based and the ultrasound-based EDD at the second-trimester examination (Tunón et al. 1999a, Nguyen et al. 2000, Källén 2004, Morin et al. 2005). However, the postponing of an ultrasound-based EDD relative to the LMP predicted date is in most cases due to a late ovulation, and the majority of these pregnancies prove to be completely normal, with deliveries of normal infants close to the ultrasound-based due date (Tunón et al. 1999b, Larsen et al. 2000, Morin et al. 2005, Fox et al. 2008, Thorsell et al. 2008)." (Souce: Økland's 2012 NTNU dr.philos. Thesis, p. 37)
- "Although Larsen et al. 19 concluded that growth-restricted fetuses were not incorrectly classified as of low gestational age, their data actually show an increased risk of low birthweight when the last normal menstrual period-based gestational age estimate exceeded the early ultrasound estimate by >7 days." (Source: "Determinants and consequences of discrepancies in menstrual and ultrasonographic gestational age estimates" Isabelle Morin, Lucie Morin, Xun Zhang, Robert W. Platt, Béatrice Blondel, Gérard Bréart, Robert Usher, Michael S. Kramer. BJOG An Interntional Journal of Obstetrics & Gynecology Volume 112, Issue 2 February 2005. Pages 145–152. First published: 3 November 2004. DOI: 10.1111/j.1471-0528.2004.00311.x)
The excerpts below make it clear other researchers take a different approach regarding large discrepancies between LMPD/OTPD/SCID-based GA relative to ultrasound-based GA. This serves to demonstrate the difference between a government-mandated protocol of evidence-obviated medicine and the ethical practice of evidence-based medicine which includes all available evidence in the determination of GA and fetal age.
- "On the other hand, revising gestational age according to ultrasound measurement may be harmful to those fetuses that are pathologically small at that stage since this will tend to underestimate fetal weight deviation and postmaturity and thereby hinder induction of labour when indicated." (Source: "Does a discrepancy between gestational age determined by biparietal diameter and last menstrual period sometimes signify early intrauterine growth retardation?" Larsen T, Nguyen TH, Greisen G, Engholm G and Møller H. BJOG 2000; 107: 238-244.)
"It is possible that fetuses with small biparietal diameter due to early growth retardation, which are inappropriately assigned a lower gestational age by the biparietal diameter method, are under-represented in spontaneous births and therefore the accuracy of the biparietal diameter method may be overestimated." (Source: ibid.,p. 238)
"However the risk of low birthweight (c 2500 g) and low birthweight for gestational age was significantly increased when (GA(LMP)-GA(BPD) was > 7 days." (Source: ibid., p. 238)
"Our findings support the use of biparietal diameter as the routine method for calculating gestational age. There was no evidence that growth retarded fetuses were systematically wrongly classified as of falsely low gestational age. A discrepancy between GA(LMP), and GA(BPD), is therefore generally indicative of late ovulation. However, the relative risk of a low birthweight infant is slightly increased. " (Source: ibid., p. 244) - However, disparities in growth may occur at an early stage of pregnancy owing to chromosomal or structural abnormalities, early placental maladaptation or environmental factors including nutrition 26. Consistent with this hypothesis are the relatively smaller CRLs in fetuses with triploidy and trisomy 18 5. "In clinical practice, substantial differences between gestational age based on ultrasound measurements and LMP, if reliable, should be considered as an indicator of possible pathology and an increased risk of fetal growth restriction 27." (Source: "New charts for ultrasound dating of pregnancy and assessment of fetal growth: longitudinal data from a population-based cohort study" B. O. Verburg, E. A. P. Steegers, M. De Ridder, R. J. M. Snijders, E. Smith, A. Hofman, H. A. Moll, V. W. V. Jaddoe, J. C. M. Witteman. Ultrasound in Obsterics & Gynecology Volume 31, Issue 4 April 2008. Pages 388–396 First published: 17 March 2008. DOI: 10.1002/uog.5225")
Ultrasound Shifted GA Distribution at the Expense of SGA Perinatal Mortality
A 1989 U.S. study, Rossavik & Fishburne 1989, concluded "that gestational age based on good menstrual records supported by a pelvic examination in the first trimester may be more reliable than even the best ultrasound method for dating."
A 1989 U.S. study, Goldenberg et al. 1989, concluded: "It is apparent that changes in use of ultrasonography had a profound effect on the reported gestational age distribution at our institution." Specifically, "a sharp increase in the preterm delivery rate and a coincident decrease in the postterm delivery rate and the rate of intrauterine growth retardation were noted."
The complete summary of Goldenberg et al. 1989 or "Prematurity, postdates, and growth retardation: The influence of use of ultrasonography on reported gestational age" is included below.
A 1992 Norwegian study, Bergh 1992, identified 33 perinatal deaths in 1991 at Rogaland Hospital (now Stavanger University Hospital). The 31 perinatal deaths (i.e., dead babies) were classified into 3 groups as follows:
- "Abstract
Ultrasound dating-curve analysis was performed for the biparietal diameter, mean head diameter, and mean trunk diameter in individual singletons, twins, and triplets from in vitro fertilization (IVF) pregnancies and pregnancies with ultrasonographic determination of ovulation. Linear growth was found for all parameters prior to 28 weeks' conceptional age. No differences were observed among singletons, twins, or triplets. Using linear equations, no significant difference was found in systematic errors between pregnancies with a known date of conception and pregnancies dated from the last menstrual period (LMP). Pregnancies with reliable LMPs had only a slight and nonsignificant increase in random errors when compared with pregnancies from IVF. Current polynomial dating equations produced considerable systematic and random errors as well as errors related to fetal growth. Acceptable results were obtained with a new linear equation based on two examinations. We conclude that gestational age based on good menstrual records supported by a pelvic examination in the first trimester may be more reliable than even the best ultrasound method for dating."
"Discussion
(...)
"An important advantage given by the two ultrasound examinations is projection of individudal growth curves necessar for reliable deteremination of growth acceleration or retardation after 30 weeks.13 These individual growht curves, however, can be decided from only one examination, at approximately 25 weeks, in pregnant women with good menstrual dates. Education regarding the necessity for accurate menstrual records therefore has fundamental value for those couples pursuing a pregnancy." (Source: "Conceptional age, menstrual age, and ultrasound age: a second-trimester comparison of pregnancies of known conception date with pregnancies dated from the last menstrual period." Rossavik IK, Fishburne JI. Obstet Gynecol. 1989 Feb;73(2):243-9.)
A 1989 U.S. study, Goldenberg et al. 1989, concluded: "It is apparent that changes in use of ultrasonography had a profound effect on the reported gestational age distribution at our institution." Specifically, "a sharp increase in the preterm delivery rate and a coincident decrease in the postterm delivery rate and the rate of intrauterine growth retardation were noted."
The complete summary of Goldenberg et al. 1989 or "Prematurity, postdates, and growth retardation: The influence of use of ultrasonography on reported gestational age" is included below.
- Summary
The preterm and postterm delivery rates and the percentage of infants with intrauterine growth retardation are dependent on the gestational age recorded at delivery. At our institution a sharp increase in the preterm delivery rate and a coincident decrease in the postterm delivery rate and the rate of intrauterine growth retardation were noted. Over a 3-year period, while the characteristics of the obstetric population changed only slightly, the gestational age distribution shifted, with a decrease in the mean gestational age of about 1 week and a rise in the reported preterm delivery rate from 12% to 17%. About 15% of this rise was explained by an increase in obstetric interventions, and another 15% can be explained by changes in the way physicians rounded off gestational age. The majority of the increase in the preterm delivery rate was related to changes involving ultrasonographic examinations. These changes included a greater percentage of the population examined, trends toward earlier examinations, a tendency for the physicians to use ultrasonography rather than the last menstrual period in choosing the final gestational age, the use of different standards, an increase in the number of structures measured, and the weight given to various structures for determination of gestational age. It is apparent that changes in use of ultrasonography had a profound effect on the reported gestational age distribution at our institution. (Source: "Prematurity, postdates, and growth retardation: The influence of use of ultrasonography on reported gestational age" Robert L. Goldenberg, MD, Richard O. Davis, MD, Gary R. Cutter, PhD, Howard J. Hoffman, MA, Cynthia G. Brumfield, MD, Judith M. Foster, MPH. American Journal of Obstetrics & Gynecology February 1989; Volume 160, Issue 2,:462-470. DOI: http://dx.doi.org/10.1016/0002-9378(89)90473-0)
A 1992 Norwegian study, Bergh 1992, identified 33 perinatal deaths in 1991 at Rogaland Hospital (now Stavanger University Hospital). The 31 perinatal deaths (i.e., dead babies) were classified into 3 groups as follows:
- 7 (23%) of the 33 perinatal deaths showed severely retarded growth (< 3 percentile) and for whom LMPD-based EDD (i.e., Naegele's rule) had been delayed an average of 18 days by ultrasound (i.e., NCFM Snurra BPD-based GA)
- 5 (16%) of the 33 perinatal deaths showed moderately retarded growth (from 3-10 percentile) and for whom LMPD-based EDD (i.e., Naegele's rule) had been delayed an average of 8 days by ultrasound (i.e., NCFM Snurra BPD-based GA)
- 21 (61%) of the 33 perinatal deaths were not definitely growth retarded and for whom LMPD-based EDD (i.e., Naegele's rule) had been delayed an average of 5 days by ultrasound (i.e., NCFM Snurra BPD-based GA)
(Source: "Bør ultralydundersøkelsen gjøres tidligere i svangerskapet?" [Should ultrasound examination be performed earlier in pregnancy?]. Bergh, J. (1992). Tidsskrift for den Norske lægeforening : tidsskrift for praktisk medicin, ny række. 1992; 112. 3450-1.) [Note: the link directs to the article's abstract at ResearchGate.net, as no other Internet-based sources were found.]
- "In one case of pregnancy following in vitro fertilization, the ultrasound term was calculated 22 days later than the term on the basis of known time of conception, relative to an ultrasound term set in 18-19 weeks, this can cause serious consequences in early growth retardation. Earlier ultrasound testing will provide more reliable term provision. The malformation diagnosis should be separate from the term provision."
- “To a man with a hammer, everything looks like a nail.” --Mark Twain
- Abstract (excerpt)
"A delivery date estimated by ultrasound at 18-19 weeks may cause serious misjudgements in cases of early retardation of growth. Earlier ultrasound examination is recommended for a more reliable estimated date of delivery." (Source: "Bør ultralydundersøkelsen gjøres tidligere i svangerskapet?" [Should ultrasound examination be performed earlier in pregnancy?]. Bergh, J. (1992). Tidsskrift for den Norske lægeforening : tidsskrift for praktisk medicin, ny række. 1992; 112. 3450-1.) [Note: the link directs to the article's abstract on ResearchGate.net, as other Internet-based sources were not found.]
[Note: Bergh 1992 is provided via the courtesy and kind assistance of Tidsskrift for Den norske legeforening (The Journal of the Norwegian Medical Association).
BPD was, and remains, a problematic, unreliable estimator of GA or EDD during routine ultrasound exams. It is known, internationally, that the more robust HC should be used instead of BPD, or HC should be used in conjunction with BPD to keep BPD in check; but, BPD should not be used alone. HC is a measurement of 2-spacial dimensions perpendicular to each other (BPD & OFD) and includes more information of fetal head size while being practically insensitive to fetal head shape. On the other hand, BPD is a measurement of just 1-spacial dimension and, thereby, is highly sensitive to fetal head shape. This is precisely why the NCFM eSnurra BPD-based EDD & GA assigned to Laila's pregnancy was grossly inaccurate and caused unnecessary increased medical risks, critical medical mistakes and grievous medical harms for Laila and her baby, and other women and their babies.
Bergh 1992 made it clear this problem existed in 1991; and, incredulously, this same, known BPD problem exists today and will be allowed to continue to exist into 2018 with the same results as those reported in Bergh 1992 and the studies included below, which begs the question: Which dimension of the 1-dimensional BPD measurement problem do Ministry of Health and Care Services, Directorate of Health and NCFM eSnurra Group not understand? This frozen-in-the-past, tunnel-vision fixation on using the problematic, unreliable BPD as the one and only fetal head measurement, no matter what, is a classic, fact-based example of why Directorate of Health's 2014 Recommendation is a knowledge-obviated policy in addition to being medically & ethically flawed, intentionally reckless & willfully negligent. Intentionally and deliberately obviating medical knowledge is the conscious disregard of the risks and consequences which constitutes willful negligence; willful negligence is a criminal act if it causes harm.
Bergh 1992 made it clear this problem existed in 1991; and, incredulously, this same, known BPD problem exists today and will be allowed to continue to exist into 2018 with the same results as those reported in Bergh 1992 and the studies included below, which begs the question: Which dimension of the 1-dimensional BPD measurement problem do Ministry of Health and Care Services, Directorate of Health and NCFM eSnurra Group not understand? This frozen-in-the-past, tunnel-vision fixation on using the problematic, unreliable BPD as the one and only fetal head measurement, no matter what, is a classic, fact-based example of why Directorate of Health's 2014 Recommendation is a knowledge-obviated policy in addition to being medically & ethically flawed, intentionally reckless & willfully negligent. Intentionally and deliberately obviating medical knowledge is the conscious disregard of the risks and consequences which constitutes willful negligence; willful negligence is a criminal act if it causes harm.
A 1989 U.S. study, Rossavik & Fishburne 1989, concluded "that gestational age based on good menstrual records supported by a pelvic examination in the first trimester may be more reliable than even the best ultrasound method for dating."
A 1992 U.K. study, Gardosi et al. 1992, identified computer-based customized fetal growth charts to account for growth variances due to physiological variables.
A 1995 Danish study, Henricksen et al. 1995, identified that the bias induced by ultrasound dating of gestational age "can distort the relative risk of preterm or postterm delivery by 10-20%."
A 1996 U.K. study, Mongelli et al. 1996, established the value of using known conception dates in conjunction with ultrasound and LMPD to establish a more accurate estimate of gestational age in individual pregnancies.
A 1997 Danish study, Olsen & Clausen 1997, concluded that Ultrasound-based EDD is not necessarily better than LMP-based EDD.
A 1997, study of Norwegian births, Campbell et al. 1997, established small for gestational age (SGA) as a risk factor for perinatal mortality in post-term births (adjusted RR 5.68; 95% CI 4.37, 7.38). Included below is the full abstract of this study.
A 1998 study of Swedish births, Divon et al. 1998, established that "fetal growth restriction was independently associated with significantly higher odds ratios for both fetal and neonatal mortality rates at every gestational age examined (with odds ratios ranging from 7.1 to 10.0 for fetal death and from 3.4 to 9.4 for neonatal death)."
A 1999 Australian study, Roberts et al. 1999, identified gestational age determination by ultrasound causing a GA distribution shift from 40 weeks to 38 and 39 weeks at birth/delivery, but did not make the connection with perinatal mortality rates.
A 1999 Norwegian study, Tunón et al. 1999a, originated as Paper III: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" within Katarina Tunón's 1999 NTNU PhD Thesis which was supervised by NCFM Snurra Group members Sturla H. Eik-Nes and Per Grøttum. NCFM Snurra Group's Tunón et al. 1999a found "no indication of any adverse consequence of the routine scan and change of estimated day of delivery" despite evidence to the contrary. Tunón et al. 1999a articulated the problem of discrepant LMPD-based GA and ultrasound-based GA in their introduction. However, Tunón et al. 1999a excluded the compounding issue that BPD is a problematic, unreliable estimator of GA or EDD during routine ultrasound exams because BPD has problems with non-standard fetal head shapes. Moreover, fetal head sizes are not all the same (i.e. accurately average) for a given GA due to random fetal growth velocity variances and/or fetal pathology; and, these variances get translated directly into GA variances (i.e., GA errors). HC should be used instead of, or in conjunction with BPD, because HC is a more robust estimator and is practically insensitive to fetal head shape for GA or EDD estimations.
The excerpt below is NCFM eSnurra Group at their science-bending best. This is where NCFM eSnurra Group asserted:
The excerpt above from Tunón et al. 1999a clearly identified an "indication" of perinatal death which would have to be considered as an "indication" of an"adverse consequence of the routine scan and change of estimated day of delivery," which begs the question: If "the estimated relative risk of perinatal death of 2.07 with a confidence interval of 0.93–4.61" resulting from the evidence of 7 dead fetuses/babies whose EDDs had been changed by ultrasound an average of 25.6 days later (median of 24 days later) was not an "indication" of "an adverse consequence of the routine scan and change of estimated day of delivery," then what was it? Also, the excerpt above indicates "the estimated relative risk of perinatal death of 2.07 with a confidence interval of 0.93–4.61 should lead to further investigations of the frequency and causes of perinatal mortality in this group of patients. " Consequently, there had to have been some sort of an "indication" for NCFM Snurra Group to have stated "further investigations" of the identified relative risk of perinatal death of 2.07, yet NCFM eSnurra Group's Tunón et al. 1999a explicitly concluded and stated: "no indication of adverse fetal outcome was found. " For contrast, included below is the stated aim of Tunón et al. 1999a (i.e., Paper III) from Tunon's 1999 NTNU PhD Thesis.
Compare the "Objective" and "Results" sections (below) from the ABSTRACT in Tunón et al. 1999a.
The downstream effects of Tunón et al. 1999a excluding the "relative risk of perinatal death of 2.07" from the Results and Conclusion sections is evidenced in a 1999 Swedish opinion article, Persson 1999, titled "Ultrasound dating of pregnancy - still controversial?" published in Ultrasound In Obstetrics and Gynecology (the official journal of ISUOG) cited Tunón et al. 1999a and Tunón et al. 1999b (citations 2 and 3 in the excerpt below) without any mention of the "relative risk of perinatal death of 2.07" identified in Table 2 of Tunón et al. 1999a. Interestingly, Sturla H. Eik-Nes head of NCFM Group (Trondheim), is a coauthor of Tunón et al. 1999a and Tunón et al. 1999b as well as principal supervisor of Katarina Tunón's 1999 NTNU PhD Thesis; moreover, and at that time, Sturla H. Eik-Nes was President ISUOG (1998 - 2002).
A 2000 Danish study, Nguyn et al 2000, of 16,469 pregnancies, found a positive discrepancy between LMP-based GA and BPD-based GA of >8 days is associated with:
A 2000 Swedish PhD Thesis, Clausson 2000, identified and discussed risk factors for SGA fetuses of "three distinct subgroups," highlighting the importance of identifying SGA fetuses at risk.
A 2002 Canadian study, Yang et al. 2002, concluded: "early ultrasound scan-based reclassification of gestational age results in a substantial increase in the prevalence of preterm births."
A 2002 Canadian study, Blondel et al. 2002, which included 4 of the coauthors of Yang et al. 2002, showed post-term births >=41 weeks and >=42 weeks decreased by 46% and 70%, respectively and, preterm births <37 weeks increased 20% when ultrasound was used to estimate gestational age, thereby demonstrating ultrasound-based GA has a major impact on the rate of post-term and preterm birth classifications.
A 2002 U.S. study, Smith-Bindman et al, 2002, concluded 2 ultrasound exams can estimate neonatal morbidity even when GA is unknown. Interestingly, 1 ultrasound exam combined with a factual LMPD/OTPD/SCID-based GA can do the same thing, but with increased precision and at no additional cost, as Laila & Edward had proved, just before they were ignored into harms' way.
A 2002 Norwegian study, Nakling & Backe 2002, completely contradicts the conclusion of the Norwegian study, Tunón et al. 1999a, as is made clear in the Abstract (below). The main results of Nakling & Backe 2002 (Paper I) were summarized on page 25 of Nakling's 2004 NTNU PhD Thesis as follows:
A 2002 Swedish Study, Källén 2002, showed systematic errors, erroneous adjusted dates, are inherent in the ultrasound method of predicting date of delivery.
A 2004 Swedish study, Källén 2004, followed Källén 2002 (above) and showed the risk for stillbirth/neonatal death increased linearly with the size of the discrepancy between LMP-based GA and Ultrasound-based GA. When infants who were SGA at birth were excluded, there was still an increased risk for perinatal/neonatal death when discrepancy was at least 5 days less than LMP-based GA, but no linear relationship between negative adjustment and perinatal/neonatal death was demonstrated. Moreover, Källén 2004 explained the association between adverse outcomes and adjustment of GA via ultrasound is likely to be underestimated given the misclassificaitons resulting from reliability of self-reported LMPD recall occurred to the same extent in both groups (i.e., LMP-based GA and ultrasound-adjusted GA) will therefore bias towards the null, ergo non-differential misclassifications (i.e., no LMPD recall bias).
A 2005 Swedish study, Lindqvist & Molin 2005, "found an awareness of SGA before delivery, in combination with a structured program of surveillance for those identified as SGA, was related to a four-fold lowered risk of adverse fetal outcome. " (Source: "Does antenatal identification of small-for-gestational age fetuses significantly improve their outcome?" . G. Lindqvist, J. Molin. Ultrasound in Obstetrics & Gynecology Volume 25, Issue 3 March 2005. Pages 258–264. https://doi.org/10.1002/uog.1806. First published: 17 February 2005)
A 2005 Canadian study, Morin et al. 2005, concluded that "although positive differences between menstrual and early ultrasound‐based gestational age often indicate erroneous menstrual dates due to delayed ovulation, erroneous recall of the last period, missed miscarriage or other explanations, they are also associated with early fetal growth restriction, a consequently smaller biparietal diameter and systematic under‐estimation of the true gestational age."
A 2005 Norwegian study, Nakling et al. 2005, made a critically important point regarding ovulation variance which, when ovulation date is known via highly reliable (high sensitivity (i.e., low false positives) & high specificity (i.e., low false negatives)), home-use, digital, urinary ovulation tests and ovulation test systems to establish OTPD:
A joint U.K and U.S. study, Bukowski et al. 2007, established "...the association between fetal growth in early pregnancy and the risk of delivering a small for gestational age infant."
