"The Fix"
Directorate of Health & NCFM eSnurra Group
Directorate of Health & NCFM eSnurra Group
Directorate of Health Exceeded Their Competence
Directorate of Health's statement (below) in their 2016 article published in Tidsskr Nor Legeforen betrays their confusion and competence.
Second, Fetal age and EDD do "need to be considered in conjunction." The conjunction in which fetal age and EDD need to be considered is the fact that actual birth/delivery date varies, naturally, over a 35+ day range, even when fetal age and gestational age (GA) are measured exactly from time of IVF or ovulation. Consequently, fetal age and gestational age should be established as directly, early and accurately as possible by including "all available information when fetal age is assessed" to ensure and accurate temporal frame of reference to ensure optimal obstetric and fetal awareness to ensure optimal obstetric and fetal management. NGF i.e., Norsk gynekologisk forening (Norwegian Gynecological & Obstetrics Association) made this clear to Directorate of Health (Hdir). Included below are excerpts from NDG's 2014 article "NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin."
Moreover, it appears Torunn Janbu was not aware Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE) had been formulated by Dr. Hutchon and published, along with a demonstration of the method using a dataset of both CRL and BPD in his seminal Hutchon 1998 and website 7 years and 9 years before NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, in which NCFM eSnurra Group laid claim to Dr. Hutchon's original idea and method as their own original idea and method, thereby engaging in ongoing research misconduct via plagiarism for the last 12-years.
In his seminal Hutchon 1998, Dr. Hutchon explicitly warned against using Population-based Direct EDD Estimation to assess GA and fetal age because Dr. Hutchon understood that the basis for determining fetal age is not the end of the pregnancy, but its beginning and that all available information should be used when assessing fetal age. This is covered in detail elsewhere in this document.
Additionally, Torunn Janbu ignored all the obstetric & fetal medicine experts who had so clearly and explicitly warned of the risks and consequences: "that critical mistakes may follow from the failure to include all available information when fetal age is assessed," as was explained above, but bears repeating.
Directorate of Health completely ignored fact-based evidence of serious data irregularities with respect to the integrity of the BPD data in NCFM eSnurra Group's studies and publications.
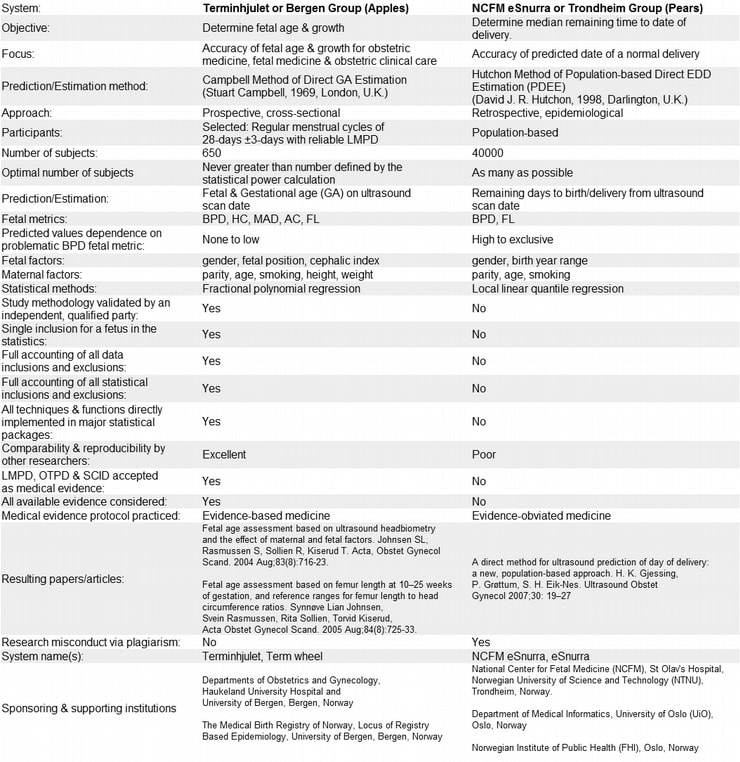
The Directorate of Health's comparison of Bergen Group's method (Terminhjulet or Term Wheel) and NCFM eSnurra Group or Trondheim Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) was an insult to:
Directorate of Health's statement (below) in their 2016 article published in Tidsskr Nor Legeforen betrays their confusion and competence.