A 2008 Swedish study, Thorsell et al. 2008, conducted by the Karolinska Institutetat in Stockholm made the point that when ultrasound-based dating postponed EDD by 7 days or more there was "an increased risk for preterm delivery and pre-eclampsia." Laila's EDD was postponed by 15 days and 14 days relative to her factual LMPD-based EDD and her factual LMPD/OTPD/SCID-based EDD, respectively. Moreover, Laila suffered from postpartum pre-eclampsia. Additionally, and with respect to this study, Laila's first trimester ultrasound exam showed her baby's NCFM eSnurra CRL-based GA and BPD-based GA lagging her factual LMPD/OTPD/SCID-based GA by 9 days and 6 days, respectively. However, this evidence was also ignored. Included below is the abstract of Thorsell et al. 2008 or "Expected day of delivery from ultrasound dating versus last menstrual period--obstetric outcome when dates mismatch."
A 2008 Danish Study, Pedersen et al. 2008, found a BPD growth rate relationship in the beginning of pregnancy with adverse pregnancy outcome, implying a sub-optimal environment in early pregnancy limits fetal growth throughout pregnancy.
A 2008 Norwegian study, Johnsen et al. 2008, assessed the effect of second trimester fetal size on the duration of pregnancy and the influence of ultrasound dating. This study used the more robust head circumference (HC) instead of the problematic, unreliable BPD metric for fetal head measurements and GA estimations. The results of Johnsen et al. 2008 "support a concept of individually assigned pregnancy duration according to growth rates rather than imposing a standard of 280–282 days on all pregnancies." This concept has been supported by subsequent studies, including the U.S. study, Jukic et al. 2013, conducted by The National Institute of Environmental Health Sciences (NIEHS) of the U.S. National Institutes of Health (NIH).
A 2010 Swedish study, Skalkidou et al. 2010, based on data from the Swedish Medical Birth Registry (SMBR) concluded there was an increased risk of adverse perinatal outcomes for baby girls (i.e., smaller) relative to baby boys after ultrasound was introduced for estimation of GA. The complete abstract of Skalkidou et al. 2010 or "Ultrasound pregnancy dating leads to biased perinatal morbidity and neonatal mortality among post-term-born girls" is included below.
A 2014 Australian study, Carberry et al. 2014, is a Cochrane Review study of The Cochrane Pregnancy and Childbirth Group’s Trials Register. And, while authors' concluded no randomized trials met the inclusion criteria, authors provide highly relevant background information for fetal growth restriction (FGR), small for gestational age (SGA) and and the importance of detecting SGA, especially within low-risk populations.
A 2014 Norwegian study, Morken et al. 2014, conducted a retrospective analysis of data for 1,855,682 pregnancies in Norway from the Medical Birth Registry of Norway (MBRN). Morken et al. presented disturbing but not an unexpected results or unexpected conclusion which directly relates to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine (i.e., "TUL" policy and protocol). It is important to note all ultrasound-based estimations of GA in study periods 1987–2006 and 1999-2006 were conducted using the Campbell Method of Gestational Age Estimation (Campbell 1969) via NCFM Snurra BPD-based GA, as stated on page 2 and via citation 23 of Morken et al. 2014. Moreover, authors identified an important clinical implication which directly addresses, if not defines, the single most important clinical issue within LailasCase.com:
A 2016 Swedish study, Kullinger et al. 2016, used data from 1,314,602 births via the Swedish Medical Birth Register (SMBR), which contains data for 99% of all births in Sweden since 1973, to compare adverse outcomes related to prematurity between male and female babies for ultrasound and LMP pregnancy dating methods. The Results and Conclusion sections from the abstract of Kullinger et al. 2016 or "Effects of ultrasound pregnancy dating on neonatal morbidity in late preterm and early term male infants: a register-based cohort study" are included below.
A 2016 international study, Morken 2016, of singleton live births in the Medical Birth Registries of Norway, Sweden and Finland and US live birth certificates demonstrated "that discrepancy between methods to estimate gestational age may be a predictor for infant mortality and other adverse pregnancy outcomes in all four study countries."
A 2016 Norwegian study, Bohlin et al. 2016, stated that "more accurate methods for estimating GA...would be of great benefit in clinical practice." The NCFM eSNurra "method" per citation/reference [1] (below) estimates EDD, not GA. The NCFM eSnurra "method" must calculate GA from an estimate of EDD using the equivalent of Naegele's rule, but in reverse. The NCFM eSnurra "method" neither estimates nor uses gestational age (GA) to assess due dates (EDD). Moreover, NCFM's eSnurra EDD estimation "method" is an appropriated, plagiarized, misused implementation of Dr. David J. R. Hutchon's original idea and method of Population-based Direct EDD Estimation (PDEE) published in 1998 (Hutchon 1998).
A 2017 Swedish study, Kullinger et al. 2017, looked at discrepancies between EDD-LMP and EDD-US gestational age. The Key Message: "Variance in early fetal growth can bias ultrasound-based pregnancy dating. Maternal obesity, height, and fetal sex may partly explain large discrepancies between pregnancy-dating methods."
A Swedish Commentary, Skalkidou et al. 2018, looked at the effects and clinical implications of misclassification of gestational age by ultrasound-based pregnancy dating in the the Nordic countries. The Key Message: "Misclassification of gestational age by ultrasound biometry in the second trimester may influence the numbers and the magnitude of adverse perinatal outcomes, closely related to gestational age, which are recorded in the Nordic birth registers. Continued reporting of last menstrual period in the registries is advocated."
A 2018 "Expert Review" titled "The World Health Organization fetal growth charts: concept, findings, interpretation, and application" states:
Epidemiological Studies: Adverse Outcomes Associated with Discrepancies Between LMP-GA & US-GA
The common theme among the studies included among the epidemiological studies is that large discrepancies between LMP-GA/EDD and Ultrasound-GA/EDD are associated with misclassification of gestational age and adverse outcomes which include perinatal and neonatal mortality. Laila's case proved that using Ultrasound-based EDD, unilaterally, and, therefrom, a calculating GA using the equivalent of Naegele's rule, in reverse, causes increased medical risks, critical medical mistakes and grievous medical harms. perinatal and neonatal mortality
Evidence-obviated Medicine: Unilateral NCFM eSnurra BPD-based EDD (or 'TUL' policy), No Matter What!
Ironically, one of the better descriptions of the problem in the literature is that which was included in NCFM Snurra Group's Tunón et al. 1999a (first excerpt below).
Evidence Supports Implementation of the Precautionary Principle
The epidemiological evidence (above, sans NCFM Snurra Group's red herring that is Tunón et al. 1999a) is both voluminous and clear, but especially the Norwegian study, Morken et al. 2014. One would think the risks and consequences identified by a plethora of international clinical and epidemiological evidence would be enough to implement the Precautionary Principle. The data and evidence assembled and presented in the Norwegian Studies are compelling, beginning with Johan Bergh's 1992 article, Bergh 1992, published in Tidsskrift for den Norske lægeforening, followed by Nakling & Backe 2002 in Acta Obstetricia et Gynecologica Scandinavica (AOGS), Nakling et al. 2005 in Early Human Development, Johnsen et al. 2008 in BMC Pregnancy and Childbirth and concluding with Morken et al. 2014, published in BMC Pregnancy and Childbirth. The published evidence makes it clear that SGA and growth restricted/malformed fetuses are at increased risk of perinatal death when estimated date of delivery is changed from the date of delivery determined by the LMPD or OTPD or SCID or LMPD/OTPD/SCID or other corroborating combinations thereof, to a later date of delivery as estimated, unilaterally, by ultrasound. The effect of which is to establish erroneous EDD & GA for individual pregnancies which create sub-optimal obstetric and fetal awareness which cause sub-optimal obstetric and fetal management, which causes increased medical risks, critical medical mistakes and grievous medical harms; grievous medical harms which include perinatal mortality.
The Constitution of the Kingdom of Norway
- "Abstract
Ultrasound dating-curve analysis was performed for the biparietal diameter, mean head diameter, and mean trunk diameter in individual singletons, twins, and triplets from in vitro fertilization (IVF) pregnancies and pregnancies with ultrasonographic determination of ovulation. Linear growth was found for all parameters prior to 28 weeks' conceptional age. No differences were observed among singletons, twins, or triplets. Using linear equations, no significant difference was found in systematic errors between pregnancies with a known date of conception and pregnancies dated from the last menstrual period (LMP). Pregnancies with reliable LMPs had only a slight and nonsignificant increase in random errors when compared with pregnancies from IVF. Current polynomial dating equations produced considerable systematic and random errors as well as errors related to fetal growth. Acceptable results were obtained with a new linear equation based on two examinations. We conclude that gestational age based on good menstrual records supported by a pelvic examination in the first trimester may be more reliable than even the best ultrasound method for dating." (Source: "Conceptional age, menstrual age, and ultrasound age: a second-trimester comparison of pregnancies of known conception date with pregnancies dated from the last menstrual period." Rossavik IK1, Fishburne JI. Obstet Gynecol. 1989 Feb;73(2):243-9.)
A 1992 U.K. study, Gardosi et al. 1992, identified computer-based customized fetal growth charts to account for growth variances due to physiological variables.
- "Abstract
Charts for fetal growth do not take physiological variables into account. We have therefore designed a computer-generated antenatal chart that can be easily "customised" for each indiviual pregnancy, taking the mother's characteristics and birthweights from previous pregnancies into consideration. The adjusted birthweight range expected at 40 weeks' gestation is combined with a standard, longitudinal ultrasound-derived curve for intrauterine weight gain. Review at the Queen's Medical Centre, Nottingham, UK, of 4179 pregnancies with ultrasound-confirmed dates showed that, in addition to gestation and sex, maternal weight at first antenatal-clinic visit, height, ethnic group, and parity were significant determinants of birthweight in our population. Correction factors were calculated for each of these variables and entered into a computer program to adjust the normal birthweight centile limits. With adjusted centiles we found that 28% of babies conventionally designated small for gestational age (<10th centile) and 22% of those designated large (>90th centile) were in fact within normal limits for the pregnancy. Conversely, 24% and 26% of babies identified as small or large, respectively, with adjusted centiles were "missed" by conventional unadjusted centile assessment. Adjustment for physiological variables will make assessment of fetal growth more precise and reduce unnecessary investigations, interventions, and parental anxiety." (Source: "Customised antenatal growth charts" J. Gardosi, MRCOG, A. Chang, FRCOG, B. Kalyan, MD, D. Sahota, PhD, E.M. Symonds, FRCOG. The Lancet Volume 339, No. 8788, p283–287, 1 February 1992. DOI: http://dx.doi.org/10.1016/0140-6736(92)91342-6)
A 1995 Danish study, Henricksen et al. 1995, identified that the bias induced by ultrasound dating of gestational age "can distort the relative risk of preterm or postterm delivery by 10-20%."
- Abstract
Ultrasound measurement of fetal dimensions is widely used for estimating gestational age. A little-discussed limitation of this method is that variations in fetal size at a given stage of pregnancy are converted to differences in gestational age. Factors that affect pregnancy duration often affect fetal size also. We explore how the effect of such factors may be biased when gestational age is determined by ultrasound. We selected 3,606 women with singleton pregnancies (1989-1991) who had an early ultrasound measurement of fetal biparietal diameter (BPD) and a good-quality history of last menstrual period (LMP). Using the two measures of gestational age, we estimated risk of preterm and postterm delivery for female babies vs males and for smoking women vs nonsmoking women. There was a 13% excess of preterm delivery among female babies when gestational age was determined by ultrasound, but no excess when gestational age was defined by LMP. For postterm delivery, female babies had a 19% lower risk with ultrasound-defined age, but no deficit with LMP-defined age. We found a similar bias with ultrasound in the analysis of maternal smoking. Thus, factors that reduce fetal size inflate the risk of preterm delivery and deflate the risk of postterm delivery when gestational age is based on ultrasound measurement of the fetus. This bias can distort the relative risk of preterm or postterm delivery by 10-20%. (Source: "Bias in studies of preterm and postterm delivery due to ultrasound assessment of gestational age" Tine Brink Henriksen, Allen J. Wilcox, Morten Hedegaard and Niels Jørgen Secher. Epidemiology. Vol. 6, No. 5 (Sep., 1995), pp. 533-537.)
A 1996 U.K. study, Mongelli et al. 1996, established the value of using known conception dates in conjunction with ultrasound and LMPD to establish a more accurate estimate of gestational age in individual pregnancies.
- "In view of the large error in LMP data, it is unlikely that combining menstrual dates with ultrasonographic data in fetal age estimation algorithms would improve their accuracy. With uhrasonography as reference, we have previously shown that dates derived from the given LMP may have considerable error 12: for 21.5% of pregnancies LMP dates were outside ±7 days on the basis of the dating scan. In contrast, the error of a midtrimester BPD measurement in a sample with certain conception dates that were not known to the scanner had an SD of 2.96 days, suggesting that only 1.8% of cases would have a scan dating error of >7 days. 13" (Source: "Estimating the date of confinement: Ultrasonographic biometry versus certain menstrual dates." "Mongelli, M., Wilcox, M., & Gardosi, J. (1996). American Journal of Obstetrics and Gynecology, 174(1), 278–281. p. 280)
A 1997 Danish study, Olsen & Clausen 1997, concluded that Ultrasound-based EDD is not necessarily better than LMP-based EDD.
- Introduction
"In a leaflet issued by The Midwives Information and Resource Service (MIDIRS) and the National Health Service Centre for Reviews and Dissemination, pregnant women are informed that the expected day of delivery determined on the basis of an ultrasound scan “is more accurate than using a calendar and the date of your last period”’. The information is supported by reference to the Cochrane review Routine ultrasound in early pregnancy 2. Two questions arise, however: 1. Is the statement based on the best available evidence? 2. Is the statement correct? p. 1221
Other evidence
A change of the definition of the term from a last menstrual period of 280 days to one of 283 days is supported by the largest published cohort study, comprising 427,582 singleton pregnancies with a reliable last menstrual period. The authors conclude that the “average duration from last menstrual period to vaginal birth was 282 days (median), 281 days (mean) and 283 days (mode) 5." ( p. 1221)
Conclusion
We conclude that the statement in the MIDRS leaflet regarding accuracy is not based on the best available evidence and that it may be wrong in women who have regular cycles and known first day of the last menstrual period. p. 1222
Future research
"A consequence of the above observations is that the reduced incidence of induction of labour for apparent post-term pregnancy in the routinely scanned groups presumably does not result from better gestational dating but is due to a shift of the distribution curve leaving fewer pregnancies under the tail of the curve to be labelled ‘post-term’. Furthermore, it may even be possible that a more elaborate clinical method of predicting the day of delivery based on Nagele’s old rule may be better than dating based on an ultrasound scan.
(...)
In new trials it is necessary to base the calculation of the expected day of delivery in the nonscanned arms on more elaborate methods than Nagele’s rule. First of all the number of days added to the last menstrual period should be so that the expected day of delivery is correct on average. Second, further corrections may be based on long or short cycles, known date of ovulation or known day of sexual intercourse. Third, additional information may be obtained for the individual woman so that the number of days added is corrected for her age, parity and other possible predictive factors. (p. 1222) (Source: "Routine ultrasound dating has not been shown to be more accurate than the calendar method" Olsen, O. and Aaroe Clausen, J. (1997), BJOG: An International Journal of Obstetrics & Gynaecology, 104: 1221–1222. doi:10.1111/j.1471-0528.1997.tb10965.x)
A 1997, study of Norwegian births, Campbell et al. 1997, established small for gestational age (SGA) as a risk factor for perinatal mortality in post-term births (adjusted RR 5.68; 95% CI 4.37, 7.38). Included below is the full abstract of this study.
- Abstract
OBJECTIVE: To identify factors associated with post-term birth and factors associated with adverse outcomes in post-term births.
METHODS: The sample was a 10-year cohort (1978-1987) of term (n = 379,445) and post-term (n = 65,796) births from the Medical Birth Registry of Norway. Gestational age was based on mothers' recall of the last menstrual period. Multivariate analyses included proportional hazards regression and binomial logistic regression.
RESULTS: After controlling for covariates, there was only a slightly increased risk of perinatal mortality in post-term as compared with term births (adjusted relative risk [RR] 1.11; 95% confidence interval [CI] 0.97, 1.27). For post-term births, risk factors for perinatal mortality were small size for gestational age (SGA) (adjusted RR 5.68; 95% CI 4.37, 7.38) and maternal age 35 years or older (adjusted RR 1.88; 95% CI 1.22, 2.89), whereas large size for gestational age (LGA) was a protective factor (adjusted RR 0.51; 95% CI 0.26, 1.00). Similar risk factor RRs were found for perinatal mortality in term births. Fetal distress was associated with both SGA and post-term birth; labor dysfunction and obstetric trauma were associated with both LGA and post-term birth; shoulder dystocia and maternal hemorrhage were associated with LGA only.
CONCLUSIONS: Among post-term births, maternal complications were generally associated with larger fetal size, and fetal complications were associated with smaller fetal size. The evidence for an adverse impact on perinatal mortality of post-term birth is weak once other factors are taken into account. (Source: "Post-term birth: risk factors and outcomes in a 10-year cohort of Norwegian births" Campbell MK, Ostbye T, Irgens LM. Obstet Gynecol. 1997 Apr;89(4):543-8.) - Appropriately, Campbell et al. 1997, was cited and referenced (no. 19) within Morken et al. 2014: "We hypothesized that death risk in post-term pregnancies is strongly associated with being small-for-gestational age (SGA) and that the implementation of ultrasound-based estimates of gestational age may have had a negative impact especially for the growth restricted infants being assessed as post-term later than they should."
- Strangely, this important 1997 Norwegian study of births based on the Medical Birth Registry of Norway, Campbell et al. 1997, was neither cited nor referenced within NCFM Snurra Group's Tunón et al. 1999a, a Norwegian study.
- Interestingly, Campbell et al. 1997 was cited and referenced in 2007 regarding the definition of post-term pregnancy ("4.1 Definition" p. 12) in Runa Heimstad's 2007 NTNU PhD Thesis "Post-term pregnancy", NTNU, Faculty of Medicine, Department of Laboratory Medicine, Children's and Women's Health. Sturla H. Eik-Nes of NCFM Group was a supervisor of Heimstad's 2007 NTNU PhD Thesis.
A 1998 study of Swedish births, Divon et al. 1998, established that "fetal growth restriction was independently associated with significantly higher odds ratios for both fetal and neonatal mortality rates at every gestational age examined (with odds ratios ranging from 7.1 to 10.0 for fetal death and from 3.4 to 9.4 for neonatal death)."
- Abstract
Objective: Our purpose was to examine the impact of gestational age and fetal growth restriction on fetal and neonatal mortality rates in the postterm pregnancy.
Study Design: All deliveries occurring in Sweden between Jan. 1, 1987, and Dec. 31, 1992, were evaluated for participation in this study. Data were derived from the National Swedish Medical Birth Registry. Pregnancies were selected for inclusion in the study on the basis of the following criteria: (1) singleton pregnancy, (2) reliable dates, (3) gestational age ≥40 weeks, and (4) maternal age 15 to 44 years. Fetal growth restriction was defined as birth weight <2 SD below the mean for gestational age. A total of 181,524 pregnancies met the inclusion criteria and formed the study population. Fetal and neonatal mortalities at 40 weeks' gestation were used as reference levels. Logistic regression analysis was used to estimate the independent effects of gestational age and fetal growth restriction on fetal and neonatal mortality rates.
Results: A significant rise in the odds ratio for fetal death was detected from 41 weeks' gestation and on (odds ratios 1.5, 1.8, and 2.9 at 41, 42, and 43 weeks, respectively). Odds ratios for neonatal mortality did not demonstrate a significant gestational age dependency. Fetal growth restriction was associated with significantly higher odds ratios for both fetal and neonatal mortality rates at every gestational age examined (with odds ratios ranging from 7.1 to 10.0 for fetal death and from 3.4 to 9.4 for neonatal death).
Conclusions: Postterm pregnancies have long been considered to be at high risk for adverse perinatal outcome. This study documents a small but significant increase in fetal mortality in accurately dated pregnancies that extend beyond 41 weeks of gestation. This study also demonstrates that fetal growth restriction is independently associated with increased perinatal mortality in these pregnancies. (Source: "Fetal and neonatal mortality in the postterm pregnancy: The impact of gestational age and fetal growth restriction" Michael Y. Divon, MD, Bengt Haglund, PhD, Henry Nisell, MD, PhD, Petra Olausson Otterblad, BSc, Magnus Westgren, MD, PhD. Am J Obstet Gynecol 1998;178:726-31. DOI: https://doi.org/10.1016/S0002-9378(98)70482-X)
A 1999 Australian study, Roberts et al. 1999, identified gestational age determination by ultrasound causing a GA distribution shift from 40 weeks to 38 and 39 weeks at birth/delivery, but did not make the connection with perinatal mortality rates.
- The increase in both the number and percentage of births at 38 and 39 weeks of gestation, and coincident decrease at 40 weeks, occurred among births with spontaneous onset as well as those with elective onset. Changes in gestational age determination or more accurate reporting of gestational age on the midwives data collection are likely explanations for some of the shift to earlier gestational ages. Studies consistently show that, compared with last normal menstrual period dating, early ultrasound dating results in a shift to the left in the gestational age distribution 10-11. (Source: "Trends in births at and beyond term: evidence of a change?" Christine L. Roberts, Lee Taylor, David Henderson-Smart. British Journal of Obstetrics and Gynaecology September 1999, Vol106, pp. 937-942.)