- "Fetal age and EDD always need to be considered in conjunction. In Terminhjulet, the EDD is derived from the age, in eSnurra the age is derived from the date of delivery." (Source: "One Norwegian national tool for estimating date of delivery and fetal age" Torunn Janbu, Head of the Department of Hospital Services, Norwegian Directorate of Health Tidsskr Nor Legeforen nr. 9, 2016; 136: 790 – 1.)
Second, Fetal age and EDD do "need to be considered in conjunction." The conjunction in which fetal age and EDD need to be considered is the fact that actual birth/delivery date varies, naturally, over a 35+ day range, even when fetal age and gestational age (GA) are measured exactly from time of IVF or ovulation. Consequently, fetal age and gestational age should be established as directly, early and accurately as possible by including "all available information when fetal age is assessed" to ensure and accurate temporal frame of reference to ensure optimal obstetric and fetal awareness to ensure optimal obstetric and fetal management. NGF i.e., Norsk gynekologisk forening (Norwegian Gynecological & Obstetrics Association) made this clear to Directorate of Health (Hdir). Included below are excerpts from NDG's 2014 article "NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin."
- "Hdir believes that gestational age should be determined on the basis of ultrasound in week 17-19. By exclusively emphasizing ultrasound at this point, natural biological variation is disregarded. Ultrasound in early pregnancy (where the biological variation is less) carried out by a competent person or where we know exactly when conception has taken place (as in assisted reproduction), shall not be taken into account. We believe this is incorrect in relation to good documented knowledge and international guidelines. It also goes against evidence-based recommendations in the newly completed and revised Guidelines in obstetrics 2014." (Source: "NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin" Bergen, Oslo, Tromsø 03.12.14, Norsk gynekologisk forening, Nyheter, 2014)
- "In Norway two ultrasound methods were developed and used - one primarily designed to determine gestational age, the other to determine date of delivery. We, as academics, are well experienced in clinical practice. Hdir's recommendation is to use a method that solves none of the clinical problems related to abortion, premature birth, growth abnormalities or post-term. There is far more to take into account than the ultrasound method used." (Source: ibid.)
- "Both from a technical and procedural point of view NGF believes that Hdir's handling of this matter is highly reprehensible, does not inspire confidence and unfortunately can be downright dangerous in relation to dealing with difficult clinical problems. NGF will therefore recommend its members to deal with the recommendations given in the Guidelines in obstetrics in 2014 which are based on the best scientific knowledge after a long and thorough process, in which Hdir was also instrumental." (Source: ibid.)
- "Fetal age and EDD always need to be considered in conjunction. In Terminhjulet, the EDD is derived from the age, in eSnurra the age is derived from the date of delivery. Evaluations (7 – 9) show that Terminhjulet’s EDDs are unstable, with a varying bias over the weeks it was developed to cover – pregnancy weeks 13 – 23." (Source: "One Norwegian national tool for estimating date of delivery and fetal age" Torunn Janbu, Head of the Department of Hospital Services, Norwegian Directorate of Health Tidsskr Nor Legeforen nr. 9, 2016; 136: 790 – 1.)
Moreover, it appears Torunn Janbu was not aware Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE) had been formulated by Dr. Hutchon and published, along with a demonstration of the method using a dataset of both CRL and BPD in his seminal Hutchon 1998 and website 7 years and 9 years before NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, in which NCFM eSnurra Group laid claim to Dr. Hutchon's original idea and method as their own original idea and method, thereby engaging in ongoing research misconduct via plagiarism for the last 12-years.
In his seminal Hutchon 1998, Dr. Hutchon explicitly warned against using Population-based Direct EDD Estimation to assess GA and fetal age because Dr. Hutchon understood that the basis for determining fetal age is not the end of the pregnancy, but its beginning and that all available information should be used when assessing fetal age. This is covered in detail elsewhere in this document.