- Abstract
Objective To examine trends in the distribution of births at and beyond term in New South Wales and in particular, to determine whether any changes are associated with changes in the obstetric practices of induction and elective caesarean section.
Design Cross-sectional analytic study.
Setting New South Wales, Australia.
Population All 540,162 women delivering a singleton cephalic-presenting infant of gestational age >= 37 weeks from 1 January 1990 to 31 December 1996.
Methods Data were obtained from the New South Wales midwives data collection, a population-based surveillance system covering all births in New South Wales. The data were analysed to examine changes over time and associations between gestational age, maternal factors and onset of labour.
Main outcome measures Induction of labour and elective caesarean section rates.
Results From 1990 to 1996 there was a significant decrease in births reported as 40 weeks of gestation, from 35,670 (46.3%) to 30,651 (40.3%). These declines were offset by significant increases in births at 38 and 39 weeks. Births >=42 weeks declined from 3321 (4.6%) to 2132 (2.8%). The decline in prolonged pregnancies was associated with increasing induction rates at 41 weeks. The re-distribution of some births from 40 to 38-39 weeks was associated with increasing rates of elective caesarean sections and induction at 38 and 39 weeks, and increasing maternal age.
Conclusions Clinicians appear to be implementing the recommendations of randomised controlled trials to offer induction after 41 weeks of gestation. However the trend of performing elective caesarean sections at earlier gestational ages may be unnecessarily putting some infants at increased risk of respiratory morbidity.
A 1999 Norwegian study, Tunón et al. 1999a, originated as Paper III: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" within Katarina Tunón's 1999 NTNU PhD Thesis which was supervised by NCFM Snurra Group members Sturla H. Eik-Nes and Per Grøttum. NCFM Snurra Group's Tunón et al. 1999a found "no indication of any adverse consequence of the routine scan and change of estimated day of delivery" despite evidence to the contrary. Tunón et al. 1999a articulated the problem of discrepant LMPD-based GA and ultrasound-based GA in their introduction. However, Tunón et al. 1999a excluded the compounding issue that BPD is a problematic, unreliable estimator of GA or EDD during routine ultrasound exams because BPD has problems with non-standard fetal head shapes. Moreover, fetal head sizes are not all the same (i.e. accurately average) for a given GA due to random fetal growth velocity variances and/or fetal pathology; and, these variances get translated directly into GA variances (i.e., GA errors). HC should be used instead of, or in conjunction with BPD, because HC is a more robust estimator and is practically insensitive to fetal head shape for GA or EDD estimations.
- "Introduction Several studies have indicated that ultrasonic measurement of the BPD is better than the last menstrual period (LMP) for predicting the day of delivery 1–4. The ultrasound method regards all fetuses with the same BPD as being the same age. Early impairment of fetal growth might therefore influence the accuracy of the method. Impairment of fetal growth early in pregnancy may be caused by chromosomal aberrations, fetal malformations or infections, or it may be an isolated feature. Growth-restricted fetuses will have a smaller BPD than expected, not because they are younger but because they are growth-restricted. A consequence of this early growth restriction might be to change the day of delivery as estimated by ultrasound, to a later date than the day of delivery that is determined in accordance with the LMP. Such an extension of the estimated day of delivery might therefore lead to a falsely lower gestational age and a later detection or no detection at all of the growth restriction, with the possible consequence of adverse obstetric management of the pregnancy."
ABSTRACT "Conclusion There was no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population. However, further studies are required to explore this phenomenon." (Source: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" Tunon K, Eik-Nes SH, Grøttum P. Ultrasound Obstet Gynecol 1999; 14: 17–22., p. 17
Discussion Conclusion "In conclusion, there is no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population. However, further studies are required to explore this phenomenon." (Source: ibid., p. 22)
The excerpt below is NCFM eSnurra Group at their science-bending best. This is where NCFM eSnurra Group asserted:
- DISCUSSION "In this study, based on a large, primarily non-selected population of fetuses without anomalies, no indication of adverse fetal outcome was found that could be linked to changing the estimated day of delivery as determined by ultrasound to more than 14 days later than the day of delivery that was in accordance with the LMP." (Source: ibid., p.21)
- Statistics for the number of days LMPD-based EDD was changed by more than 14 days later by ultrasound for the 7 dead babies.
Number of days later LMPD-based EDD was changed by ultrasound: 24, 16, 37, 24, 18, 43, 17
Mean: 25.6 days
Median: 24 days
Mode: 24 days
Minimum: 16 days
Maximum: 43 days
Standard Deviation: 10.5 days
Range: 28 days
- "Despite the lack of distinctive pathological findings in the deaths of fetuses in the study group, the estimated relative risk of perinatal death of 2.07 with a confidence interval of 0.93–4.61 should lead to further investigations of the frequency and causes of perinatal mortality in this group of patients. It is possible that the extensive discrepancy in gestational age is a marker for fetuses that might benefit from closer monitoring." (Source: ibid., p.21)
The excerpt above from Tunón et al. 1999a clearly identified an "indication" of perinatal death which would have to be considered as an "indication" of an"adverse consequence of the routine scan and change of estimated day of delivery," which begs the question: If "the estimated relative risk of perinatal death of 2.07 with a confidence interval of 0.93–4.61" resulting from the evidence of 7 dead fetuses/babies whose EDDs had been changed by ultrasound an average of 25.6 days later (median of 24 days later) was not an "indication" of "an adverse consequence of the routine scan and change of estimated day of delivery," then what was it? Also, the excerpt above indicates "the estimated relative risk of perinatal death of 2.07 with a confidence interval of 0.93–4.61 should lead to further investigations of the frequency and causes of perinatal mortality in this group of patients. " Consequently, there had to have been some sort of an "indication" for NCFM Snurra Group to have stated "further investigations" of the identified relative risk of perinatal death of 2.07, yet NCFM eSnurra Group's Tunón et al. 1999a explicitly concluded and stated: "no indication of adverse fetal outcome was found. " For contrast, included below is the stated aim of Tunón et al. 1999a (i.e., Paper III) from Tunon's 1999 NTNU PhD Thesis.
- "Further aims were to evaluate the possibility of an increased risk for adverse fetal outcome when the predicted day of delivery as estimated by ultrasound is more than 14 days later than the predicted day of delivery as estimated by the last menstrual period (Paper III)." (Source: Katarina Tunon 1999 NTNU PhD Thesis "Ultrasound and Prediction of Gestational Age" "SUMMARY: Aims," p. 9. Norwegian University of Science and Technology (NTNU), National Center for Fetal Medicine, Department of Gynecology and Obstetrics, ISBN 82-519-1260-1, ISSN 0805-7680)
Compare the "Objective" and "Results" sections (below) from the ABSTRACT in Tunón et al. 1999a.
- Objective To evaluate the effect on fetal outcome of changing the estimated day of delivery as calculated according to ultrasound measurements more than 14 days later than the day estimated according to the last menstrual period.
- Results Changing the estimated day of delivery, based on the ultrasound evaluation, to a date 14 days later than the day of delivery as estimated according to the last menstrual period did not influence the risk of abortion, perinatal death or transferral to the neonatal intensive care unit. There was a difference of 3 days in the accuracy of the prediction of day of delivery between the two groups. There was a greater number of infants with a birth weight below 2500 g in the study group, but no difference was found between the groups in the number of infants with a birth weight < 2 SD from the mean according to the ultrasound estimate.
- Objective: "more than 14 days later"
- Design: "more than 14 days later"
- Results: "to a date 14 days later"
- Conclusion: "the routine scan and change of estimated day of delivery"
The downstream effects of Tunón et al. 1999a excluding the "relative risk of perinatal death of 2.07" from the Results and Conclusion sections is evidenced in a 1999 Swedish opinion article, Persson 1999, titled "Ultrasound dating of pregnancy - still controversial?" published in Ultrasound In Obstetrics and Gynecology (the official journal of ISUOG) cited Tunón et al. 1999a and Tunón et al. 1999b (citations 2 and 3 in the excerpt below) without any mention of the "relative risk of perinatal death of 2.07" identified in Table 2 of Tunón et al. 1999a. Interestingly, Sturla H. Eik-Nes head of NCFM Group (Trondheim), is a coauthor of Tunón et al. 1999a and Tunón et al. 1999b as well as principal supervisor of Katarina Tunón's 1999 NTNU PhD Thesis; moreover, and at that time, Sturla H. Eik-Nes was President ISUOG (1998 - 2002).
- "Two studies from Trondheim reveal, first, that there is no increased risk of adverse fetal outcome or impaired fetal growth in a group of babies whose date of delivery had been postponed more than 14 days compared with Naegele's rule." Second, there is no increased risk of low Apgar score or referral to the neonatal intensive care unit in babies who are delivered at term judged by ultrasound and who would be post-term according to the last menstrual period 2, 3." [Note: Citations 2 and 3 reference Tunón et al. 1999a and Tunón et al. 1999b, respectively.] (Source: Opinion: "Ultrasound dating of pregnancy - still controversial?" P.-H. Perrson. Cura Kliniken (Malmo, Sweden) Ultrasound Obstet Gynecol 1999;14:9-11. p. 9-10)
- "The Norwegian study shows that changing the expected date of delivery by ultrasound has no adverse effect at all." (Source: ibid., p. 11)
- "It has been reported that infants whose gestational age according to ultrasound fetometry in early pregnancy (GA-U) is less than the gestational age according to LMP (GA-LMP) are at increased risk of low birth weight 12-15 and intrauterine growth restriction 10, 12, 13, 15. These findings suggest that for some newborn infants who were considered small‐for‐gestational age at birth (SGA), the growth restriction was already present in early pregnancy. In a study comprising 16 469 pregnancies, Nguyen et al. 13 reported that a discrepancy between GA-LMP and GA-U also indicated an increased risk of fetal death (especially in combination with high maternal alpha‐fetoprotein). The authors concluded that such a discrepancy might indicate early fetal pathology. However, investigating 15 241 pregnancies, Tunon et al. 14 found no increased risk for perinatal death in pregnancies in which the GA-U was more than 14 days less than the GA-LMP. In another Norwegian study 15 based on 16 302 pregnancies, a highly significantly increased risk for perinatal death was found in such pregnancies." (Source: "Increased risk of perinatal/neonatal death in infants who were smaller than expected at ultrasound fetometry in early pregnancy" K. Källén. Ultrasound in Obstetrics & Gynecology Volume 24, Issue 1 July 2004 Pages 30–34 First published: 26 May 2004) [Note: Citations:"13 Nguyen T, Larsen T, Engholm G, Møller H. -. Br J Obstet Gynaecol 2000; 107: 1122–1129.; "14 Tunón K, Eik-Nes SH, Grøttum P. Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate. Ultrasound Obstet Gynecol 1999; 14: 17–22.; "15 Nakling J, Backe B. Adverse obstetric outcome in fetuses that are smaller than expected at second trimester routine ultrasound examination. Acta Obstet Gynecol Scand 2002; 81: 846–851.]"
- "The purpose of this study was to evaluate the possibility of an increased risk of adverse fetal outcome and impaired fetal growth when the predicted day of delivery as estimated by ultrasound was more than 14 days later than the predicted day of delivery as estimated by the LMP."
- DISCUSSION "In this study, based on a large, primarily non-selected population of fetuses without anomalies, no indication of adverse fetal outcome was found that could be linked to changing the estimated day of delivery as determined by ultrasound to more than 14 days later than the day of delivery that was in accordance with the LMP."
- Paper III, NCFM Snurra Group's Tunón et al. 1999a, "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate"
Abstract Conclusion "There was no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population."
Discussion Conclusion "In conclusion, there is no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population. However, further studies are required to explore this phenomenon."
Paper IV, NCFM Snurra Group's Tunón et al. 1999b, "Fetal outcome in pregnancies defined as post-term according to the last menstrual period estimate, but not according to the ultrasound estimate"
Abstract Conclusion "The effect of ultrasound in changing the estimated day of delivery to a later date leading to pregnancies becoming post-term according to the last menstrual period estimate but not according to the ultrasound estimate does not have any adverse consequences for the fetal outcome. However, there seems to be an increased risk for adverse consequences for pregnancies that are post-term according to the ultrasound estimate."
"Discussion Conclusion In conclusion, using ultrasound to correct dates and postpone the estimated day of delivery leads to some pregnancies being defined as post-term according to the last menstrual period estimate but not as post-term according to the ultrasound estimate [and some pregnancies being defined as post-term according to the ultrasound estimate]. However, managing these pregnancies according to the ultrasound estimate does not have any adverse consequence on the fetal outcome."
A 2000 Danish study, Nguyn et al 2000, of 16,469 pregnancies, found a positive discrepancy between LMP-based GA and BPD-based GA of >8 days is associated with:
- increased risk of death; OR = 2.2 [1.6–3.1]
- increased risk of preterm delivery; OR = 1.7 [1.4–2.0]
- increased risk for a birth-weight < 2500 g; OR = 1.7 [1.4–2.1]
- increased risk of low birthweight for gestational age (SGA); OR = 1.4 [1.2–1.7]
- and, high maternal alpha-fetoprotein (MoM > 2) was found to increase each risk above from 3X to 6X.
[Note: The group of (GALMP – GABPD) ≤ 7 days was used as reference (OR = 1)]
(Source: "A discrepancy between gestational age estimated by last menstrual period and biparietal diameter may indicate an increased risk of fetal death and adverse pregnancy outcome" Tri huu Nguyen, Torben Larsen, Gerda Engholm, Henrik Møller. BJOG: An International Journal of Obstetrics & Gynaecology Volume 107, Issue 9. September 2000 Pages 1122–1129. http://dx.doi.org/10.1111/j.1471-0528.2000.tb11111.x)
- Results Section: "For example, the OR for stillbirth/neonatal death was 1.7 among infants whose GA-U was 14 days or more less than their GA-LMP, compared with infants with smaller adjustments of their gestational age. The risk for stillbirth/neonatal death increased linearly with the discrepancy between GA-LMP and GA-U. When infants who were SGA at birth were excluded, there was still an increased risk for perinatal/neonatal death when GA-U was at least 5 days less than GA-LMP, but no linear relationship between negative adjustment and perinatal/neonatal death was demonstrated."
- Abstract
Objective To determine if the discrepancy between gestational age estimated by last menstrual period and by biparietal diameter (GALMP− GABPD) is associated with adverse pregnancy outcome.
Design Population/-based follow up study.
Population Singleton pregnancies were studied when a reliable date of last menstrual period and biparietal diameter measured between 12 and 22 weeks of gestation was available (n= 16,469).
Methods Logistic regression analysis and Kaplan-Meier survival analysis were used to analyse the association between GALMP− GABPD and adverse pregnancy outcome.
Main outcome measures Adverse outcome was defined as abortion after 12 weeks of gestation, stillbirth or postnatal death within one year of birth, delivery < 37 weeks of gestation, a birthweight < 2500 g or a sex-specific birthweight lower than 22% below the expected.
Results The risk of death was more than doubled if GA_LMP − GA_BPD of ≥ 8 days was compared with GA_LMP− GA_BPD of < 8 days (OR 2.2; 95% CI 1.6–3.1). The risk of death was a factor of 6.1 higher if GA_LMP− GA_BPD of ≥ 8 days was combined with increased (> 2 × multiple of median) maternal alphafetoprotein measured in the 2nd trimester.
Conclusions A discrepancy between GALMP and GABPD generally reflects the precision of the two methods used to predict term pregnancy. However, a positive discrepancy of more than seven days, particularly with high maternal alpha-fetoprotein, might indicate intrauterine growth retardation and an increased risk of adverse perinatal outcome.
A 2000 Swedish PhD Thesis, Clausson 2000, identified and discussed risk factors for SGA fetuses of "three distinct subgroups," highlighting the importance of identifying SGA fetuses at risk.
- DISCUSSION
Risk factors for SGA vary by gestational age, and SGA infants have higher death rates than AGA infants at all gestational ages. In post-term pregnancy there is an increased rate of SGA births, which appears to explain the increased risk of stillbirth observed among post-term pregnancies. Genetic factors appear to influence fetal growth as well as gestational length. We find no evidence that caffeine consumption during pregnancy influences fetal growth. Maternal anthropometrics influence risk of SGA birth, as commonly defined by population-based birthweight standards. Compared with SGA defined by population based birthweight standards, SGA defined by birthweight curves standardised for maternal height, weight, parity and ethnicity (”customised” birthweight standards) increases the strength of the associations between SGA birth and adverse outcomes, such as stillbirth. (Source: "Risk Factors and Adverse Pregnancy Outcomes in Small-for-Gestational-Age Births" Britt Clausson. Dissertation for the Degree of Doctor of Philosophy, Faculty of Medicine in Obstetrics and Gynecology presented at Uppsala University in 2000, ISSN 0282-7476, ISBN 91-554-4858-5)
"Risk factors for SGA.
Though the aetiology of SGA is complex, three distinct subgroups can be discerned: the constitutionally small, healthy infant, the infant with chromosomal or other dysfunctions that exist from the onset of pregnancy, and the growth restricted, nonmalformed infant. While risk factors for chromosomal and other inborn dysfunctions naturally exist, they are beyond the scope of the present study. Some previously described risk factors for SGA are merely risk factors for constitutional, healthy smallness, whereas others are risk factors for IUGR." (Source: ibid.)
A 2002 Canadian study, Yang et al. 2002, concluded: "early ultrasound scan-based reclassification of gestational age results in a substantial increase in the prevalence of preterm births."
- Abstract
OBJECTIVE: Early ultrasound scanning estimation of gestational age is known to increase the reported preterm delivery rate (<37 completed weeks) compared with estimation by date of the last normal menstrual period, but it is unclear how this systematic difference arises.
STUDY DESIGN: This study was a hospital-based study of 44,623 women who delivered a live-born or stillborn infant between January 1, 1978, and March 31, 1996, and who had both last normal menstrual period-based and early (usually at 16-18 weeks) ultrasound scan-based gestational age estimates. Cross-classification of the 2 estimates by completed weeks was used to examine the direction and magnitude of the differences between them and to compare the resulting classifications of preterm birth.
RESULTS: The early ultrasound scan-based gestational age distribution was shifted uniformly to the left (ie, lower gestational age) relative to the last normal menstrual period gestational age distribution; the early ultrasound scan-based preterm delivery rate was 9.1%, which was 19.5% (n = 659 births) higher than the 7.6% rate by last normal menstrual period (P <.0001). The last normal menstrual period estimate exceeded the early ultrasound scan estimate far more often than the reverse, up to and including early ultrasound scan estimates of 40 weeks. No concentration of 4-week discrepancies was observed in either direction, as would be expected with random or systematic errors in recall of the last normal menstrual period. The absolute number of births at 37 to 39 weeks of gestation (by last normal menstrual period) that were reclassified as preterm (n = 1206 births) was much higher than the number of preterm births at 34 to 36 weeks of gestation that were reclassified as term (n = 581 births). The net increase of 625 preterm births (from 581 to 1206 births) that resulted from reclassification of births at 37 to 39 last normal menstrual period weeks accounted for 95% of the total 659-birth increase in early ultrasound scan-based preterm births at all last normal menstrual period gestational ages.
CONCLUSION: Early ultrasound scanning reduces the gestational age estimate across the entire gestational age range; early ultrasound scan-based reclassification of gestational age results in a substantial increase in the prevalence of preterm births. Small downward reclassifications exceed upward reclassifications of similar magnitude, which is consistent with previous reports that delayed (>14 days) ovulation is more frequent than early (<14 days) ovulation. (Source: "How does early ultrasound scan estimation of gestational age lead to higher rates of preterm birth?" Yang H, Kramer MS, Platt RW, Blondel B, Bréart G, Morin I, Wilkins R, Usher R. Am J Obstet Gynecol. 2002 Mar;186(3):433-7. DOI: http://dx.doi.org/10.1067/mob.2002.120487)
A 2002 Canadian study, Blondel et al. 2002, which included 4 of the coauthors of Yang et al. 2002, showed post-term births >=41 weeks and >=42 weeks decreased by 46% and 70%, respectively and, preterm births <37 weeks increased 20% when ultrasound was used to estimate gestational age, thereby demonstrating ultrasound-based GA has a major impact on the rate of post-term and preterm birth classifications.
- "We compared rates of preterm and postterm birth according to six algorithms for gestational age (GA) estimates based on last menstrual period (LMP) and early ultrasound (EUS): LMP alone, LMP if the discrepancy between the two estimates was within 14 days and otherwise EUS (14-day rule), a 10-day rule, a seven-day rule, a three-day rule and EUS alone. In a sample of 44,623 births in a Canadian tertiary hospital, the choice of algorithms makes a substantial impact on both preterm and postterm birth rates, even when EUS was used for discrepancies over two weeks." [Note: EUS = early ultrasound in Canada]
Abstract
Rates of preterm and postterm birth estimated from LMP or US (n = 44,623), only LMP and US are included below.
Preterm birth (%) LMP US Change (%)
<32 weeks 1.3 1.3 0.0
<34 weeks 2.2 2.3 4.5
<37 weeks 7.6 9.1 19.7
Postterm birth (%)
>=41 weeks 20.9 11.2 -46.4
>=42 weeks 6.4 1.9 -70.3
(Source: Blondel et al. 2002, LMP & USE extracted from Table 1, p . 719)
Results Concordance between LMP and EUS estimates was within three days in 46.6% of births, within seven days in 72.4% of births , within 10days for 83.4% of births and within 14 days for 90.7% of births. - Discussion Our results show that the use of EUS estimates of GA has a major impact on the rate of postterm birth; the impact is less forpreterm birth and negligible for births < 34 weeks. No impact was discernible for births < 32 weeks, because the number of reclassified birthswas very small. The effect of EUS on the proportion of deliveries < 37 weeks was apparent even when EUS was used for discrepancies over twoweeks and it was large with all the studied strategies for the proportion of births >= 41 or >= 42 weeks. (Source: "Algorithms for combining menstrual and ultrasound estimates ofgestational age: consequences for rates of pretermand postterm birth" Beatrice Blondel, Isabelle Morin, Robert W. Platt, Michael S. Kramer, Robert Usher, Gerard Bréart. BJOG: an International Journal of Obstetrics and Gynaecology June 2002, Vol. 109, pp. 718–720
A 2002 U.S. study, Smith-Bindman et al, 2002, concluded 2 ultrasound exams can estimate neonatal morbidity even when GA is unknown. Interestingly, 1 ultrasound exam combined with a factual LMPD/OTPD/SCID-based GA can do the same thing, but with increased precision and at no additional cost, as Laila & Edward had proved, just before they were ignored into harms' way.