Additionally, Torunn Janbu ignored all the obstetric & fetal medicine experts who had so clearly and explicitly warned of the risks and consequences: "that critical mistakes may follow from the failure to include all available information when fetal age is assessed," as was explained above, but bears repeating.
Directorate of Health completely ignored fact-based evidence of serious data irregularities with respect to the integrity of the BPD data in NCFM eSnurra Group's studies and publications.
- "The Directorate of Health also ignores published criticism of the Trondheim study (4): selection bias before and after weeks 18 – 20 of gestation; unclear exclusion criteria for fetuses with potentially hampered growth; and failing to account for the inclusion of fetuses with an elongated head whose biparietal diameter was adjusted based on the longitudinal axis of the skull." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093) Reference (4): (Source: Re: A direct method for ultrasound prediction of day of delivery:a new, population-based approach. Problems of accounting for a retrospective selection. Kiserud T, Johnsen SL, Rasmussen S., Ultrasound Obstet Gynecol 2008; 31: 22)
The Directorate of Health's comparison of Bergen Group's method (Terminhjulet or Term Wheel) and NCFM eSnurra Group or Trondheim Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) was an insult to:
- the scientific method and basic reasoning,
- Bergen Group,
- Norsk gynekologisk forening,
- Norway's medical professionals,
- Norway's women and their fetuses/babies and
- the public trust
- "When you set up studies with controversial comparisons, you risk misleading everybody --regulatory agencies, physicians and patients 9." (Source: (Source: Bending Science: How special interests corrupt public health research. "Chapter 4. Shaping Science: "The Recipe for Shaping Science" p. 64. Thomas O. McGarity and Wendy E. Wagner. Harvard University Press. Cambridge, Massachusetts, USA. 2008. ISBN: 978-0-674-04714-3. Book Review: The Journal of Clinical Investigation or pdf) Also see: Bending Science
- "We hold the opinion that the comparison conducted by the Trondheim Group suffers from conflicts of interest, but the Directorate of Health appears not to have realized that the comparative evaluation of the two methods really amounts to comparing apples to pears. The Directorate of Health also ignores the criticism raised against the Trondheim study (4): selection bias before and after weeks 18 – 20 of gestation; unclear exclusion criteria for fetuses with potentially hampered growth; and failing to account for the inclusion of fetuses with an elongated head whose biparietal diameter was adjusted based on the longitudinal axis of the skull." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
"the comparative evaluation of the two methods really amounts to comparing apples to pears."
NCFM eSnurra Group's Gjessing et al. 2007: Mission Creep & Mission Leap
The objectives of the NCFM eSnurra Group study, as articulated in Gjessing et al. 2007: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach" (excerpt below) were clearly defined and explicitly stated by the 3 NCFM eSnurra Group authors; the 3 "copyright owners" of NCFM eSnurra (© 2007 EikNes, Grøttum og Gjessing); the 3 NCFM eSnurra Group coauthors of Eik-Nes et al. 2005 and Gjessing et al. 2007 which appropriated Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE), as their own original idea and method from Dr. Hutchon's seminal Hutchon 1998, website and other publications, in NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, thus engaging in research misconduct via plagiarism for the last 12 years. Moreover, NCFM Snurra/eSnurra Group participated in a recognized collaboration, foregoing authorship credits, which resulted in Taipale & Hiilesmaa 2001, which also appropriated and plagiarized the Hutchon Method of PDEE.
Directorate of Health either missed or ignored these important distinctions between direct estimation of fetal age from fetal metric measurements and calculating fetal age and GA from EDD using the equivalent of Naegele's rule, in reverse, from estimates of the remaining days (RE) from the ultrasound exam to birth/delivery date. Clearly:
Incredulously, Dr. Johnson's request to NOKC (Forslagsnr: 2015_005) with Bergen Group's Johnsen et al. 2008 attached were ignored by NOKC and Directorate of Health, which begs the question: How was it possible for NOKC to ignore the caliber of research, scholarship, experience and evidence presented in Dr. Johnson's request which included that which was presented in Bergen Group's Johnsen et al. 2008? The answer is both simple and obvious. At the time, NOKC formally reported to Directorate of Health. And, as is made perfectly clear below, NOKC had been directly and specifically "instructed in professional matters" by Directorate of Health via their request to NOKC (Forslagsnr: 792, 15.11.2013) a.k.a. "the fix" regarding what they wanted and needed from NOKC to effect their knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive NCFM eSnurra Group's "method" (i.e., the plagiarized, intentionally misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine.
"The Fix"
Not coincidentally, the term "the fix" is a euphemism for that which is effected by those who are "instructed in professional matters." Notice the word "instructed" is a euphemism. The nesting of euphemisms is also no coincidence, as this is the vernacular of the modus operandi known as "the fix."
Directorate of Health's Request to NOKC a.k.a. "The Fix"
Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, delivered Økland's 2012 NTNU dr.philos. Thesis and 3 NCFM eSnurra Group papers via 2 separate statements and references in their request to NOKC (Forslagsnr: 792, 15.11.2013) on behalf of Ministry of Health & Care Services and Directorate of Health. Grøgaard already knew NCFM eSnurra Group member (and current Directorate of Health employee)Inger Økland's 2012 NTNU dr.philos. Thesis concluded in favor of NCFM eSnurra Group's method (i.e., the plagiarized intentionally misused Hutchon Method of PDEE) because Grøgaard had been a member of Økland's 2012 NTNU dr.philos. Thesis Assessment Committee, and Grøgaard had adjudicated Økland's 2012 NTNU dr.philos. Thesis' public defense on 13.01.2012. The excerpt below, just 1 sentence, within Directorate of Health's formal request to NOKC was (and remains) "the fix." Everything else in Directorate of Health's request to NOKC was cover and packaging for "the fix," evidenced in NOKC's official reply or answer. (See Merriam-Webster: the fix is in; See Wictionary: the fix is in)
Directorate of Health's Official Request to NOKC
Included below is the electronically filed request made to the Norwegian Knowledge Centre for the Health Services (kunnskapssenteret) (NOKC) by Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, on behalf of the Norwegian Ministry of Health & Care Services and Norwegian Directorate of Health. Some of the text has been color-coded to assist the reader in context tracking and analysis of the issues of: gestational age (GA) & estimated date of delivery (EDD or term) and the issues of pregnancy & abortion. A quick look at the Issues Table below identifies Gestational Age and Pregnancy as the overwhelming, dominant issues, i.e., at least numerically.
The objectives of the NCFM eSnurra Group study, as articulated in Gjessing et al. 2007: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach" (excerpt below) were clearly defined and explicitly stated by the 3 NCFM eSnurra Group authors; the 3 "copyright owners" of NCFM eSnurra (© 2007 EikNes, Grøttum og Gjessing); the 3 NCFM eSnurra Group coauthors of Eik-Nes et al. 2005 and Gjessing et al. 2007 which appropriated Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE), as their own original idea and method from Dr. Hutchon's seminal Hutchon 1998, website and other publications, in NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, thus engaging in research misconduct via plagiarism for the last 12 years. Moreover, NCFM Snurra/eSnurra Group participated in a recognized collaboration, foregoing authorship credits, which resulted in Taipale & Hiilesmaa 2001, which also appropriated and plagiarized the Hutchon Method of PDEE.
- "Objectives To introduce a direct population-based method for prediction of term based on ultrasound measurements of the biparietal diameter and femur length in the second trimester of pregnancy" (Source: "A direct method for ultrasound Prediction of day of delivery: a new, population-based approach, H. K. Gjessing, P. Grøttum, S. H. Eik-Nes, Ultrasound Obstet Gynecol 2007; 30: 19–27. p.19)
- "... the aim of this study was to develop a method for estimating expected day of delivery and gestational age based on a large population" (Source: ibid., p. 20).