- Abstract
PURPOSE: To determine whether fetal growth measured at serial ultrasonographic (US) examinations can predict neonatal morbidity, independent of whether gestational age is known.
MATERIALS AND METHODS: Women (n = 321) who had singleton pregnancies and underwent two or more second- or third-trimester obstetric US examinations were included in a retrospective cohort analysis. Inadequate fetal growth was defined as growth at or below the 10th percentile. The relative risk of each poor outcome was calculated for fetuses with inadequate growth, compared with the risk for fetuses with normal growth.
RESULTS: Inadequate fetal growth was associated with 3.9 times the risk of a birth weight less than 2,500 g, 17.7 times the risk of a birth weight less than the 3rd percentile for gestational age, 2.3 times the risk of preterm birth, 2.6 times the risk of a long newborn hospital stay, and 3.6 times the risk of neonatal intensive care unit admission. After adjusting for confounding variables, including fetal weight, fetal growth remained a significant predictor of small birth size and poor outcomes. Inadequate growth predicted the risk of poor outcomes, even when gestational age was unknown. When inadequate growth was used to identify fetuses at risk, 21%–67% of neonates who were small at birth or had poor outcomes were identified at false-positive rates of only 5%–9%. For all outcomes, inadequate growth enabled identification of more fetuses with poor birth outcomes than low estimated fetal weight.
CONCLUSION: Morbidity is significantly increased among fetuses who demonstrate less than expected growth. Growth between two US examinations can be used to estimate the risk of neonatal morbidity, even when gestational age is unknown. (Source: "US evaluation of fetal growth: prediction of neonatal outcomes" Smith-Bindman R1, Chu PW, Ecker JL, Feldstein VA, Filly RA, Bacchetti P. Radiology. 2002 Apr;223(1):153-61.https://doi.org/10.1148/radiol.2231010876)
A 2002 Norwegian study, Nakling & Backe 2002, completely contradicts the conclusion of the Norwegian study, Tunón et al. 1999a, as is made clear in the Abstract (below). The main results of Nakling & Backe 2002 (Paper I) were summarized on page 25 of Nakling's 2004 NTNU PhD Thesis as follows:
- "In 1,133 pregnancies (7%) the EDD was postponed with more than 14 days. The central finding is that these pregnancies carry a statistically significant increased risk for perinatal death, preterm birth, SGA and low birthweight. This effect is independent of smoking, age, parity and major anomalies (included chromosomal aberrations). Also, the effect is not associated with irregular ovulation due to recent OC use." (Source: Jakob Nakling, 2008 NTNU PhD Thesis (p. 25). "Results and consequences of routine ultrasound screening in pregnancy: A geographic based population study" Norwegian University of Science and Technology, Faculty of Medicine, Department of Laboratory Medicine, Children’s and Women’s Health. ISBN: 82-471-8006-5, ISSN: 1503-8181)
- Abstract
Background. Adverse obstetric outcome in fetuses that are smaller than expected at second trimester routine ultrasound examination.
Aim. To assess the obstetric outcome when the interval between the estimated date of delivery by last menstrual period and the estimated date of delivery by second trimester ultrasound exceeds 14 days.
Materials and methods. Population-based prospective cohort study. Included were all women (n = 16 302) with a singleton pregnancy, in one Norwegian county from 1989 to 1999, with a reliable menstrual history and whose second trimester ultrasound examination was conclusive with a 35–60-mm biparietal diameter.
Results. Adverse outcome was defined as preterm birth (< 37 weeks), perinatal death, low birthweight (< 2500 g) and small-for-gestational age (< 2 standard deviation). The risk for perinatal death (odds ratio = 2.3), preterm birth (odds ratio = 1.7), low birth weight (odds ratio = 1.5), and small-for-gestational age (odds ratio = 1.5) was highly significantly increased in deliveries where the discrepancy between the two terms was more than 14 days. The increased risk is not explained by differences in parity, maternal age, smoking, fetal malformations, or use of oral contraceptives before pregnancy.
Conclusion. Fetuses that are smaller than expected at the mid-second trimester ultrasound corresponding to a discrepancy of more than 14 days have an increased risk for adverse obstetric outcome. (Source: "Adverse obstetric outcome in fetuses that are smaller than expected at second trimester routine ultrasound examination" Nakling J, Backe B. Acta Obstet Gynecol Scand 2002; 81: 846–851)
A 2002 Swedish Study, Källén 2002, showed systematic errors, erroneous adjusted dates, are inherent in the ultrasound method of predicting date of delivery.
- Abstract
Objective To detect possible sources of bias in ultrasound prediction of gestational age
Subjects and methods Using the Swedish Medical Birth Registry, 571 617 women were identified who were delivered between 1990 and 1997 and who had obtainable information on last menstrual period and expected date of delivery according to ultrasound
Results Male fetuses were more likely than females to be judged older than the last menstrual period date suggested at early fetometry. The estimated magnitude of the systematic error by infant gender corresponded to 1.5 days. Similarly, the fetuses of young women, multiparous women, smokers and women with low educational level were at increased risk of being smaller than expected at ultrasound examination in early pregnancy. A strong association was seen between adjustments of expected date of delivery −7 days or more and small-for-gestational age according to ultrasound at birth. Compared to singleton pregnancies, twin pregnancies were more likely to be judged more progressed at ultrasound fetometry than the last menstrual period date suggested.
Conclusions Compared to last menstrual period estimates, routine ultrasound measurements to predict date of delivery are comparatively reliable but systematic errors are inherent in the method. The erroneous adjusted dates may be due to incorrect measurements or systematic bias (e.g. gender), but they are also likely to reflect early growth restriction (e.g. in the case of maternal smoking and small-for-gestational age).Further studies are needed to investigate whether the systematic errors in ultrasound prediction of gestational age could lead to suboptimal obstetric management in adjusted pregnancies. (Source: "Mid-trimester ultrasound prediction of gestational age: advantages and systematic errors" Dr K. Källén. Ultrasound in Obstetrics & Gynecology Volume 20, Issue 6, December 2002. Pages 558–563. DOI: 10.1046/j.1469-0705.2002.00855.x)
A 2004 Swedish study, Källén 2004, followed Källén 2002 (above) and showed the risk for stillbirth/neonatal death increased linearly with the size of the discrepancy between LMP-based GA and Ultrasound-based GA. When infants who were SGA at birth were excluded, there was still an increased risk for perinatal/neonatal death when discrepancy was at least 5 days less than LMP-based GA, but no linear relationship between negative adjustment and perinatal/neonatal death was demonstrated. Moreover, Källén 2004 explained the association between adverse outcomes and adjustment of GA via ultrasound is likely to be underestimated given the misclassificaitons resulting from reliability of self-reported LMPD recall occurred to the same extent in both groups (i.e., LMP-based GA and ultrasound-adjusted GA) will therefore bias towards the null, ergo non-differential misclassifications (i.e., no LMPD recall bias).
- Introduction: It has been reported that infants whose gestational age according to ultrasound fetometry in early pregnancy (GA-U) is less than the gestational age according to LMP (GA-LMP) are at increased risk of low birth weight 12 –15 and intrauterine growth restriction 10,12,13,15. These findings suggest that for some newborn infants who were considered small-for-gestational age at birth (SGA), the growth restriction was already present in early pregnancy. In a study comprising 16 469 pregnancies, Nguyen et al. 13 reported that a discrepancy between GA-LMP and GA-U also indicated an increased risk of fetal death (especially in combination with high maternal alpha-fetoprotein). The authors concluded that such a discrepancy might indicate early fetal pathology. However, investigating 15 241 pregnancies, Tunon et al. 14 found no increased risk for perinatal death in pregnancies in which the GA-U was more than 14 days less than the GA-LMP. In another Norwegian study 15 based on 16 302 pregnancies, a highly significantly increased risk for perinatal death was found in such pregnancies.
- Results: "For example, the OR for stillbirth/neonatal death was 1.7 among infants whose GA-U was 14 days or more less than their GA-LMP, compared with infants with smaller adjustments of their gestational age. The risk for stillbirth/neonatal death increased linearly with the discrepancy between GA-LMP and GA-U. When infants who were SGA at birth were excluded, there was still an increased risk for perinatal/neonatal death when GA-U was at least 5 days less than GA-LMP, but no linear relationship between negative adjustment and perinatal/neonatal death was demonstrated."
- Discussion: "This study confirms the results of Nguyen et al. 13 and Nakling and Backe 15 of an association between perinatal/neonatal death and a shorter gestational age according to ultrasound than the LMP-based estimate. Tunón et al. 14 found no such statistically significant association, but it should be noted that their study was based on 47 perinatal deaths, compared with 188 deaths in the investigation of Nguyen et al. 13 and the 3338 deaths in the current study." (Source: "Increased risk of perinatal/neonatal death in infants who were smaller than expected at ultrasound fetometry in early pregnancy" K. Källén. Ultrasound in Obstetrics & Gynecology Volume 24, Issue 1 July 2004 Pages 30–34 First published: 26 May 2004) [Note: Citations:"13 Nguyen T, Larsen T, Engholm G, Møller H. -. Br J Obstet Gynaecol 2000; 107: 1122–1129.; "14 Tunón K, Eik-Nes SH, Grøttum P. Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate. Ultrasound Obstet Gynecol 1999; 14: 17–22.; "15 Nakling J, Backe B. Adverse obstetric outcome in fetuses that are smaller than expected at second trimester routine ultrasound examination. Acta Obstet Gynecol Scand 2002; 81: 846–851.]"
- "The information on LMP used in this study was based on self-reported information obtained at the antenatal units and must be considered somewhat unreliable. However, the misclassification bias is non-differential as this information is obtained in early pregnancy and could not be biased by the pregnancy outcome. Errors of this type would bias the results towards unity. Thus, the association between adverse pregnancy outcome and adjustment of gestational age at ultrasound examination is likely to be underestimated, and would have been even more persuasive if putative erroneous LMP dates could be detected and excluded." (Source: ibid., p. 33)
ABSTRACT
Objectives To investigate if there is an association between perinatal/neonatal death and a discrepancy between gestational age by ultrasound fetometry in early pregnancy (GA-U) and gestational age by last menstrualperiod (GA-LMP), and to investigate possible causes for such an association.
Methods The Swedish Medical Birth Registry was used to identify singleton pregnancies with information available on GA-LMPand GA-U that were delivered in Sweden between 1990 and 2000. A total of 718 011 pregnancies was included and information on the pregnancy and delivery was obtained from the National Board of Health.
Results Infants with a GA-U at least 7 days less than the GA-LMP were at increased risk for stillbirth (odds ratio(OR), 1.45; 95% CI, 1.32–1.58), neonatal death within 1 month (OR, 1.87; 95% CI, 1.67–2.09), Apgar score< 7 at 5 min (OR, 1.18; 95% CI, 1.11–1.24), birth weight< 2500 g (OR, 1.48; 95% CI, 1.43–1.52), and preterm birth < 37 weeks (OR, 1.45; 95% CI, 1.42–1.49). The association between a postponed expected date of delivery and perinatal/neonatal death increased with gestational length and was especially pronounced among infants who were born after at least 40 completed weeks of pregnancy (GA-U).
Conclusions A discrepancy between GA-U and GA-LMP may indicate early disturbances in fetal/placental development. Furthermore, it can be speculated that, as the risk significantly increased with gestational duration, at least a part of the increased risk for poor pregnancy outcome in adjusted pregnancies was due to consequences of true post-term pregnancies not being recognized as such. (Source: ibid., p. 33)
A 2005 Swedish study, Lindqvist & Molin 2005, "found an awareness of SGA before delivery, in combination with a structured program of surveillance for those identified as SGA, was related to a four-fold lowered risk of adverse fetal outcome. " (Source: "Does antenatal identification of small-for-gestational age fetuses significantly improve their outcome?" . G. Lindqvist, J. Molin. Ultrasound in Obstetrics & Gynecology Volume 25, Issue 3 March 2005. Pages 258–264. https://doi.org/10.1002/uog.1806. First published: 17 February 2005)
- Abstract
Objectives Most obstetric clinics have a program for the identification of small-for-gestational age (SGA) fetuses because of the increased risk of fetal complications that they present. We have a structured model for the identification and follow-up of SGA pregnancies. We aimed to determine whether the recognition of SGA antepartum improves fetal outcome.
Methods All pregnancies at Malmö University Hospital from 1990 to 1998 (n = 26 968) were reviewed. SGA fetuses identified prior to delivery (n = 681) were compared with those not identified (n = 573). Also, all pregnancies with SGA fetuses were compared with those appropriate-for-gestational age (AGA) (n= 24 585). The risk of serious fetal complications (hypoxic encephalopathy grade 2 or 3, intracranial hemorrhage, Apgar score <4 at 5 min, neonatal convulsions, umbilical pH <7.0, cerebral palsy, mental retardation, stillbirth, intrapartum or infant death) was assessed with cross-tabulation and logistic regression analysis, adjusted for gestational age and degree of SGA.
Results When compared with SGA fetuses identified before delivery (54%), SGA fetuses not identified before delivery were characterized by a four-fold increased risk of adverse fetal outcome (odds ratio, 4.1; 95% CI, 2.5–6.8). Similarly, compared with AGA fetuses, SGA fetuses were associated with a four-fold increased risk of serious fetal complications.
Conclusions A structured antenatal surveillance program for fetuses identified as SGA results in a lower risk of adverse fetal outcome, compared with cases of SGA fetuses not identified antepartum.
A 2005 Canadian study, Morin et al. 2005, concluded that "although positive differences between menstrual and early ultrasound‐based gestational age often indicate erroneous menstrual dates due to delayed ovulation, erroneous recall of the last period, missed miscarriage or other explanations, they are also associated with early fetal growth restriction, a consequently smaller biparietal diameter and systematic under‐estimation of the true gestational age."
- Abstract
Objectives To assess the association between maternal and fetal characteristics and discrepancy between last normal menstrual period and early (<20 weeks) ultrasound-based gestational age and the association between discrepancies and pregnancy outcomes.
Design Hospital-based cohort study.
Setting Montreal, Canada.
Sample A total of 46,514 women with both menstrual- and early ultrasound-based gestational age estimates.
Main outcome measures Positive (last normal menstrual period > early ultrasound, i.e. menstrual-based gestational age is higher than early ultrasound-based gestational age, so that the expected date of delivery is earlier with the menstrual-based gestational age) discrepancies ≥+7 days, mean birthweight, low birthweight, stillbirth and in-hospital neonatal death.
Results Multiparous mothers and those with diabetes, small stature or high pre-pregnancy body mass index were more likely to have positive discrepancies. The proportion of women with discrepancies ≥+7 days was significantly higher among chromosomally malformed and female fetuses. The mean birthweight declined with increasingly positive differences. The risk of low birthweight was significantly higher for positive differences. Associations with fetal growth measures were more plausible with early ultrasound estimates.
Conclusions Although most discrepancies between last normal menstrual period- and early ultrasound-based gestational age are attributable to errors in menstrual dating, our results suggest that some positive differences reflect early growth restriction.
(Source: "Determinants and consequences of discrepancies in menstrual and ultrasonographic gestational age estimates" Isabelle Morin, Lucie Morin, Xun Zhang, Robert W. Platt, Béatrice Blondel, Gérard Bréart, Robert Usher, Michael S. Kramer. BJOG An Interntional Journal of Obstetrics & Gynecology Volume 112, Issue 2 February 2005. Pages 145–152. First published: 3 November 2004. DOI: 10.1111/j.1471-0528.2004.00311.x) - "In conclusion, although positive differences between menstrual and early ultrasound‐based gestational age often indicate erroneous menstrual dates due to delayed ovulation, erroneous recall of the last period, missed miscarriage or other explanations, they are also associated with early fetal growth restriction, a consequently smaller biparietal diameter and systematic under‐estimation of the true gestational age. These findings should be taken into account when interpreting studies of potential risk factors for preterm birth when those studies base their gestational age estimates on early ultrasound, particularly for those risk factors (like maternal short stature and severe pregnancy‐induced hypertension and fetal sex and chromosomal malformations) that restrict fetal growth early in gestation. Awareness of these findings may also help in decisions regarding diagnostic management (subsequent ultrasound examinations, non‐stress testing, biophysical profiles) and induction." (Source: ibid.)
A 2005 Norwegian study, Nakling et al. 2005, made a critically important point regarding ovulation variance which, when ovulation date is known via highly reliable (high sensitivity (i.e., low false positives) & high specificity (i.e., low false negatives)), home-use, digital, urinary ovulation tests and ovulation test systems to establish OTPD:
- to be included with all available evidence for consideration in the practice of evidence-based medicine to establish the beginning of pregnancy and GA while, simultaneously,
- preventing ovulation variance from being erroneously allocated into a grossly inaccurate NCFM eSnurra BPD-based EDD and GA thereby creating sub-optimal obstetric and fetal awareness and, consequently, sub-optimal obstetric and fetal management while, simultaneously,
- preventing constitutionally small, normal fetuses, SGA fetuses, fetal growth restrictions/malformations and other fetal pathology from being masked by inaccurate or grossly inaccurate NCFM eSnurra BPD-based EDD & GA.
- Abstract
Objective In a large unselected population of normal spontaneous pregnancies, to estimate the biologic variation of the interval from the first day of the last menstrual period to start of pregnancy, and the biologic variation of gestational length to delivery; and to estimate the random error of routine ultrasound assessment of gestational age in mid-second trimester.
Study design Cohort study of 11,238 singleton pregnancies, with spontaneous onset of labour and reliable last menstrual period. The day of delivery was predicted with two independent methods: According to the rule of Nägele and based on ultrasound examination in gestational weeks 17–19. For both methods, the mean difference between observed and predicted day of delivery was calculated. The variances of the differences were combined to estimate the variances of the two partitions of pregnancy.
Results The biologic variation of the time from last menstrual period to pregnancy start was estimated to 7.0 days (standard deviation), and the standard deviation of the time to spontaneous delivery was estimated to 12.4 days. The estimate of the standard deviation of the random error of ultrasound assessed foetal age was 5.2 days.
Conclusion Even when the last menstrual period is reliable, the biologic variation of the time from last menstrual period to the real start of pregnancy is substantial, and must be taken into account. Reliable information about the first day of the last menstrual period is not equivalent with reliable information about the start of pregnancy. (Source: "The biologic error in gestational length related to the use of the first day of last menstrual period as a proxy for the start of pregnancy" Jakob Nakling, Harald Buhaug, Bjorn Backe. Early Human Development (2005) 81, 833-839, p. 837) [Note: To avoid the paywall, this publication is include in Jacob Nakling's 2006 NTNU PhD Thesis beginning on PDF-page 44.]
- ABSTRACT
OBJECTIVE: Biological evidence suggests that both mother and fetus are involved in triggering a normal delivery. A tendency of a child to have a gestational age at birth similar to the father’s could represent the effect of genes passed from the father to the fetus. Similar tendencies between mother and child could represent maternal genes passed to the fetus, as well as genes to the mother received from the grandmother that affect a woman’s capacity to carry a pregnancy.
METHODS: The Medical Birth Registry of Norway contains data on all births in Norway from 1967 onward. We identified 77,452 pairs of boys and girls born at term who later became parents and linked their birth data to the birth records for their first child.
RESULTS: Gestational age of the child at birth increased on average 0.58 days for each additional week in the father’s gestational age (95% confidence interval 0.48–0.67) and 1.22 days for each additional week in the mother’s gestational age (1.21–1.32). Gestational age was, however, 0.65 days reduced for each additional kilogram in the father’s birth weight, presumably due to more rapid growth of the fetus triggering delivery.
CONCLUSION: Initiation of delivery has a fetal component that is heritable (passed from father and mother to child) and an additional maternal component that is also heritable. In addition, a more rapid rate of fetal growth appears to trigger delivery at earlier gestation.
A joint U.K and U.S. study, Bukowski et al. 2007, established "...the association between fetal growth in early pregnancy and the risk of delivering a small for gestational age infant."
- "First trimester growth
Our main finding was that the size of the fetus in the first trimester of pregnancy was associated with the birth weight. Approximately half of this association was due to the effect of first trimester size on the duration of pregnancy. The clinical significance of this finding is underlined by the association between fetal growth in early pregnancy and the risk of delivering a small for gestational age infant. Before the widespread use of ultrasound, fetal growth was thought to be largely genetically determined in early pregnancy and variation in fetal growth was thought to be primarily a feature of the second half of pregnancy.13 With the widespread clinical use of ultrasound, analysis of routinely collected data showed that fetuses that were smaller than expected in early pregnancy were at increased risk of adverse outcome, particularly poor growth. Intrauterine growth restriction was postulated to be evident in very early pregnancy.6 However, other authors suggested that a prolonged interval between menstruation and conception was the determining factor.7 Here we have shown that fetal growth in the first trimester of pregnancy is a major determinant of birth weight. Our study in pregnancies resulting from assisted reproductive technology has shown that the association between size in the first trimester and birth weight is not related to delayed ovulation but to first trimester growth.