- "It is interesting to note that the approach also provides estimates for gestational age at the time of the ultrasound examination." (Source: ibid., p. 26)
- gestational age data collected for use as a dependent variable or as any other type of variable,
- gestational age determination resulting from local linear quantile regressions or other parametric or non-parametric statistical techniques in their "Statistical methods" section (Source: ibid., p. 20)
Directorate of Health either missed or ignored these important distinctions between direct estimation of fetal age from fetal metric measurements and calculating fetal age and GA from EDD using the equivalent of Naegele's rule, in reverse, from estimates of the remaining days (RE) from the ultrasound exam to birth/delivery date. Clearly:
- " the basis for determining gestational age is not the end of the pregnancy, but its beginning." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- Background and justification for the proposal: "In pregnancy care, the gestational age is the reference point in order to follow and assess the development of pregnancy, and it is particularly important in risk pregnancies which are followed by close monitoring and growth controls. Proper gestational age is essential for proper clinical decisions, in the most difficult cases, this may be life or death. The Knowledge Center earlier this year made an assessment of "Methods for Estimating Pregnancy Length and Term", and then chose to focus on the ability of two Norwegian models to predict the term. In clinical practice, calculated term has little significance since only about 4% of pregnant women give birth on this date and the biological variation associated with pregnancy length at birth is high (the term concept covers a five-week period from weeks 37-42). What is important clinically is that the gestational age determination of pregnancy is as accurate as possible and reflects as much as possible the biological age of the fetus. The Directorate of Health has, among other things, based on the Knowledge Center's assessment recommending that in Norway "eSnurra" be used to determine the duration of pregnancy and term, and their recommendation can also be interpreted as all dating should take place at the routine ultrasound exam in weeks 17-19. This is problematic in several ways, primarily because we believe that age determination performed earlier in pregnancy is more precise because of less biological variation related to the size of the fetus. Today, approx. 50-60% of pregnant women have an ultrasound exam prior to the routine 18-week ultrasound exam either as part of a fetal diagnostic examination or clinical indication (bleeding, pain, multilateral risk assessment) and many of us believe it is wrong later in pregnancy, based on the growth of the fetus, to change the age determined by an early examination. There is also a group of pregnant women for whom the time of conception is known (e.g., pregnancy occurred after in vitro fertilization), and it is also not correct to change the age due to the fetus' growth in pregnancy. It is also not clear that it is correct that a reference set designed to predict term based on a study that does not document gestational age, should be used to determine gestational age. Since age determination in pregnancy affects so many (60,000 pregnant women in Norway per year), is so crucial in clinical decisions and was not considered separately in the order "Methods for estimating pregnancy length and term", we request that the Knowledge Center conduct a new assessment focusing on age determination in pregnancy instead of on term prediction." (Source: "Age Determination of Pregnancy" Synnøve Lian Johnsen, 01.11.2014 Request to NOKC (Forslagsnr: 2015_005, 01.11.2014))
- Intervention / measures to be assessed: "Assess the accuracy of age determination based on ultrasound in the first trimester compared to the second trimester. Evaluate gestational age determination with known time of conception. Evaluate "eSnurra's" fitness and precision of gestational age determination in the first and second trimester. Assess the fitness and precision of gestational age determination based on the reference set from Bergen Group's study." (Source: "Age Determination of Pregnancy" Synnøve Lian Johnsen, Request to NOKC (Forslagsnr: 2015_005, 01.11.2014))
- ABSTRACT
Background Conventionally, the pregnancy duration is accepted to be 280–282 days. Fetuses determined by ultrasound biometry to be small in early pregnancy, have an increased risk of premature birth. We speculate that the higher rate of preterm delivery in such small fetuses represents a pathological outcome not applicable to physiological pregnancies. Here we test the hypothesis that in low-risk pregnancies fetal growth (expressed by fetal size in the second trimester) is itself a determinant for pregnancy duration with the slower growing fetuses having a longer pregnancy.