The association between first trimester size and birth weight has now been shown in spontaneously conceived pregnancies6 and in pregnancies resulting from assisted reproductive technology, with precisely known time of conception. The same finding in two different populations would be unlikely to result from other factors than a common underlying mechanism. Pregnancies with appropriate fetal growth in the first trimester, of which the observed and expected sizes were equal (ΔGA =0), had smaller birth weight and a higher risk of small for gestational age infants than the general population. This is presumably the result of impaired fetal growth occurring after the first trimester in pregnancies resulting from assisted reproductive technology." (Source: "Fetal growth in early pregnancy and risk of delivering low birth weight infant: prospective cohort study" Radek Bukowski, Gordon C S Smith, Fergal D Malone, Robert H Ball, David A Nyberg, Christine H Comstock, Richard L Berkowitz, Susan J Gross, Lorraine Dugoff, Sabrina D Craigo, Ilan E Timor-Tritsch, Stephen R Carr, Honor M Wolfe, Mary E D'Alton. BMJ 2007; 334 doi: https://doi.org/10.1136/bmj.39129.637917.AE. Published 19 April 2007)
A 2008 Swedish study, Thorsell et al. 2008, conducted by the Karolinska Institutetat in Stockholm made the point that when ultrasound-based dating postponed EDD by 7 days or more there was "an increased risk for preterm delivery and pre-eclampsia." Laila's EDD was postponed by 15 days and 14 days relative to her factual LMPD-based EDD and her factual LMPD/OTPD/SCID-based EDD, respectively. Moreover, Laila suffered from postpartum pre-eclampsia. Additionally, and with respect to this study, Laila's first trimester ultrasound exam showed her baby's NCFM eSnurra CRL-based GA and BPD-based GA lagging her factual LMPD/OTPD/SCID-based GA by 9 days and 6 days, respectively. However, this evidence was also ignored. Included below is the abstract of Thorsell et al. 2008 or "Expected day of delivery from ultrasound dating versus last menstrual period--obstetric outcome when dates mismatch."
- Objective To analyse the association between fetal size at time of dating ultrasound and risk for preterm delivery and small-for-gestational-age (SGA) birth and to evaluate if timing of ultrasound, that is before 14 weeks of gestation or after 16 weeks affects this association.
Results When the expected date of delivery was postponed after ultrasound dating by 7 days or more, there was an increased risk for preterm delivery and pre-eclampsia in the late dating group (OR 1.49, 95% CI 1.27–1.73 and OR 1.27, 95% CI 1.02–1.60, respectively) but not in the early dating group. In both dating groups, there was an increased risk for SGA birth (OR 1.77, 95% CI 1.13–2.78 and OR 2.09, 95% CI 1.59–2.73, respectively) There was no increased risk for any of the other diagnoses.
Conclusion Our study gives further support to the notion that intrauterine growth restriction may be present as early as the first trimester. Accordingly, our study also suggests that surveillance of pregnancies with postponed estimated date of delivery may provide means for increased detection of fetal growth restriction. (Source: "Expected day of delivery from ultrasound dating versus last menstrual period--obstetric outcome when dates mismatch" Thorsell M, Kaijser M, Almström H, Andolf E. BJOG. 2008 Apr;115(5):585-9. doi: 10.1111/j.1471-0528.2008.01678.x.) - This "Discussion" section topic is interesting...
"In our study, we show that the increased risk for a SGA birth when expected date of delivery is postponed more than 1 week is independent of whether the dating ultrasound is performed in the first or second trimester. Thus, our study adds to the literature that fetal size in the first trimester is determined not only by gestational duration but may also be affected by poor fetal growth. However, reduced fetal size in the first trimester does not necessarily lead to growth restriction later in pregnancy. The fetus may be genetically small or experience catch-up growth. This could explain the reduced frequency of pregnancies that have their estimated date of delivery postponed in the late ultrasound compared with the early, 14.7 versus 23.5%." (Source: ibid.)
A 2008 Danish Study, Pedersen et al. 2008, found a BPD growth rate relationship in the beginning of pregnancy with adverse pregnancy outcome, implying a sub-optimal environment in early pregnancy limits fetal growth throughout pregnancy.
- "Discussion The central finding of our study was the significant relationship between BPD growth rate between the first and second trimesters and adverse pregnancy outcome. Low growth rates were associated with increased ORs for perinatal mortality and IUGR, and high growth rates were associated with increased ORs for macrosomia and preterm delivery. These findings underline the importance of focusing on early growth, potentially to prevent irreparable damage later in pregnancy. Traditional thinking is that early growth is principally controlled genetically and occurs at a constant exponential rate with little biological variation 14; IUGR has been assumed to occur mainly in the latter half of pregnancy. Our study refutes this, showing that fetal growth rate between the first and second trimesters does vary between fetuses and is associated with perinatal death and low birth weight. This implies that a suboptimal environment in the beginning of pregnancy limits fetal growth for the remainder of the pregnancy." (Source: "Fetal growth between the first and second trimesters and the risk of adverse pregnancy outcome" N. G. PEDERSEN, K. R. WØJDEMANN, T. SCHEIKE and A. TABOR. Ultrasound Obstet Gynecol 2008; 32: 147–154. DOI: 10.1002/uog.6109)
- Abstract
Objectives To relate growth rate of the biparietal diameter (BPD) between the first and second trimesters to the risk of perinatal death, intrauterine growth restriction (IUGR), macrosomia, preterm/post-term delivery and pre-eclampsia.
Methods In this retrospective study, we analyzed sono-graphic BPD measurements at 11–14 and 17–21 weeks from 8215 singleton pregnancies in the Copenhagen First Trimester Study. Growth rate was defined as millimeters of growth per day between the two measurements and was dichotomized into growth rates < 2.5th vs. 2.5th–97.5th centiles, and > 97.5th vs. 2.5th–97.5th centiles. Odds ratios (OR) and 95% CIs for adverse outcome were calculated.
Results Fetuses with growth rates < 2.5th centile had an OR of 4.79 (95% CI, 1.43–15.99) for perinatal death and an OR of 2.64 (95% CI, 1.51–4.62) for birth weight< sonographically estimated mean fetal weight (adjusted for gestational age) − 2 SD. Fetuses with growth rates > 97.5th centile had an OR of 2.83 (95% CI, 1.58–5.06)for birth weight > mean + 2 SD and an OR of 2.30 (95%CI, 1.15–4.59) for delivery in weeks 34–36. Growth rate showed no association with pre-eclampsia.
Conclusions There is a significant relationship between the growth rate of BPD from the first to the second trimester and adverse pregnancy outcome. Low growth rates are associated with an increased OR for perinatal death and IUGR, while high growth rates are associated with an increased OR for macrosomia and preterm delivery.
A 2008 Norwegian study, Johnsen et al. 2008, assessed the effect of second trimester fetal size on the duration of pregnancy and the influence of ultrasound dating. This study used the more robust head circumference (HC) instead of the problematic, unreliable BPD metric for fetal head measurements and GA estimations. The results of Johnsen et al. 2008 "support a concept of individually assigned pregnancy duration according to growth rates rather than imposing a standard of 280–282 days on all pregnancies." This concept has been supported by subsequent studies, including the U.S. study, Jukic et al. 2013, conducted by The National Institute of Environmental Health Sciences (NIEHS) of the U.S. National Institutes of Health (NIH).
- "We hypothesize that, in addition to LMP, fetal growth (reflected in fetal size) might be such a determining factor for pregnancy duration. The aim of the present study was therefore to assess the effect of second trimester fetal size on the duration of pregnancy and the influence of ultrasound dating." (Source: "Fetal size in the second trimester is associated with the duration of pregnancy, small fetuses having longer pregnancies" Synnøve L Johnsen, Tom Wilsgaard, Svein Rasmussen, Mark A Hanson, Keith M Godfrey and Torvid Kiserud. BMC Pregnancy and Childbirth 2008, 8:25 doi:10.1186/1471-2393-8-25. Received: 22 November 2007, Accepted: 16 July 2008, Published: 16 July 2008)
- Abstract
Background: Conventionally, the pregnancy duration is accepted to be 280–282 days. Fetuses determined by ultrasound biometry to be small in early pregnancy, have an increased risk of premature birth. We speculate that the higher rate of preterm delivery in such small fetuses represents a pathological outcome not applicable to physiological pregnancies. Here we test the hypothesis that in low-risk pregnancies fetal growth (expressed by fetal size in the second trimester) is itself a determinant for pregnancy duration with the slower growing fetuses having a longer pregnancy.
Methods: We analysed duration of gestation data for 541 women who had a spontaneous delivery having previously been recruited to a cross-sectional study of 650 low-risk pregnancies. All had a regular menses and a known date of their last menstrual period (LMP). Subjects were examined using ultrasound to determine fetal head circumference (HC), abdominal circumference (AC) and femur length (FL) at 10–24 weeks of gestation. Length of the pregnancy was calculated from LMP, and birth weights were noted. The effect of fetal size at 10–24 weeks of gestation on pregnancy duration was assessed also when adjusting for the difference between LMP and ultrasound based fetal age.
Results: Small fetuses (z-score -2.5) at second trimester ultrasound scan had lower birth weights (p < 0.0001) and longer duration of pregnancy (p < 0.0001) than large fetuses (z-score +2.5): 289.6 days (95%CI 288.0 to 291.1) vs. 276.1 (95%CI 273.6 to 278.4) for HC, 289.0 days (95%CI 287.4 to 290.6) vs. 276.9 days (95%CI 274.4 to 279.2) for AC and 288.3 vs. 277.9 days (95%CI 275.6 to 280.1) for FL. Controlling for the difference between LMP and ultrasound dating (using HC measurement), the effect of fetal size on pregnancy length was reduced to half but was still present for AC and FL (comparing z-score -2.5 with +2.5, 286.6 vs. 280.2 days, p = 0.004, and 286.0 vs. 280.9, p = 0.008, respectively).
Conclusion: Fetal size in the second trimester is a determinant of birth weight and pregnancy duration, small fetuses having lower birth weights and longer pregnancies (up to 13 days compared with large fetuses). Our results support a concept of individually assigned pregnancy duration according to growth rates rather than imposing a standard of 280–282 days on all pregnancies. (p. 1) - Discussion
"In contrast to the mentioned studies, the present study was based on a healthy population of low-risk women who spontaneously went into labour and the overall obstetric outcome was good, with a low incidence of low birth weight and premature births (Table 1). Thus,smaller fetuses in the present study can be regarded to be within normal biological variation, not growth restricted, and interestingly they had longer, not shorter duration of pregnancies." (p. 5)
"Our results are supported by a recent study of the heritable component of duration of pregnancy [19]. In that study, the father and mother's own gestational age at birth were associated with the offspring's gestational age, and fathers with higher birth weights had larger offspring with shorter gestational length, which is in line with our results. The results of all the studies mentioned above fit with a U-shaped relationship between fetal growth and duration of pregnancy; rapidly growing fetuses tend to have shorter duration, slower growing fetuses a longer duration of pregnancy while pathologically slow growth have increased rates of birth before 37 weeks of gestation." (p. 5)
"The present results suggest that within physiological ranges fetal growth may be slower and then associated with an extended pregnancy, a phenomenon that is also known from animal studies [27]. Nutritionally restricted pregnancies resulted in slower growth and longer pregnancies." (p. 6) - Discussion Conclusion To accommodate biological variation in fetal growth, customized [29] and conditional [30] models have been developed to individualize growth assessment. We believe that by accepting a greater biological variation of pregnancy duration than is imposed by the current ultrasound dating method, our clinical assessments may be founded on sounder biological principles. (p. 6)
A 2010 Swedish study, Skalkidou et al. 2010, based on data from the Swedish Medical Birth Registry (SMBR) concluded there was an increased risk of adverse perinatal outcomes for baby girls (i.e., smaller) relative to baby boys after ultrasound was introduced for estimation of GA. The complete abstract of Skalkidou et al. 2010 or "Ultrasound pregnancy dating leads to biased perinatal morbidity and neonatal mortality among post-term-born girls" is included below.
- ABSTRACT
BACKGROUND: Ultrasound assessment of gestational length is based on the assumption that fetuses of the same gestational age have equal size at the time of investigation. However, there are detectable sex differences in fetal size by the end of the first trimester. We examined whether ultrasound dating introduces sex differences in risks of adverse perinatal outcomes related to post-term birth.
METHODS: We used the Swedish Medical Birth Register to compare male and female newborns during 1973-1978, when gestational age was based on the last menstrual period, and 1995-2007, when gestational age was based on ultrasound. We included singleton births from 39 to 43 gestational weeks.
RESULTS: During the first time period, the newborn male-to-female ratio by gestational age at delivery was constant around 1.0, but in the later time period it consistently increased by gestational age, reaching 1.60 at 43 weeks. In the first time period, post-term females had reduced risk for adverse perinatal outcomes compared with post-term males. After the introduction of ultrasound, post-term females had higher risks of stillbirth (odds ratio = 1.60 [95% confidence interval = 1.11 to 2.30]) and meconium aspiration (1.39 [1.10 to 1.75]), compared with post-term males. One-third of stillbirths among post-term girls today might be due to incorrect calculation of gestational age.
CONCLUSIONS: Introduction of ultrasound for the estimation of gestational age may be associated with increased risks of adverse perinatal outcomes among females classified as post-term compared with their male counterparts. (Source: "Ultrasound pregnancy dating leads to biased perinatal morbidity and neonatal mortality among post-term-born girls" Skalkidou A1, Kieler H, Stephansson O, Roos N, Cnattingius S, Haglund B. Epidemiology. 2010 Nov;21(6):791-6. doi: 10.1097/EDE.0b013e3181f3a660)
A 2014 Australian study, Carberry et al. 2014, is a Cochrane Review study of The Cochrane Pregnancy and Childbirth Group’s Trials Register. And, while authors' concluded no randomized trials met the inclusion criteria, authors provide highly relevant background information for fetal growth restriction (FGR), small for gestational age (SGA) and and the importance of detecting SGA, especially within low-risk populations.
- "Authors' conclusions
There is no randomised trial evidence currently available. Further randomised trials are required to accurately assess whether the improvement in detection shown is secondary to customised charts alone or an effect of the policy change. Future research in large trials is needed to investigate the benefits and harms (including perinatal mortality) of using customised growth charts in different settings and for both fundal height and ultrasound measurements" - "Background
Fetal growth restriction is defined as failure to reach growth potential and is considered one of the major complications of pregnancy. Impaired fetal growth may be due to maternal complications such as pregnancy-associated hypertension, fetal complications (including structural or chromosomal problems) or problems with placental development (which is the most common cause of impaired growth) (Grivell 2009). These infants are often, although not universally, small for gestational age (SGA). SGA is defined as a weight less than a specified percentile (usually the 10th percentile). However, it is important to note that a proportion of infants defined as SGA will actually be normally grown (constitutionally small) and another proportion truly growth restricted (pathologically small). Furthermore, some infants who have not reached their growth potential will not be less than the 10th percentile and therefore not classified as SGA (Gelbaya 2005).
Identification of SGA infants is important because these infants are at an increased risk for perinatal morbidity and mortality, associated health problems (such as neurodevelopment and intellectual consequences), persistent short stature, as well as long-term adverse consequences such as adult onset cardiovascular disease and metabolic alternations in later life (Barker 2004; Clayton 2007; Maulik 2006).
Screening for SGA is a challenge for all maternity care providers, particularly in low-risk pregnancies, and current methods of clinical assessment fail to detect many infants who are SGA (Wright 2006). Previous research has shown that, using standard methods of antenatal care, only 16% (Kean 1996) of SGA infants were detected and 26% (Hepburn 1986) of SGA infants were suspected to be small prior to birth. The majority of maternity services measure symphysiofundal height (SFH) and use a rule that normal growth should be within two weeks of gestational age. In low-risk populations, SFH as a screening tool for assessment of SGA has a low detection rate in women with a normal BMI (body mass index) (Kean 1996). Furthermore, SFH measurement has an even lower sensitivity in screening for SGA in women with an increased body mass (Jelks 2007; Stuart 1989). A Cochrane review on using SFH measurement in pregnancy for detecting abnormal fetal growth is currently being prepared (Japaraj 2009)."
(Source: "Customised versus population-based growth charts as a screening tool for detecting small for gestational age infants in low-risk pregnant women" Angela E Carberry, Adrienne Gordon, Diana M Bond, Jon Hyett, Camille H Raynes-Greenow, Heather E Jeffery. Cochrane Database of Systematic Reviews, 2014 Issue 5. http://dx.doi.org/10.1002/14651858)
A 2014 Norwegian study, Morken et al. 2014, conducted a retrospective analysis of data for 1,855,682 pregnancies in Norway from the Medical Birth Registry of Norway (MBRN). Morken et al. presented disturbing but not an unexpected results or unexpected conclusion which directly relates to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine (i.e., "TUL" policy and protocol). It is important to note all ultrasound-based estimations of GA in study periods 1987–2006 and 1999-2006 were conducted using the Campbell Method of Gestational Age Estimation (Campbell 1969) via NCFM Snurra BPD-based GA, as stated on page 2 and via citation 23 of Morken et al. 2014. Moreover, authors identified an important clinical implication which directly addresses, if not defines, the single most important clinical issue within LailasCase.com:
- "However, one of the most important clinical implications of our study is that these growth restricted infants should probably not have their gestational age determined solely by ultrasound." (Source: "Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study" Nils-Halvdan Morken, Kari Klungsøyr and Rolv Skjaerven. BMC Pregnancy and Childbirth 2014 14:172. https://doi.org/10.1186/1471-2393-14-172. Received: 20 January 2014, Accepted: 7 May 2014, Published: 22 May 2014) [Note: Also, check out: Medical Birth Registry of Norway (MBRN)]
- Morken et al. 2014 identify evidence of the risks and consequences inherent in government-mandated, unilateral reliance on ultrasound-based estimation (or calculation) of gestational age with the active exclusion of all other evidence of known, proven efficacy; evidence of the risks and consequences of which NGF, Bergen Group and others had explicitly warned Directorate of Health; warnings which were ignored. Morken et al. 2014 was conducted by a team of 3 Bergen-based medical science researchers:
- Nils-Halvdan Morken, MD, PhD, Department of Global Public Health and Primary Care, University of Bergen; Department of Clinical Sciences, University of Bergen; Department of Obstetrics and Gynecology, Haukeland University Hospital, Bergen
- Kari Klungsøyr, MD, PhD, Department of Global Public Health and Primary Care, University of Bergen; Medical Birth Registry of Norway, Norwegian Institute of Public Health, Bergen
- Rolv Skjaerven, PhD, Department of Global Public Health and Primary Care, University of Bergen; Medical Birth Registry of Norway, Norwegian Institute of Public Health, Bergen
- This seminal Norwegian study was published by BMC Pregnancy and Childbirth as "Perinatal mortality by gestational week and size at birth in singleton pregnancies at and beyond term: a nationwide population-based cohort study." The Abstract, followed by select, relevant excerpts (emphasis added) are included below.
- Abstract
Background: Whether gestational age per se increases perinatal mortality in post-term pregnancy is unclear. We aimed at assessing gestational week specific perinatal mortality in small-for-gestational-age (SGA) and non-SGA term and post-term gestations, and specifically to evaluate whether the relation between post-term gestation and perinatal mortality differed before and after ultrasound was introduced as the standard method of gestational age estimation.
Methods: A population-based cohort study, using data from the Medical Birth Registry of Norway (MBRN), 1967–2006, was designed. Singleton births at 37 through 44 gestational weeks (n = 1 855 682), excluding preeclampsia, diabetes and fetal anomalies, were included. Odds ratios (OR) with 95% confidence intervals (CI) for perinatal mortality and stillbirth in SGA and non-SGA births by gestational week were calculated.
Results: SGA infants judged post-term by LMP had significantly higher perinatal mortality than post-term non-SGA infants at 40 weeks, independent of time period (highest during 1999–2006 [OR 9.8, 95% CI: 5.7-17.0]). When comparing years before (1967–1986) versus after (1987–2006) ultrasound was introduced, there was no decrease in the excess mortality for post-term SGA versus non-SGA births (ORs from 6.1 [95% CI: 5.2-7.1] to 6.7 [5.2-8.5]), while mortality at 40 weeks decreased significantly (ORs from 4.6, [4.0-5.3] to 3.2 [2.5-3.9]). When assessing stillbirth risk (1999–2006), more than 40% of SGA stillbirths (11/26) judged to be ≥41 weeks by LMP were shifted to lower gestational ages using ultrasound estimation.
Conclusions: Mortality risk in post-term infants was strongly associated with growth restriction. Such infants may erroneously be judged younger than they are when using ultrasound estimation, so that the routine assessment for fetal wellbeing in the prolonged gestation may be given too late. - Included below are select, relevant excerpts from Morken et al. 2014.
"We hypothesized that death risk in post-term pregnancies is strongly associated with being small-for-gestational age (SGA) and that the implementation of ultrasound-based estimates of gestational age may have had a negative impact especially for the growth restricted infants being assessed as post-term later than they should. The main purpose of the current study was to assess the risk of perinatal death in SGA and non-SGA term and post-term gestations by gestational week, and specifically to evaluate whether the relation between post-term gestation and perinatal mortality was different in the time period before and after ultrasound was introduced as the standard method of gestational age estimation."
"Ultrasound gestational age estimation may reduce the total burden of post-term delivery by shifting the entire distribution towards younger gestational ages, but the prize [sic] seems to be paid by the small, misclassified fetus."
"Our study thus suggests a possible negative impact of changing gestational age estimation method on the relation between post term gestation and mortality risk. The acknowledged shift [16] in gestational age distribution towards younger gestations when using ultrasound measurements at 18 weeks is mostly a problem for growth restricted infants, some of which may be growth restricted also at this early age [18]. These fetuses will mistakenly be judged as younger than they are, and the pregnancies will thus be set up for post-term evaluation too late. At the same time, these growth restricted infants are the exact infants with the highest mortality risk in the post term period."
"However, we also show an interaction between SGA status and post-term gestation in LMP dated pregnancies with significantly higher excess mortality for SGA than non-SGA post-term infants. This suggests that the perinatal mortality risk in the post-term pregnancy is mostly linked to growth restriction rather than to the prolonged gestational age per se."
"We also found a significantly increased risk of perinatal death in non-SGA post-term infants when gestational age was based on menstrual dates, whereas mortality was not significantly increased when post-term gestation was based on ultrasound."
"Our data emphasize the importance of identifying the growth-restricted infants in the prolonged and post-term phase of pregnancy due to their increased perinatal mortality risk. However, one of the most important clinical implications of our study is that these growth restricted infants should probably not have their gestational age determined solely by ultrasound." - "Conclusions: Perinatal death risk in prolonged and post-term pregnancies was strongly associated with SGA, independent of time period and method of gestational age estimation. However, the excess mortality risk seen for SGA infants judged to be post-term by LMP has increased after ultrasound estimation has become routine, when compared to non-SGA infants at 40 weeks. This indicates that pregnancies with growth restricted infants may be judged younger than they are when gestational age is estimated by ultrasound. This was further supported by finding that more than 40% of SGA stillbirths judged to be ≥41 weeks by LMP were shifted to lower gestational ages when using ultrasound estimation. Routine assessment of fetal wellbeing in the prolonged and post-term gestations will be missed in these pregnancies."
A 2016 Swedish study, Kullinger et al. 2016, used data from 1,314,602 births via the Swedish Medical Birth Register (SMBR), which contains data for 99% of all births in Sweden since 1973, to compare adverse outcomes related to prematurity between male and female babies for ultrasound and LMP pregnancy dating methods. The Results and Conclusion sections from the abstract of Kullinger et al. 2016 or "Effects of ultrasound pregnancy dating on neonatal morbidity in late preterm and early term male infants: a register-based cohort study" are included below.
- Results: As expected, adverse outcomes were lower in the later time period, but the reduction in prematurity-related morbidity was less marked for male than for female infants. After changing the pregnancy dating method, male infants born early term had, in relation to female infants, higher odds for pneumothorax (Cohort ratio [CR] 2.05; 95 % confidence interval [CI] 1.33–3.16), respiratory distress syndrome of the newborn (CR 1.99; 95 % CI 1.33–2.98), low Apgar score (CR 1.26; 5 % CI 1.08–1.47), and hyperbilirubinemia (CR 1.12; 95 % CI 1.06–1.19), when outcome was compared between the two time periods. A similar trend was seen for late preterm male infants.
Conclusion: Misclassification of gestational age by ultrasound, due to size differences, can partially explain currently reported sex differences in early term and late preterm infants’ adverse neonatal outcomes, and should be taken into account in clinical decisions and when interpreting study results related to fetal sex. (Source: "Effects of ultrasound pregnancy dating on neonatal morbidity in late preterm and early term male infants: a register-based cohort study" Merit Kullinger, Bengt Haglund, Helle Kieler and Alkistis Skalkidou. BMC Pregnancy Childbirth. 2016; 16: 335. Published online 2016 Oct 31. doi: 10.1186/s12884-016-1129-z)
A 2016 international study, Morken 2016, of singleton live births in the Medical Birth Registries of Norway, Sweden and Finland and US live birth certificates demonstrated "that discrepancy between methods to estimate gestational age may be a predictor for infant mortality and other adverse pregnancy outcomes in all four study countries."
- Abstract
Background Gestational age estimation by last menstrual period (LMP) vs. ultrasound (or best obstetric estimate in the US) may result in discrepant classification of preterm vs. term birth. We investigated whether such discrepancies are associated with adverse infant outcomes.
Methods We studied singleton livebirths in the Medical Birth Registries of Norway, Sweden and Finland and US live birth certificates from 1999 to the most recent year available. Risk ratios (RR) with 95% confidence intervals (CI) by discordant and concordant gestational age estimation for infant, neonatal and post-neonatal mortality, Apgar score <4 and <7 at 5 min, and neonatal intensive care unit (NICU) admission were estimated using generalised linear models, adjusting for maternal age, education, parity, year of birth, and infant sex. Results were presented stratified by country.
Results Compared to infants born at term by both methods, infants born preterm by ultrasound/best obstetric estimate but term by LMP had higher infant mortality risks (range of adjusted RRs 3.9 to 7.2) and modestly higher risks were obtained among infants born preterm by LMP but term by ultrasound/best obstetric estimate (range of adjusted RRs 1.6 to 1.9). Risk estimates for the other outcomes showed the same pattern. These findings were consistent across all four countries.
Conclusions Infants classified as preterm by ultrasound/best estimate, but term by LMP have consistently higher risks of adverse outcomes than those classified as preterm by LMP but term by ultrasound/best estimate. Compared with ultrasound/best estimate, use of LMP overestimates the proportion of births that are preterm. (Source: "Adverse Infant Outcomes Associated with Discordant Gestational Age Estimates" Nils‐Halvdan Morken, Rolv Skjærven, Jennifer L. Richards, Michael R. Kramer, Sven Cnattingius, Stefan Johansson, Mika Gissler, Siobhan M. Dolan, Jennifer Zeitlin, Michael S. Kramer for the PREBIC Epidemiology Working Group, Paediatric and Perinatal Epidemiology, 2016 November; 30(6): 541–549.. First published: 23 August 2016 https://doi.org/10.1111/ppe.12311) - Comment
"This analysis of data from Norway, Sweden, Finland, and the United States demonstrates that both groups with discordant gestational age estimates had consistently higher risks of adverse perinatal outcomes than those classified as term by both methods. These results show that discrepancy between methods to estimate gestational age may be a predictor for infant mortality and other adverse pregnancy outcomes in all four study countries." (Source: ibid.)
"A valid assessment of gestational age is essential in clinical management, clinical trials, epidemiologic studies, and vital statistics. Our multicountry study highlights that discrepant estimates in gestational age assessment are associated with adverse infant outcomes across all four study countries. It seems reasonable to conclude that using the ultrasound/best obstetric estimate to define preterm will yield infants with higher risks of poor outcomes (whether or not they are truly preterm)." (Source: ibid.)
A 2016 Norwegian study, Bohlin et al. 2016, stated that "more accurate methods for estimating GA...would be of great benefit in clinical practice." The NCFM eSNurra "method" per citation/reference [1] (below) estimates EDD, not GA. The NCFM eSnurra "method" must calculate GA from an estimate of EDD using the equivalent of Naegele's rule, but in reverse. The NCFM eSnurra "method" neither estimates nor uses gestational age (GA) to assess due dates (EDD). Moreover, NCFM's eSnurra EDD estimation "method" is an appropriated, plagiarized, misused implementation of Dr. David J. R. Hutchon's original idea and method of Population-based Direct EDD Estimation (PDEE) published in 1998 (Hutchon 1998).
- "Background
Determination of gestational age (GA) is important for assessing due dates, giving adequate prenatal care, and suggesting appropriate interventions in preterm and post-term pregnancies. In Norway it is common clinical practice to assign pregnant women a due date based on the date of the last menstrual period (LMP). Around pregnancy week 18 a routine ultrasound examination, attended by almost all pregnant women, is used to calculate more precise estimates of GA and due date [1]. Although ultrasound-based estimates of GA are more precise in predicting the birth date than estimates based on the last menstrual period, LMP-based estimates may be preferred in some circumstances [2, 3]. There is wide variability in estimated GA even when ultrasound is used [4]. Ultrasound GA predictions eliminate uncertainties such as inaccurate reporting of the date of LMP and variability in the follicular phase length, although they assume uniform fetal growth during early pregnancy, which is only approximately true [5]. Hence, there is room for more accurate methods for estimating GA, which would be of great benefit in clinical practice." (Source: "Prediction of gestational age based on genome-wide differentially methylated regions" J. Bohlin, S. E. Håberg, P. Magnus, S. E. Reese, H. K. Gjessing, M. C. Magnus, C. L. Parr, C. M. Page, S. J. London and W. Nystad. Genome Biology 2016 17:207 https://doi.org/10.1186/s13059-016-1063-4. Received: 11 April, 2016 Accepted: 14 September 2016, Published: 7 October 2016) [Note: Citation/Reference 1 is Gjessing et al. 2007; Citation/Reference 5 is Bukowski et al. 2007.]
A 2017 Swedish study, Kullinger et al. 2017, looked at discrepancies between EDD-LMP and EDD-US gestational age. The Key Message: "Variance in early fetal growth can bias ultrasound-based pregnancy dating. Maternal obesity, height, and fetal sex may partly explain large discrepancies between pregnancy-dating methods."
- "Abstract
Introduction Gestational age is estimated by ultrasound using fetal size as a proxy for age, although variance in early growth affects reliability. The aim of this study was to identify characteristics associated with discrepancies between last menstrual period‐based (EDD‐LMP) and ultrasound‐based (EDD‐US) estimated delivery dates.
Material and methods We identified all singleton births (n = 1 201 679) recorded in the Swedish Medical Birth Register in 1995–2010, to assess the association between maternal/fetal characteristics and large negative and large positive discrepancies (EDD‐LMP earlier than EDD‐US and 10th percentile in the discrepancy distribution vs. EDD‐LMP later than EDD‐US and 90th percentile). Analyses were adjusted for age, parity, height, body mass index, smoking, and employment status.
Results Women with a body mass index >40 kg/m2 had the highest odds for large negative discrepancies (−9 to −20 days) [odds ratio (OR) 2.16, 95% CI 2.01–2.33]. Other factors associated with large negative discrepancies were: diabetes, young maternal age, multiparity, body mass index between 30 and 39.9 kg/m2 or <18.5 kg/m2, a history of gestational diabetes, female fetus, shorter stature (<−1 SD), a history of preeclampsia, smoking or snuff use, and unemployment. Large positive discrepancies (+4 to +20 days) were associated with male fetus (OR 1.80, 95% CI 1.77–1.83), age ≥30 years, multiparity, not living with a partner, taller stature (>+1 SD), and unemployment.
Conclusions Several maternal and fetal characteristics were associated with discrepancies between dating methods. Systematic associations of discrepancies with maternal height, fetal sex, and partly obesity, may reflect an influence on the precision of the ultrasound estimate due to variance in early growth. - Discussion Increased awareness of maternal and fetal characteristics that can bias GA estimates can be helpful in clinical situations when large discrepancies between methods are noted. A large discrepancy combined with characteristics affecting early growth should lead to critical evaluation of the GA estimate based on US, and additional information, such as the date of the LMP or an assumed date of conception, should be considered before decision-making. As large negative discrepancies are associated with adverse outcomes, these pregnancies may benefit from closer monitoring in order to detect intrauterine growth retardation and to avoid post-term pregnancies (14,33)." (Source: "Maternal and fetal characteristics affect discrepancies between pregnancy‐dating methods: a population‐based cross‐sectional register study" Merit Kullinger, Jan Wesström, Helle Kieler, Alkistis Skalkidou. Acta Obstetricia et Gynecologica Scandinavica Volume 96, Issue 1, January 2017, Pages 86-95First published: 3 October 2016 https://doi.org/10.1111/aogs.13034)
A Swedish Commentary, Skalkidou et al. 2018, looked at the effects and clinical implications of misclassification of gestational age by ultrasound-based pregnancy dating in the the Nordic countries. The Key Message: "Misclassification of gestational age by ultrasound biometry in the second trimester may influence the numbers and the magnitude of adverse perinatal outcomes, closely related to gestational age, which are recorded in the Nordic birth registers. Continued reporting of last menstrual period in the registries is advocated."
- "Abstract
Historically, pregnancy dating has been based on self-reported information on the first day of the last menstrual period. In the 1970s, ultrasound biometry was introduced as an alternative for pregnancy dating and is now the leading method in Nordic countries. The use of ultrasound led to a reduction of post-term births and fewer inductions, and is considered more precise than last menstrual period-based methods for pregnancy dating. Nevertheless, differences in early growth and specific situations, such as maternal obesity, can render its estimates less precise, leading to gestational age misclassification. Clinical implications of ultrasound dating include effect on timely induction in case of post-term pregnancies, treatment with corticosteroids in cases of anticipated preterm delivery and decision on viability in cases of extreme prematurity. Furthermore, gestational age misclassification may influence the numbers and the magnitude of some adverse perinatal outcomes, closely related to gestational age, which are recorded in the Nordic birth registers." - Effects of Ultrasound Used for Pregnancy Dating
"More importantly, discrepancies between dating methods are associated with adverse perinatal outcomes (20– 22). For example, when a fetus is smaller than expected at the time of the ultrasound examination, the estimated gestational age will be less that [sic] the real gestational age, and the EDD will be postponed. Thus, when the ultrasound-based EDD arrives, the fetus will actually be more mature than 40 completed weeks. Size differences related to fetal sex have been estimated to affect relative risk estimates of pre- and post-term birth of female compared with male fetuses by 10–20% (23) simply because fetal sex is associated with fetal size, which in turn is used to determine gestational age. Discrepancies of more than seven days between the estimates have been associated with increased risk for stillbirth, neonatal death, low Apgar score at 5 min, low birthweight and preterm birth (21)." - Implications for Clinical Practice
"Given the wide adoption of ultrasound-based pregnancy dating within current obstetric practice in the Nordic countries, both beneficial and adverse effects of the method are expected to impact on clinical decisions and on perinatal outcomes. In cases of early growth restriction, gestational age may be underestimated, leading to misclassification of size at birth (24). Data from the Iowa Health in Pregnancy Study indicate an underestimation of small-for-gestational-age (SGA) births by 13% when ultrasound-based pregnancy dating is used (25). An underestimation of gestational age could also lead to a delay in induction of pregnancies that have entered the post-term period, which could adversely affect perinatal and neonatal mortality (21,26). Misclassification of gestational age is expected to be more pronounced when ultrasound dating is performed in the second trimester, at which time fetal growth differences are even greater than in the first trimester."
(Source: "Systematic misclassification of gestational age by ultrasound biometry: implications for clinical practice and research methodology in the Nordic countries" ALKISTIS SKALKIDOU, MERIT KULLINGER, MARIOS K. GEORGAKIS , HELLE KIELER & ULRIK S. KESMODEL. Acta Obstetricia et Gynecologica Scandinavica 97 (2018) 440–444. SPECIAL THEMED ISSUE: Methodology in Clinical Epidemiological Research in Obstetrics and Gynecology, April 2018. DOI: 10.1111/aogs.13300. Received: 18 December 2017 Accepted: 12 January 2018)
A 2018 "Expert Review" titled "The World Health Organization fetal growth charts: concept, findings, interpretation, and application" states:
- "The wide physiologic ranges, as illustrated by the 5th–95th percentile for estimated fetal weight being 2205–3538 g at 37 weeks gestation, signify that human fetal growth under optimized maternal conditions is not uniform. Rather, it has a remarkable variation that largely is unexplained by commonly known factors. We suggest this variation could be part of our common biologic strategy that makes human evolution extremely successful. The World Health Organization fetal growth charts are intended to be used internationally based on low-risk pregnancies from populations in Africa, Asia, Europe, and South America. We consider it prudent to test and monitor whether the growth charts’ performance meets the local needs, because refinements are possible by a change in cut-offs or customization for fetal sex, maternal factors, and populations. In the same line, the study finding of variations emphasizes the need for carefully adjusted growth charts that reflect optimal local growth when public health issues are addressed." (Source: "The World Health Organization fetal growth charts: concept, findings, interpretation, and application" Torvid Kiserud, MD, PhD; Alexandra Benachi, MD, PhD; Kurt Hecher, MD; Rogelio González Perez MD; José Carvalho, PhD; Gilda Piaggio, PhD; Lawrence D. Platt, MD. American Journal of Obstetrics and Gynecology Volume 218, Issue 2, Supplement, February 2018, Pages S619-S629. https://doi.org/10.1016/j.ajog.2017.12.010f. Received 8 November 2017, Revised 5 December 2017, Accepted 6 December 2017, Available online 6 February 2018.)
Epidemiological Studies: Adverse Outcomes Associated with Discrepancies Between LMP-GA & US-GA
The common theme among the studies included among the epidemiological studies is that large discrepancies between LMP-GA/EDD and Ultrasound-GA/EDD are associated with misclassification of gestational age and adverse outcomes which include perinatal and neonatal mortality. Laila's case proved that using Ultrasound-based EDD, unilaterally, and, therefrom, a calculating GA using the equivalent of Naegele's rule, in reverse, causes increased medical risks, critical medical mistakes and grievous medical harms. perinatal and neonatal mortality
Evidence-obviated Medicine: Unilateral NCFM eSnurra BPD-based EDD (or 'TUL' policy), No Matter What!
Ironically, one of the better descriptions of the problem in the literature is that which was included in NCFM Snurra Group's Tunón et al. 1999a (first excerpt below).
- "The ultrasound method regards all fetuses with the same BPD as being the same age. Early impairment of fetal growth might therefore influence the accuracy of the method. Impairment of fetal growth early in pregnancy may be caused by chromosomal aberrations, fetal malformations or infections, or it may be an isolated feature. Growth-restricted fetuses will have a smaller BPD than expected, not because they are younger but because they are growth-restricted. A consequence of this early growth restriction might be to change the day of delivery as estimated by ultrasound, to a later date than the day of delivery that is determined in accordance with the LMP. Such an extension of the estimated day of delivery might therefore lead to a falsely lower gestational age and a later detection or no detection at all of the growth restriction, with the possible consequence of adverse obstetric management of the pregnancy." (Source: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" Tunon K, Eik-Nes SH, Grøttum P. Ultrasound Obstet Gynecol 1999; 14: 17–22., p. 17)
- And, to be clear with respect to the excerpt above, "the possible consequence of adverse obstetric management of the pregnancy" is perinatal death. Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" (i.e., the plagiarized, intentionally misused Hutchon Method of PDEE) with a government-mandated protocol of evidence-obviated medicine is proven to cause increased medical risks, critical medical mistakes and grievous medical harms to some of Norway's women and their fetuses/babies; increased risks, critical mistakes & grievous harms which include unnecessary adverse events = perinatal deaths = dead babies.
NCFM Snurra Group obviated the evidence that was the relative risk of 2.07 for perinatal death from the Results and Conclusion sections of NCFM Snurra Group's Tunón et al. 1999a. It is interesting to note that the NCFM Snurra Group had the government contract/concession to provide ultrasound estimations of GA and, therefrom, calculations of EDD for all pregnancies in Norway while, at the same time, NCFM Snurra Group were the one and only research group to falsely conclude: - Abstract: "Conclusion There was no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population."
- Discussion Section Conclusion "In conclusion, there is no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population. However, further studies are required to explore this phenomenon."
- However, NCFM Snurra Group obviated their own evidence (i.e., a relative risk of 2.07 for perinatal death) from their conclusion in order to establish themselves as the one and only research group to have concluded: "there is no indication of any adverse consequence of the routine scan and change of estimated day of delivery among 15 000 pregnancies in a non-selected population." This was, of course, a falsified conclusion, evidenced by Tables 2 & 3 of Tunón et al. 1999a.
Evidence Supports Implementation of the Precautionary Principle
The epidemiological evidence (above, sans NCFM Snurra Group's red herring that is Tunón et al. 1999a) is both voluminous and clear, but especially the Norwegian study, Morken et al. 2014. One would think the risks and consequences identified by a plethora of international clinical and epidemiological evidence would be enough to implement the Precautionary Principle. The data and evidence assembled and presented in the Norwegian Studies are compelling, beginning with Johan Bergh's 1992 article, Bergh 1992, published in Tidsskrift for den Norske lægeforening, followed by Nakling & Backe 2002 in Acta Obstetricia et Gynecologica Scandinavica (AOGS), Nakling et al. 2005 in Early Human Development, Johnsen et al. 2008 in BMC Pregnancy and Childbirth and concluding with Morken et al. 2014, published in BMC Pregnancy and Childbirth. The published evidence makes it clear that SGA and growth restricted/malformed fetuses are at increased risk of perinatal death when estimated date of delivery is changed from the date of delivery determined by the LMPD or OTPD or SCID or LMPD/OTPD/SCID or other corroborating combinations thereof, to a later date of delivery as estimated, unilaterally, by ultrasound. The effect of which is to establish erroneous EDD & GA for individual pregnancies which create sub-optimal obstetric and fetal awareness which cause sub-optimal obstetric and fetal management, which causes increased medical risks, critical medical mistakes and grievous medical harms; grievous medical harms which include perinatal mortality.
The Constitution of the Kingdom of Norway
- Chapter E: Human Rights
Article 104
Children have the right to respect for their human dignity. They have the right to be heard in questions that concern them, and due weight shall be attached to their views in accordance with their age and development.
For actions and decisions that affect children, the best interests of the child shall be a fundamental consideration.
Children have the right to protection of their personal integrity. The authorities of the state shall create conditions that facilitate the child's development, including ensuring that the child is provided with the necessary economic, social and health security, preferably within their own family.
(Source: The Constitution of the Kingdom of Norway; https://lovdata.no/NLE/lov/1814-05-17/aicle104)
Constitutional Questions - In the context of this systemic problem, Chapter E: Human Rights, Article 104 of The Constitution of the Kingdom of Norway begs a few direct questions.
- Is a baby a child in Norway?
- Does a baby have the rights of a child in Norway?
- Does a baby "have the right to respect for their human dignity?"
- Does a baby who does not have the ability to make herself heard "due to her age and development...have the right to be heard" through the voice(s) of others who would speak on her behalf, e.g., parents, guardian, attorney etc. "in questions that concern them?"
- Are the "decisions and actions" of a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care "a fundamental consideration" deemed to be in "the best interests of the" baby?