Methods We analysed duration of gestation data for 541 women who had a spontaneous delivery having previously been recruited to a cross-sectional study of 650 low-risk pregnancies. All had a regular menses and a known date of their last menstrual period (LMP). Subjects were examined using ultrasound to determine fetal head circumference (HC), abdominal circumference (AC) and femur length (FL) at 10–24 weeks of gestation. Length of the pregnancy was calculated from LMP, and birth weights were noted. The effect of fetal size at 10–24 weeks of gestation on pregnancy duration was assessed also when adjusting for the difference between LMP and ultrasound based fetal age.
Results Small fetuses (z-score -2.5) at second trimester ultrasound scan had lower birth weights (p < 0.0001) and longer duration of pregnancy (p < 0.0001) than large fetuses (z-score +2.5): 289.6 days (95%CI 288.0 to 291.1) vs. 276.1 (95%CI 273.6 to 278.4) for HC, 289.0 days (95%CI 287.4 to 290.6) vs. 276.9 days (95%CI 274.4 to 279.2) for AC and 288.3 vs. 277.9 days (95%CI 275.6 to 280.1) for FL. Controlling for the difference between LMP and ultrasound dating (using HC measurement), the effect of fetal size on pregnancy length was reduced to half but was still present for AC and FL (comparing z-score -2.5 with +2.5, 286.6 vs. 280.2 days, p = 0.004, and 286.0 vs. 280.9, p = 0.008, respectively).
Conclusion Fetal size in the second trimester is a determinant of birth weight and pregnancy duration, small fetuses having lower birth weights and longer pregnancies (up to 13 days compared with large fetuses). Our results support a concept of individually assigned pregnancy duration according to growth rates rather than imposing a standard of 280–282 days on all pregnancies. (Source: Fetal size in the second trimester is associated with the duration of pregnancy, small fetuses having longer pregnancies Synnøve L Johnsen, Tom Wilsgaard, Svein Rasmussen, Mark A Hanson, Keith M Godfrey and Torvid Kiserud, BMC Pregnancy and Childbirth 2008 8:25 DOI: 10.1186/1471-2393-8-25)
- "Among natural conceptions where the date of conception (ovulation) is known, the variation in pregnancy length spanned 37 days, even after excluding women with complications or preterm births." (Source: "Length of human pregnancy and contributors to its natural variation" A.M. Jukic, D.D. Baird, C.R. Weinberg, D.R. McConnaughey, A.J. Wilcox, Hum Reprod (2013) 28 (10): 2848-2855. DOI: https://doi.org/10.1093/humrep/det297, Published: 06 August 2013)
Incredulously, Dr. Johnson's request to NOKC (Forslagsnr: 2015_005) with Bergen Group's Johnsen et al. 2008 attached were ignored by NOKC and Directorate of Health, which begs the question: How was it possible for NOKC to ignore the caliber of research, scholarship, experience and evidence presented in Dr. Johnson's request which included that which was presented in Bergen Group's Johnsen et al. 2008? The answer is both simple and obvious. At the time, NOKC formally reported to Directorate of Health. And, as is made perfectly clear below, NOKC had been directly and specifically "instructed in professional matters" by Directorate of Health via their request to NOKC (Forslagsnr: 792, 15.11.2013) a.k.a. "the fix" regarding what they wanted and needed from NOKC to effect their knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive NCFM eSnurra Group's "method" (i.e., the plagiarized, intentionally misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine.
"The Fix"
Not coincidentally, the term "the fix" is a euphemism for that which is effected by those who are "instructed in professional matters." Notice the word "instructed" is a euphemism. The nesting of euphemisms is also no coincidence, as this is the vernacular of the modus operandi known as "the fix."
- "The National Knowledge Center for Health Services provides and disseminates knowledge of the effects of methods, means and measures and of quality in all parts of the health service. The goal is to make good decisions so that users get the best possible healthcare. The center is formally a governing body under the Directorate of Health, without governmental functions. The Knowledge Center can not be instructed in professional matters."