- Does a baby "have the right to protection of their personal integrity?"
- In their "actions and decisions" to implement a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care did "the authorities of the state...create conditions that facilitate a baby's development, including ensuring that the baby is provided with the necessary economic, social and health security, preferably within their own family."
- Again, is a baby a child in Norway?
- Is it time for the official defenders of The Constitution of the Kingdom of Norway to consider the clinical and epidemiological evidence relative to Chapter E: Human Rights, Article 104 of The Constitution of the Kingdom of Norway and then implement the Precautionary Principle with respect to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's plagiarized, misused "method" with a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care?
NCFM eSnurra & Independent Expert Group to Review Abortion
In a letter dated 16.05.2012, Ministry of Health and Care Services commissioned Directorate of Health to assemble an "independent group of experts" to review Norway's regulations and practices related to late-term abortions. This excerpt (below, emphasis added) was taken from the report created by this expert group: "Report: Independent Expert Group for Evaluation of Abortions" ("Rapport: Uavhengig ekspertgruppe for vurdering av svangerskapsavbrudd").
Critical Medical Mistake: First-trimester Ultrasound Exam
At Laila's first-trimester ultrasound exam, 10.08.2016, for a nuchal translucency (NT) measurement (screen for trisomy 13, 18 & 21) the CRL, BPD & FL fetal metrics were measured to establish the NCFM eSnurra EDD & GA values below. Consequently, the NCFM eSnurra EDD & GA lags of 11 days and 9 days (or 1w+2), respectively, from Laila's factual LMPD/OTPD/SCID-based GA & EDD indicated a fetal pathology, such as small for gestational age (SGA), but the lags were either ignored or attributed to a later ovulation date, which could make sense for other pregnancies, but it is a fact Laila's ovulation had not been delayed 9 days. Consequently, the NT scan of 1.4 mm and the blood tests (beta-hCG & PAPP-A) were compared to GA reference curves/charts using an NCFM eSnurra CRL-based GA which was factually inaccurate. This was a critical medical mistake made before Laila's LMPD/OTPD/SCID had been obviated, which appears to make the point, obviated or not, Laila's key pregnancy dates were never considered. Following are the discrepancies.
Laila's NT test was based on an inaccurate NCFM eSnurra CRL-based EDD and, therefrom, a calculated GA = 12w+0, also inaccurate, i.e. relative to LMPD/OTPD/SCID-based GA = 13w+2. The charts included below show NT values in mm for CRL (left) and GA (right). Using NCFM eSnurra CRL = 54 mm shows an NT of 1.2 mm (50th centile, left chart); and CRL-based GA = 12w+0 = NT of 1.2 mm (50th centile, right chart). However, Laila's factual LMPD/OTPD/SCID-based GA = 13w+2 = 1.4 mm NT (50th centile. right chart). The actual ultrasound NT measurement was NT = 1.4 mm which fully corresponded with Laila's factual LMPD/OTPD/SCID-based GA = 13w+2. However, the test results do not indicate if GA or CRL or both were used to assess risk, which is important given that NCFM eSnurra CRL-based GA was lagging Laila's factual LMPD/OTPD/SCID-based GA by 9 days. NCFM eSnurra Group assume CRL of 54 mm is always GA = 12w+0 because NCFM eSnurra must assume no random fetal growth velocity variances nor pathology exist in any of their CRL measurements, or other fetal metric measurements. All NCFM eSnurra CRL measurements are assumed to be accurately average for their corresponding CRL reference GA, i.e., NCFM eSnurra CRL measurements are assumed to be accurately average for their corresponding estimated days remaining from ultrasound date to birth/delivery date from which EDD is calculated and, therefrom, which GA is calculated using the equivalent of Naegele's rule, in reverse.
Using only CRL and NT, i.e., without maternal age and the 2 blood serum levels (beta-hCG & PAPP-A), the perinatology.com website's CRL & NT calculator confirmed CRL = 54 mm mapped to a GA = 12w+0, as would be expected. The results are included below.
In a letter dated 16.05.2012, Ministry of Health and Care Services commissioned Directorate of Health to assemble an "independent group of experts" to review Norway's regulations and practices related to late-term abortions. This excerpt (below, emphasis added) was taken from the report created by this expert group: "Report: Independent Expert Group for Evaluation of Abortions" ("Rapport: Uavhengig ekspertgruppe for vurdering av svangerskapsavbrudd").
- "In Norway, an ultrasound study in full-week 18 is part of pregnancy care. The ultrasound method used systematically for age and term is quality assured against the last menstruation as a method ("Nägeles rule") and generally found better. In Norway, the ultrasound method "Snurra" [4] was introduced in 1984 and soon used throughout the country. The method introduced a review of pregnancy in integers. In 2005, the ultrasound method "The Term Wheel" was published [9]. The population-based method "eSnurra" came in 2007 to improve "Snurra" and "Term wheel" [6], "eSnurra" has been validated last year on 72000 pregnancies [16-18]." (Source: "Report: Independent Expert Group for Evaluation of Abortions" ("Rapport: avhengig ekspertgruppe for vurdering av svangerskapsavbrudd") Oslo 8. april 2013, Stein Kinserdal /s/, Leder., p. 19)
- While Sturla H. Eik-Nes stated "an ultrasound exam in full-week 18 is part of pregnancy care" he did not state the 18-week ultrasound exam was completely optional and voluntary for the pregnant woman, as is explicitly stated in Directorate of Health's publication "A National Clinical Guideline for Antenatal Care: Short Version - Recommendations." Laila had never been informed her routine 18wUSE was completely optional and voluntary. Instead, Laila had been informed by her midwife the 18wUSE was an important part of the pregnancy care, just as it was presented by Sturla H. Eik-Nes in the excerpt above. The reality stated in the Norwegian guidelines is most decidedly different than the reality practiced by Norway's midwives and doctors.
- Also, Sturla H. Eik-Nes stated "The population-based method "eSnurra" came in 2007 to improve "Snurra"." This statement is misleading because Snurra, which used the Campbell Method of GA Estimation (Campbell, 1969) was not improved, it was completely replaced with the Hutchon Method of Population-based Direct EDD Estimation (PDEE) (Hutchon, 1998).
- Additionally, Sturla H. Eik-Nes stated: "The population-based method "eSnurra" came in 2007..." was correct, because ""eSnurra" came in 2007" via the appropriation and plagiarism of Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE), as NCFM eSnurra Group's own original idea and method in NCMF eSnurra Group's Eik-Nes et al. 2005 and then, more prominently, in their Gjessing et al. 2007, both published in Ultrasound in Obstetrics & Gynecology, also known as The White Journal, the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG), of which Sturla H. Eik-Nes had been President (1998-2002), thereby initiating NCFM eSnurra Group's 12-years of ongoing research misconduct via plagiarism. And, earlier, in a recognized NCFM Snurra Group collaboration foregoing authorship credits which resulted in Taipale & Hiilesmaa 2001, which also appropriated and plagiarized the Hutchon Method of PDEE. Taipale was employed by NCFM.
- Moreover, Sturla H. Eik-Nes was President of ISUOG (1998-2002) when Dr. Hutchon's manuscripts (1998 & 1999) presenting his original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE), were submitted to Ultrasound in Obstetrics & Gynecology.
- What is both interesting and significant about this is the report from which these excerpts were taken, as explained above, was commissioned by Ministry of Health & Care Services for Directorate of Health to manage and then deliver to Ministry of Health and Care Services. So much for speaking truth to power.
See: Ethics & Plagiarism > Hutchon Timeline
Critical Medical Mistake: First-trimester Ultrasound Exam
At Laila's first-trimester ultrasound exam, 10.08.2016, for a nuchal translucency (NT) measurement (screen for trisomy 13, 18 & 21) the CRL, BPD & FL fetal metrics were measured to establish the NCFM eSnurra EDD & GA values below. Consequently, the NCFM eSnurra EDD & GA lags of 11 days and 9 days (or 1w+2), respectively, from Laila's factual LMPD/OTPD/SCID-based GA & EDD indicated a fetal pathology, such as small for gestational age (SGA), but the lags were either ignored or attributed to a later ovulation date, which could make sense for other pregnancies, but it is a fact Laila's ovulation had not been delayed 9 days. Consequently, the NT scan of 1.4 mm and the blood tests (beta-hCG & PAPP-A) were compared to GA reference curves/charts using an NCFM eSnurra CRL-based GA which was factually inaccurate. This was a critical medical mistake made before Laila's LMPD/OTPD/SCID had been obviated, which appears to make the point, obviated or not, Laila's key pregnancy dates were never considered. Following are the discrepancies.
- NCFM eSnurra CRL-based EDD = 25.02.2017, which lagged Laila's factual LMPD/OTPD/SCID-based EDD by 11 days
NCFM eSnurra CRL-based GA = 12w+0, which lagged Laila's factual LMPD/OTPD/SCID-based GA by 9 days - NCFM eSnurra BPD-based EDD = 22.02.2017, which lagged Laila's factual LMPD/OTPD/SCID-based EDD by 8 days
NCFM eSnurra BPD-based GA= 12w+3, which lagged Laila's factual LMPD/OTPD/SCID-based GA by 6 days
[Note: EDD & GA were not provided for FL on the ultrasound report]
Laila's NT test was based on an inaccurate NCFM eSnurra CRL-based EDD and, therefrom, a calculated GA = 12w+0, also inaccurate, i.e. relative to LMPD/OTPD/SCID-based GA = 13w+2. The charts included below show NT values in mm for CRL (left) and GA (right). Using NCFM eSnurra CRL = 54 mm shows an NT of 1.2 mm (50th centile, left chart); and CRL-based GA = 12w+0 = NT of 1.2 mm (50th centile, right chart). However, Laila's factual LMPD/OTPD/SCID-based GA = 13w+2 = 1.4 mm NT (50th centile. right chart). The actual ultrasound NT measurement was NT = 1.4 mm which fully corresponded with Laila's factual LMPD/OTPD/SCID-based GA = 13w+2. However, the test results do not indicate if GA or CRL or both were used to assess risk, which is important given that NCFM eSnurra CRL-based GA was lagging Laila's factual LMPD/OTPD/SCID-based GA by 9 days. NCFM eSnurra Group assume CRL of 54 mm is always GA = 12w+0 because NCFM eSnurra must assume no random fetal growth velocity variances nor pathology exist in any of their CRL measurements, or other fetal metric measurements. All NCFM eSnurra CRL measurements are assumed to be accurately average for their corresponding CRL reference GA, i.e., NCFM eSnurra CRL measurements are assumed to be accurately average for their corresponding estimated days remaining from ultrasound date to birth/delivery date from which EDD is calculated and, therefrom, which GA is calculated using the equivalent of Naegele's rule, in reverse.
Using only CRL and NT, i.e., without maternal age and the 2 blood serum levels (beta-hCG & PAPP-A), the perinatology.com website's CRL & NT calculator confirmed CRL = 54 mm mapped to a GA = 12w+0, as would be expected. The results are included below.
- "For the crown rump length (CRL) of 54 mm the predicted gestational age is 12 weeks 0 days. The expected nuchal translucency (NT) is 1.50 mm (50th percentile)
Your measured NT value is 43 percentile for this CRL."
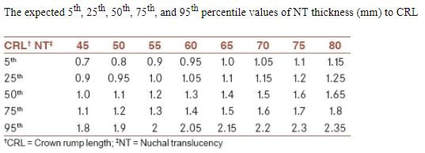
|
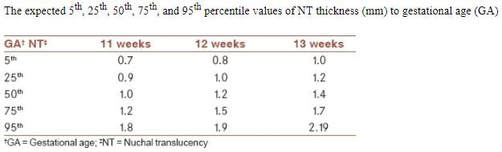
|
(Source: "Normal reference range of fetal nuchal translucency thickness in pregnant women in the first trimester, one center study" Marzeie Sharifzadeh, Atoosa Adibi, Kimia Kazemi, and Silva Hovsepian. J Res Med Sci. 2015 Oct; 20(10): 969–973.)
Ultrasound-based Fetal Metric Measurements with GA & EDD
Included below are the data from all of Laila's ultrasound exams.
Included below are the data from all of Laila's ultrasound exams.
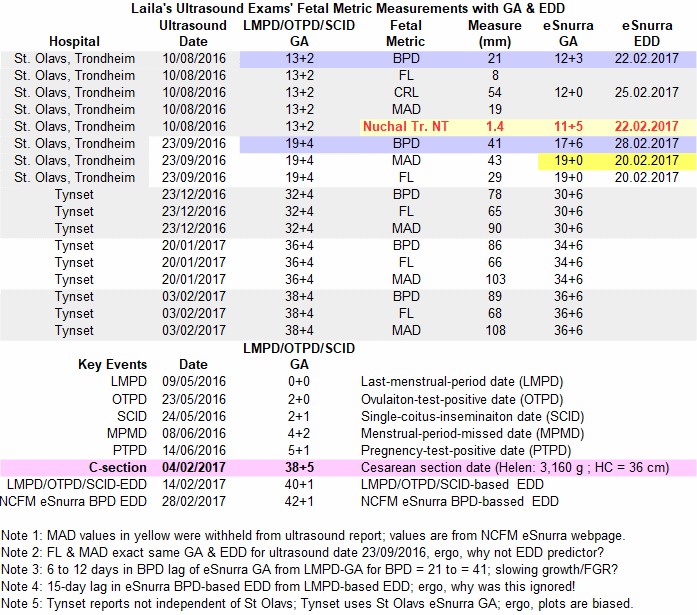
The links to the pregnancy and ultrasound calculators included below can be used with Laila's key pregnancy dates and ultrasound data (above) to develop a hands-on understanding. For example, how would one interpret:
UpToDate: Calculator: Estimated Date of Delivery (EDD)
(Source: UpToDate.com: https://www.uptodate.com/contents/13505)
(Source: UpToDate.com: https://www.uptodate.com/contents/13503)
UpToDate: Calculator: Estimated date of delivery (EDD) (Patient education)
(Source: UpToDate.com: https://www.uptodate.com/contents/13504)
NCFM eSnurra BPD-based GA Systemically Biases Ultrasound Reports from Other Hospitals
The advantage of having the same medical exam conducted at two separate hospitals, assuming they are neither sharing personnel nor exam/lab facilities, is their independence. Two, separate, independent exams yield two separate, independent exam results and two separate, independent exam reports. With respect to Laila's Tynset Hospital ultrasound exams, the fetal metric measurements were completely independent of the fetal metric measurements from her ultrasound exams at St Olavs Hospital. However, none of Laila's ultrasound exam reports from Tynset Hospital were independent of her ultrasound exam reports at St Olavs Hospital. All of Laila's ultrasound reports from Tynset Hospital are biased by her ultrasound reports from St Olavs Hospital. Specifically, the Tynset sonographer acquired the NCFM eSnurra BPD-based GA for that day by using the NCFM eSnurra BPD-based GA from the exam report from St Olavs to plot the BPD, FL & MAD measurements made at Tynset Hospital to create their respective fetal metric growth-chart curves. Specifically, the sources of x-axis data (i.e., time or GA) were calculated using GA from St. Olavs exam reports while the y-axis data (fetal metric measurements) were from Tynset Hospital's measurements. Consequently, the same grossly inaccurate 12-day lag of NCFM eSnurra BPD-based GA was incorporated into each of Tynset Hospital's plots of BPD, FL & MAD measurements vs. GA (i.e., their respective growth curves), which does 2 things, systemically:
More on BPD Confirmation Bias
Getting back to BPD confirmation bias: The page of Tynset Hospital's ultrasound report has room for 2 growth curve plots. Tynset Hospital plotted BPD and MAD on the same page, but did not plot FL. It would have been interesting to have had a side-by-side visual of BPD and FL to see how well each was tracking its respective growth cure (albeit BPD- and FL-based GA lagging Laila's factual LMPD/OTPD/SCID-based GA by 12 days and 8 days, respectively) given that the NCFM eSnurra website states:
Cost Comparison
There appears to be general consensus in the literature that it is more important for fetal age and GA to be accurate than for a woman to deliver on or near her EDD. This makes sense considering a woman only has a 4% chance of her birth/delivery occurring on her EDD. Consider the additional medical risks, consequences and costs if a woman of normal pregnancy misses her EDD by 1 day or 2 days or 3 days or even 10 days. Again, given that less than 4% of normal pregnancies actual deliver on their EDD, one might reasonably expect the additional medical risks and medical costs to be insignificant or close to zero, again for normal pregnancies. However, what are the additional medical risks, consequences and medical costs of an NCFM eSnurra GA lagging a factual LMPD/OTPD/SCID-based GA by 1w+5 (or 12 days) and, correspondingly, an NCFM eSnurra EDD lagging a factual LMPD/OTPD/SCID-based EDD by 2w+0 (or 14 days) while masking fetal pathology?
While wearing a blindfold to cross a street of low traffic volume is neither smart nor responsible behavior; this blindfolded-street-crossing behavior might take a long time to result in harm. However, the possibly many no-harm-street-crossings are not evidence of the absence of risk of grievous or deadly consequences for intentional, irresponsible, blindfolded-street-crossing behavior (Risk x Consequences = Expected Harm).
Institutional Confirmation Bias & Doublethink
Laila's baby was officially recorded as NCFM eSnurra BPD-based GA = 37w+0 (or 36w+6 depending on the version of eSnurra) at delivery, a preterm as classified by NCFM eSnurra Group, yet, other than the grossly inaccurate NCFM eSnurra EDD & GA, there is no medical evidence to indicate Laila's baby was preterm; there is no such evidence, whatsoever, before or after Laila's Cesarean section surgery delivery. So, why is Laila's baby still "officially" classified as GA = 37w+0 at delivery; a GA everyone now knows was grossly inaccurate, completely erroneous, and flat-out wrong. The reason is because this insidious problem created by Directorate of Health's 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine with their exclusive NCFM eSnurra implementation is systemic and institutionalized. It's because of systemic, institutionalized confirmation bias and doublethink. Laila's medical professionals know Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD were correct from the very beginning, but they are not allowed to acknowledge this truth, this reality. They all know, and knew, Laila's factual LMPD/OTPD/SCID-based GA & EDD were correct while they also knew they had to conform to Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive NCFM eSnurra implementation with a government-mandated protocol of evidence-obviated medicine; a government-mandated protocol in which they are mandated to trust in order to "believe" and, consequently, they want to "believe," so they do "believe," with doublethink. Laila's medical professionals were, and some still are, holding two contradictory beliefs in their minds, simultaneously:
Critical Mistakes: Medical Birth Registry of Norway (MBRN)
A unique and interesting medical editorial "How long does a pregnancy last?" includes a graph showing the variance of pregnancy duration using data from the Medical Birth Registry of Norway (MBRN), administered by the Norwegian Institute of Public Health (NIPH). The description of the data and its MBRN source made it clear Laila's baby, Helen, would have her grossly inaccurate, completely erroneous, flat-out wrong NCFM eSnurra BPD-based GA = 37w+0 at delivery sealed, forever, in her permanent national medical birth record at MBRN, like a seed sequestered in the Svalbard Global Seed Vault, and just when Laila & Edward thought this knowledge-obviated medical policy with its government-mandated protocol of evidence-obviated medicine problem could not possibly become any more insidious, systemic or institutionalized. Think about it. Helen's first contribution of personal medical evidence of her existence was her grossly inaccurate, completely erroneous, flat-out wrong NCFM eSnurra BPD-based eSnurra GA of 37w+0 at delivery; false medical evidence which was proven to be false, mathematically, was entered into Helen's permanent medical birth record and then this false medical evidence of a newborn Norwegian citizen (also an American citizen) was entered, permanently, into her national medical birth record without any means of stopping it.
The Law & MBRN Data Integrity
To intentionally include data known to be factually incorrect (such as Helen's grossly inaccurate, completely erroneous, flat-out wrong NCFM BPD-based GA = 37w+0 at delivery) into individual medical birth records and medical research datasets is an act of research misconduct via falsification. There are specific legal penalties for this with respect to the data submitted to MBRN, which could also be argued extend to Directorate of Health's medically & ethically flawed 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine, which obviates a woman's key pregnancy dates (e.g., LMPD/OTPD/SCID) at the scheduling of the 18-week ultrasound exam; a government-mandated protocol which is the epitome of, and a monument to, intentional recklessness and willful negligence.
Interestingly, the above referenced medical editorial "How long does a pregnancy last?" was published in 2012. Shortly thereafter, a 2013 study (and other studies) provided fact-based evidence in support of important, relevant points made in this medical editorial (first 2 excerpts below). The third excerpt makes the point about measurement precision: "since length of pregnancy is subject to biological variation and other factors."
Norway's Abortion Law
Interestingly, Norway's abortion law is specifically and explicitly based on gestational age, not estimated date of delivery (EDD).
Norway's health authorities (i.e., Norway's Ministry of Health & Care Services and Directorate of Health) selected, implemented and promoted a science-bending, medically & ethically flawed 2014 national medical policy for obstetric & fetal medicine which includes a government-mandated protocol of evidence-obviated medicine (without patients’ informed consent) to ensure unilateral reliance on Norway's National Center for Fetal Medicine (NCFM) Group's ultrasound-based eSnurra EDD estimation "method" to establish the clinically important gestational age for all pregnancies and abortions in Norway. However, this national medical policy is proven to systemically misclassify gestational age, which causes suboptimal obstetric & fetal awareness, which causes suboptimal obstetric & fetal management, unnecessarily. Moreover, NCFM Group's unilateral, ultrasound-based eSnurra "method" estimates EDD, not the clinically important gestational age upon which obstetric & fetal medicine decisions and abortion adjudications are based. Furthermore, Norway's Abortion Act is entirely based on gestational age, not EDD. In fact, EDD is not mentioned in Norway's Abortion Act, Norway's Abortion Regulations nor Norway's Abortion Register Regulations, i.e., Lov om svangerskapsavbrudd [abortloven], Forskrift om svangerskapsavbrudd (abortforskriften) and Forskrift om innsamling og behandling av helseopplysninger i register over svangerskapsavbrudd (abortregisterforskriften), respectively. Consequently, Norway's health authorities and NCFM Group decided (in conscious disregard of the explicit, published warnings of the risks & consequences identified by Norway's obstetric & fetal medicine experts, international practice guidelines and Norway’s epidemiological experts) to calculate gestational age by using the equivalent of Naegele's rule, but in reverse, by assuming, erroneously, LMP = EDD – 283 days for all pregnancies and abortion adjudications in Norway. In short, estimating gestational age and estimating EDD are not synonymous for individual pregnancies.
In effect, and in reality, Norway's health authorities and NCFM Group implemented authority-based medicine over evidence-based medicine, surreptitiously, in conscious disregard of Norway's Abortion Act and Norway's Abortion Regulations while causing increased medical risks, critical medical mistakes and grievous medical harms, unnecessarily, for some of Norway's women and their fetuses/babies., a violation of the public trust. Not surprisingly, Norway's health authorities' actions might reasonably be classified as a form of tyranny. (Sources: 1) Lov om svangerskapsavbrudd [abortloven] (Pregnancy Abortion Act [Abortion Act]), 2) Forskrift om svangerskapsavbrudd (abortforskriften) (Pregnancy Abortion Regulations (Abortion Regulations); and 3) View/Download: Synopsis of Situation pdf)
- Laila's factual key pregnancy dates, alone?
- the ultrasound data, alone?
- the ultrasound data in conjunction with Laila's factual, key pregnancy dates individually
- the ultrasound data in conjunction with Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA?
- the ultrasound data, alone, to screen for SGA or other fetal pathology?
- the ultrasound data used in conjunction with Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA to screen for SGA or other fetal pathology?
- Calculate estimated due date (EDD) and gestational age
- Due Date from Utrasound Report
- Calculate Gestational Age from Ultrasound Measurements
- Estimated Gestational Age and Fetal Weight Calculator (from ultrasound report)
- Fetal Biometry Calculator II (more advanced)
- Crown Rump Length and Nuchal Translucency
UpToDate: Calculator: Estimated Date of Delivery (EDD)
(Source: UpToDate.com: https://www.uptodate.com/contents/13505)
- Input:
Current date Feb 04, 2017 [Note: Current date is set to actual date of delivery.]
Last menstrual period May 09, 2016
Ultrasound date September 23, 2016
Gestational age by ultrasound 17 weeks 6 days [Note: NCFM eSnurra BPD-based GA, exclusively] - Results:
Current gestational age by LMP 38 weeks 5 days [Note: Current date is set to actual date of delivery.]
EDD by LMP Feb 13, 2017 [Note: EDD Error = (Predicted - Actual) = 9 days]
Current gestational age by US 37 weeks 0 days [Note: NCFM eSnurra BPD-based GA, exclusively]
EDD by US Feb 25, 2017 [Note: EDD Error = (Predicted - Actual) = 22 days (or > 3 weeks)]
- This calculator gives you two options for estimating EDD.
- Enter either the date of the first day of the last menstrual period (LMP), or the date of an ultrasound examination and the gestational age by ultrasound (US).
- Input any parameters to compare the two date calculations.
- Gestational age by LMP is calculated from the first day of the last menstrual period.
- EDD by LMP is calculated by adding 280 days (40 weeks) to the first day of the last menstrual period.
- Gestational age by US is measured by ultrasound (US) on the Ultrasound Date.
- EDD by US is the estimated date of delivery based on the Gestational age by US and the Ultrasound date. It is the Ultrasound date + (280 [days] - Gestational age by ultrasound [days] on the Ultrasound date).
- Mul T, Mongelli M, Gardosi J. A comparative analysis of second-trimester ultrasound dating formulae in pregnancies conceived with artificial reproductive techniques. Ultrasound Obstet Gynecol 1996; 8:397.
- Westerway SC, Davison A, Cowell S. Ultrasonic fetal measurements: new Australian standards for the new millennium. Aust N Z J Obstet Gynaecol 2000; 40:297.
- Altman DG, Chitty LS. New charts for ultrasound dating of pregnancy. Ultrasound Obstet Gynecol 1997; 10:174."
(Source: UpToDate.com: https://www.uptodate.com/contents/13503)
- Input:
Current date Feb 04, 2017 [Note: Current date is set to actual date of delivery.]
EDD Feb 25, 2017 [Note: EDD Error = (Predicted - Actual) = 21 days (or 3 weeks)]
Results:
Current gestational age by EDD 37 weeks 0 days [Note: Current gestational age by LMP 38 weeks 5 days; this 12-day difference is the warning signal which was repeatedly ignored by all medical professionals.]
Notes none
References none
UpToDate: Calculator: Estimated date of delivery (EDD) (Patient education)
(Source: UpToDate.com: https://www.uptodate.com/contents/13504)
- Input:
Today's date Feb 04, 2017 [Note: Today's date is set to actual date of delivery.]
First day of last period May 09, 2016
Results:
Estimated due date Feb 13, 2018
Estimated gestational age 38 weeks 5 days
- This calculator helps you estimate your date of delivery ("due date") based on the timing of your last menstrual period.
- Gestational age estimates how far along you are in your pregnancy. Your health care provider uses the gestational age in weeks (rather than months) to plan your care during pregnancy. Most pregnancies last about 40 weeks from the first day of the last menstrual period.
- To calculate your estimated due date and gestational age, enter the current date and the date your last menstrual period started."
NCFM eSnurra BPD-based GA Systemically Biases Ultrasound Reports from Other Hospitals
The advantage of having the same medical exam conducted at two separate hospitals, assuming they are neither sharing personnel nor exam/lab facilities, is their independence. Two, separate, independent exams yield two separate, independent exam results and two separate, independent exam reports. With respect to Laila's Tynset Hospital ultrasound exams, the fetal metric measurements were completely independent of the fetal metric measurements from her ultrasound exams at St Olavs Hospital. However, none of Laila's ultrasound exam reports from Tynset Hospital were independent of her ultrasound exam reports at St Olavs Hospital. All of Laila's ultrasound reports from Tynset Hospital are biased by her ultrasound reports from St Olavs Hospital. Specifically, the Tynset sonographer acquired the NCFM eSnurra BPD-based GA for that day by using the NCFM eSnurra BPD-based GA from the exam report from St Olavs to plot the BPD, FL & MAD measurements made at Tynset Hospital to create their respective fetal metric growth-chart curves. Specifically, the sources of x-axis data (i.e., time or GA) were calculated using GA from St. Olavs exam reports while the y-axis data (fetal metric measurements) were from Tynset Hospital's measurements. Consequently, the same grossly inaccurate 12-day lag of NCFM eSnurra BPD-based GA was incorporated into each of Tynset Hospital's plots of BPD, FL & MAD measurements vs. GA (i.e., their respective growth curves), which does 2 things, systemically:
- artificially decreases MAD's GA value (x-axis, time) relative to Laila's LMPD/OTPD/SCID-based GA, thus shifting MAD left, which causes MAD to "appear" to rise above the growth curve, thereby making it seem as though MAD is leading the growth curve when, in reality, MAD is either on or very close to the growth curve; and
- artificially decreases the BPD's GA value (x-axis, time) relative to Laila's factual LMPD/OTPD/SCID-based GA, thus shifting BPD left 12 days, which causes BPD to "appear" to rise up toward the growth curve making it seem as though BPD is tracking closer to the growth curve when, in reality, BPD is significantly further below the growth curve and, in Laila's case, 12 days further to the left (plus any additional FGR/malformation effect on BPD as a function of increasing GA.)
More on BPD Confirmation Bias
Getting back to BPD confirmation bias: The page of Tynset Hospital's ultrasound report has room for 2 growth curve plots. Tynset Hospital plotted BPD and MAD on the same page, but did not plot FL. It would have been interesting to have had a side-by-side visual of BPD and FL to see how well each was tracking its respective growth cure (albeit BPD- and FL-based GA lagging Laila's factual LMPD/OTPD/SCID-based GA by 12 days and 8 days, respectively) given that the NCFM eSnurra website states:
- Basically, BPD should be used. In deviating head shape, FL is used to provide the same precise term as BPD. BPD and FL quality assure each other and therefore both should be filled out." ("I utgangspunktet skal BPD brukes. Ved avvikende hodeform brukes FL som gir like presis termin som BPD. BPD og FL kvalitetssikrer hverandre og derfor bør begge fylles ut.") (Source: NCFM eSNurra website: http://www.nsfm.no/esnurra/2.php)
- How to use eSnurra
Whatever version of eSnurra you are using, it is important to use the method correctly.
• From week 8/0 to 12/0, CRL is most accurate for EDD settiing.
• From week 12/0 to 22/6, BPD is most accurate for EDD setting if the shape of the scull is normal.
• From week 15/6 to 22/6, FL can be used to quality assure the BPD measurement.
• eSnurra use a median pregnancy lenght of 283 days
• Use the average of 3 BPD measurements from outher [sic] to outer limits when measuring the fetal scull.
• Use the largest of 3 FL-measurements.
It is important to use the method this way – especially when you use the plastic wheel where you can determine the EDD from any factor, but the method described above will be more accurate. (Source: NCFM eSnurra Group's Website: from 18.03.2016, via https://web.archive.org/web/20160318081147/http://www.esnurra.com/how-to-use-esnurra/)
Cost Comparison
There appears to be general consensus in the literature that it is more important for fetal age and GA to be accurate than for a woman to deliver on or near her EDD. This makes sense considering a woman only has a 4% chance of her birth/delivery occurring on her EDD. Consider the additional medical risks, consequences and costs if a woman of normal pregnancy misses her EDD by 1 day or 2 days or 3 days or even 10 days. Again, given that less than 4% of normal pregnancies actual deliver on their EDD, one might reasonably expect the additional medical risks and medical costs to be insignificant or close to zero, again for normal pregnancies. However, what are the additional medical risks, consequences and medical costs of an NCFM eSnurra GA lagging a factual LMPD/OTPD/SCID-based GA by 1w+5 (or 12 days) and, correspondingly, an NCFM eSnurra EDD lagging a factual LMPD/OTPD/SCID-based EDD by 2w+0 (or 14 days) while masking fetal pathology?
While wearing a blindfold to cross a street of low traffic volume is neither smart nor responsible behavior; this blindfolded-street-crossing behavior might take a long time to result in harm. However, the possibly many no-harm-street-crossings are not evidence of the absence of risk of grievous or deadly consequences for intentional, irresponsible, blindfolded-street-crossing behavior (Risk x Consequences = Expected Harm).
Institutional Confirmation Bias & Doublethink
Laila's baby was officially recorded as NCFM eSnurra BPD-based GA = 37w+0 (or 36w+6 depending on the version of eSnurra) at delivery, a preterm as classified by NCFM eSnurra Group, yet, other than the grossly inaccurate NCFM eSnurra EDD & GA, there is no medical evidence to indicate Laila's baby was preterm; there is no such evidence, whatsoever, before or after Laila's Cesarean section surgery delivery. So, why is Laila's baby still "officially" classified as GA = 37w+0 at delivery; a GA everyone now knows was grossly inaccurate, completely erroneous, and flat-out wrong. The reason is because this insidious problem created by Directorate of Health's 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine with their exclusive NCFM eSnurra implementation is systemic and institutionalized. It's because of systemic, institutionalized confirmation bias and doublethink. Laila's medical professionals know Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD were correct from the very beginning, but they are not allowed to acknowledge this truth, this reality. They all know, and knew, Laila's factual LMPD/OTPD/SCID-based GA & EDD were correct while they also knew they had to conform to Directorate of Health's medically & ethically flawed 2014 Recommendation with their exclusive NCFM eSnurra implementation with a government-mandated protocol of evidence-obviated medicine; a government-mandated protocol in which they are mandated to trust in order to "believe" and, consequently, they want to "believe," so they do "believe," with doublethink. Laila's medical professionals were, and some still are, holding two contradictory beliefs in their minds, simultaneously:
- their mandated trust and belief in the Directorate of Health's 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) with a government-mandated protocol of evidence-obviated medicine at the scheduling of the 18-week ultrasound exam, without pregnant women's prior, informed, voluntary, explicit consent and
- their belief in the evidence of their own senses; their own thinking and use of fundamental mathematics to know and understand that Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD were accurate and that Laila's NCFM eSnurra BPD-based GA & EDD and her baby's NCFM eSnurra GA = 37w+0 at delivery were grossly inaccurate, especially given the NCFM eSnurra BPD-based EDD prediction error of -24 days, but still accepting both beliefs, simultaneously.
- "DOUBLETHINK means the power of holding two contradictory beliefs in one’s mind simultaneously, and accepting both of them. The Party intellectual knows in which direction his memories must be altered; he therefore knows that he is playing tricks with reality; but by the exercise of DOUBLETHINK he also satisfies himself that reality is not violated. The process has to be conscious, or it would not be carried out with sufficient precision, but it also has to be unconscious, or it would bring with it a feeling of falsity and hence of guilt" (Source: George Orwell, "1984," Part Two, Chapter 9)
Critical Mistakes: Medical Birth Registry of Norway (MBRN)
A unique and interesting medical editorial "How long does a pregnancy last?" includes a graph showing the variance of pregnancy duration using data from the Medical Birth Registry of Norway (MBRN), administered by the Norwegian Institute of Public Health (NIPH). The description of the data and its MBRN source made it clear Laila's baby, Helen, would have her grossly inaccurate, completely erroneous, flat-out wrong NCFM eSnurra BPD-based GA = 37w+0 at delivery sealed, forever, in her permanent national medical birth record at MBRN, like a seed sequestered in the Svalbard Global Seed Vault, and just when Laila & Edward thought this knowledge-obviated medical policy with its government-mandated protocol of evidence-obviated medicine problem could not possibly become any more insidious, systemic or institutionalized. Think about it. Helen's first contribution of personal medical evidence of her existence was her grossly inaccurate, completely erroneous, flat-out wrong NCFM eSnurra BPD-based eSnurra GA of 37w+0 at delivery; false medical evidence which was proven to be false, mathematically, was entered into Helen's permanent medical birth record and then this false medical evidence of a newborn Norwegian citizen (also an American citizen) was entered, permanently, into her national medical birth record without any means of stopping it.
- "After registration at the first prenatal visit, the last menstrual period date given by the mother is supposedly left unchanged until it is transferred to the registry, regardless of whether it is in accordance with ultrasound dating and whether it is certain or not. Thus, a pattern of systematic errors may be more evident in the Norwegian material than elsewhere." (Source: "Errors in Gestational Age: Evidence of Bleeding Early in Pregnancy" Håkon K. Gjessing, PhD, Rolv Skjcerven, PhD, and Allen J. Wilcox, MD, PhD, American Journal of Public Health, February 1999, Vol. 89, No. 2 , p. 216) [Note: The irony is not lost.]
The Law & MBRN Data Integrity
To intentionally include data known to be factually incorrect (such as Helen's grossly inaccurate, completely erroneous, flat-out wrong NCFM BPD-based GA = 37w+0 at delivery) into individual medical birth records and medical research datasets is an act of research misconduct via falsification. There are specific legal penalties for this with respect to the data submitted to MBRN, which could also be argued extend to Directorate of Health's medically & ethically flawed 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine, which obviates a woman's key pregnancy dates (e.g., LMPD/OTPD/SCID) at the scheduling of the 18-week ultrasound exam; a government-mandated protocol which is the epitome of, and a monument to, intentional recklessness and willful negligence.
- Medical Birth Registry Regulations
Chapter 7. Penalties
§ 7-1. (Penalty)
Anyone who deliberately or through gross negligence contravenes provisions laid down in this Regulation § 1-2, § 3-2 and § 4-2 to § 4-4, punishable by a fine or imprisonment not exceeding one year or both.
Complicity is punishable in the same way. (Source: Forskrift om innsamling og behandling av helseopplysninger i Medisinsk fødselsregister (Medisinsk fødselsregisterforskriften)
Interestingly, the above referenced medical editorial "How long does a pregnancy last?" was published in 2012. Shortly thereafter, a 2013 study (and other studies) provided fact-based evidence in support of important, relevant points made in this medical editorial (first 2 excerpts below). The third excerpt makes the point about measurement precision: "since length of pregnancy is subject to biological variation and other factors."
- "The median time from ovulation to birth was 268 days (38 weeks, 2 days). Even after excluding six preterm births, the gestational length range was 37 days."
- "Human gestational length varies considerably even when measured exactly (from ovulation). An individual woman’s deliveries tend to occur at similar gestational ages. Events in the first 2 weeks after conception are predictive of subsequent pregnancy length, and may suggest pathways underlying the timing of delivery." (Source: Length of human pregnancy and contributors to its natural variation A.M. Jukic, D.D. Baird, C.R. Weinberg, D.R. McConnaughey, and A.J. Wilcox, Human Reproduction, Vol.28, No.10 pp. 2848–2855, 2013)
- "As the observations above indicate, trials may well prove that a natural method to predict the day of delivery is more precise than the current technological approach. However, there is a limit to the precision of any method, since length of pregnancy is subject to biological variation and other factors. The current methods, corrected for bias, may well be close to this limit." (Source: Routine ultrasound dating has not been shown to be more accurate than the calendar method. Olsen, O. and Aaroe Clausen, J. (1997), BJOG: An International Journal of Obstetrics & Gynaecology, 104: 1221–1222. doi:10.1111/j.1471-0528.1997.tb10965.x)
Norway's Abortion Law
Interestingly, Norway's abortion law is specifically and explicitly based on gestational age, not estimated date of delivery (EDD).
- "Information about applying for termination (abortion) after pregnancy week 12
In Norway, women have the right to abortion on demand within the first twelve weeks of gestation (11 weeks and 6 days). If you wish to have an abortion after the 12-week time limit, you must apply to a special medical assessment board – called an ’abortion board’ (Norwegian: ‘abortnemnd’ or ‘primærnemnd’) – that will determine whether or not to grant you an abortion.
The duration of a pregnancy is calculated from the first day of the last menstrual period, but is determined more precisely by an ultrasound scan. You have the right to receive the information you believe you need in order to decide to terminate a pregnancy.
To apply for an abortion after the 12th week of gestation (11 weeks and 6 days), you can contact a hospital directly, your regular GP, a gynaecologist or another medical doctor. It is important to get an appointment as soon as possible. If you are uncertain about when you had your last menstrual period or if your periods are irregular, it is important to mention this when contacting the doctor/hospital."
(...)
"Approval or denial of your application
The longer you have been pregnant, the stricter the requirements for being granted an abortion. After the end of the 18th week of gestation (17 weeks + 6 days), the pregnancy cannot be terminated except on grounds of grave risk. A foetus is presumed to be viable from the end of the 22nd week of gestation (21 weeks + 6 days), from which time abortion is prohibited by Norwegian law. However, if there is something seriously wrong with the foetus so it is not viable, you will be eligible for abortion throughout the pregnancy." (Source: "Information about applying for termination (abortion) after pregnancy week 12" Helsedirektoratet, Norwegian Directorate of Health, IS-0603E)
Norway's health authorities (i.e., Norway's Ministry of Health & Care Services and Directorate of Health) selected, implemented and promoted a science-bending, medically & ethically flawed 2014 national medical policy for obstetric & fetal medicine which includes a government-mandated protocol of evidence-obviated medicine (without patients’ informed consent) to ensure unilateral reliance on Norway's National Center for Fetal Medicine (NCFM) Group's ultrasound-based eSnurra EDD estimation "method" to establish the clinically important gestational age for all pregnancies and abortions in Norway. However, this national medical policy is proven to systemically misclassify gestational age, which causes suboptimal obstetric & fetal awareness, which causes suboptimal obstetric & fetal management, unnecessarily. Moreover, NCFM Group's unilateral, ultrasound-based eSnurra "method" estimates EDD, not the clinically important gestational age upon which obstetric & fetal medicine decisions and abortion adjudications are based. Furthermore, Norway's Abortion Act is entirely based on gestational age, not EDD. In fact, EDD is not mentioned in Norway's Abortion Act, Norway's Abortion Regulations nor Norway's Abortion Register Regulations, i.e., Lov om svangerskapsavbrudd [abortloven], Forskrift om svangerskapsavbrudd (abortforskriften) and Forskrift om innsamling og behandling av helseopplysninger i register over svangerskapsavbrudd (abortregisterforskriften), respectively. Consequently, Norway's health authorities and NCFM Group decided (in conscious disregard of the explicit, published warnings of the risks & consequences identified by Norway's obstetric & fetal medicine experts, international practice guidelines and Norway’s epidemiological experts) to calculate gestational age by using the equivalent of Naegele's rule, but in reverse, by assuming, erroneously, LMP = EDD – 283 days for all pregnancies and abortion adjudications in Norway. In short, estimating gestational age and estimating EDD are not synonymous for individual pregnancies.
In effect, and in reality, Norway's health authorities and NCFM Group implemented authority-based medicine over evidence-based medicine, surreptitiously, in conscious disregard of Norway's Abortion Act and Norway's Abortion Regulations while causing increased medical risks, critical medical mistakes and grievous medical harms, unnecessarily, for some of Norway's women and their fetuses/babies., a violation of the public trust. Not surprisingly, Norway's health authorities' actions might reasonably be classified as a form of tyranny. (Sources: 1) Lov om svangerskapsavbrudd [abortloven] (Pregnancy Abortion Act [Abortion Act]), 2) Forskrift om svangerskapsavbrudd (abortforskriften) (Pregnancy Abortion Regulations (Abortion Regulations); and 3) View/Download: Synopsis of Situation pdf)