Norwegian: (Nasjonalt kunnskapssenter for helsetjenesten fremskaffer og formidler kunnskap om effekt av metoder, virkemidler og tiltak og om kvalitet innen alle deler av helsetjenesten. Målet er å bidra til gode beslutninger slik at brukerne får best mulige helsetjenester. Senteret er formelt et forvaltningsorgan under Helsedirektoratet, uten myndighetsfunksjoner. Kunnskapssenteret kan ikke instrueres i faglige spørsmål.) (Source: "Utprøving av mini-HTA i Helse Vest RHF, Notat fra Kunnskapssenteret april 2011" Notat: ISBN 978-82-8121-404-0; april 2011. Nasjonalt kunnskapssenter for helsetjenesten.
Directorate of Health's Request to NOKC a.k.a. "The Fix"
Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, delivered Økland's 2012 NTNU dr.philos. Thesis and 3 NCFM eSnurra Group papers via 2 separate statements and references in their request to NOKC (Forslagsnr: 792, 15.11.2013) on behalf of Ministry of Health & Care Services and Directorate of Health. Grøgaard already knew NCFM eSnurra Group member (and current Directorate of Health employee)Inger Økland's 2012 NTNU dr.philos. Thesis concluded in favor of NCFM eSnurra Group's method (i.e., the plagiarized intentionally misused Hutchon Method of PDEE) because Grøgaard had been a member of Økland's 2012 NTNU dr.philos. Thesis Assessment Committee, and Grøgaard had adjudicated Økland's 2012 NTNU dr.philos. Thesis' public defense on 13.01.2012. The excerpt below, just 1 sentence, within Directorate of Health's formal request to NOKC was (and remains) "the fix." Everything else in Directorate of Health's request to NOKC was cover and packaging for "the fix," evidenced in NOKC's official reply or answer. (See Merriam-Webster: the fix is in; See Wictionary: the fix is in)
- "In a recently published doctorate in 2012 (Inger Økland, SUS) compared both methods. Can KS issue a statement about which method is considered to be the best science and that can be the basis for selecting the method for health authorities?" (Source: Forslagsnr: 792, 15.11.2013) [Note: "KS" is an abbreviation for Knowledge Center/Senter]
- References included in Directorate of Health's official request to NOKC
References: 1. bias of traditional term prediction models: results from different sample based models evaluated on 41,343 ultrasound examinations. Ultrasound Obstet Gynecol 2010; 36: 728-734. 2. A new population-based term prediction model vs. two traditional sample based models: validation on 9046 ultrasound examinations. Ultrasound Obstet Gynecol 2011; 37: 207-213. 3. Advantages of the population-based approach, two pregnancy dating Demonstrated with results from 23,020 ultrasound examinations Ultrasound Obstet Gynecol 2011. DOI: 10.1002 / uog.10081. 4. Bias in second-trimester ultrasound dating related to prediction models and fetal measurements. Thesis 2012 NTNU Inger Økland main challenge is: an evaluation of the two methods used in Norway today and an overview of the most commonly used methods in Western Europe, how they are validated and how they are in relation to our two Norwegian methods?"
- Jørg Kessler, MD, PhD: "The author has completed the ICMJE form and reports the following conflict of interest: He is a member of the research group that published the fetal biometry reference tables referred to in this article."
- Torvid Kiserud, MD, PhD: "The author has completed the ICMJE form and reports the following conflict of interest: He has developed an alternative method to the eSnurra obstetrics wheel, which is currently being recommended by Norwegian health authorities."
- Dr. Stuart Campbell, London, U.K., Campbell 1969: Campbell Method of Estimation of Gestational Age, implemented by the Bergen Group as Terminhjulet or Term wheel
- Dr. David J. R. Hutchon, Darlington, U.K., Hutchon 1998: Hutchon Method of Population-based Direct EDD Estimation (PDEE), implemented via appropriation & plagiarism by NCFM eSnurra Group as NCFM eSnurra or eSnurra
See: Intro & more > GA & EDD METHODS
- NCFM eSnurra Group references identified to NOKC by Directorate of Health as the designated means for "the fix."
References: 1. bias of traditional term prediction models: results from different sample based models evaluated on 41,343 ultrasound examinations. Ultrasound Obstet Gynecol 2010; 36: 728-734. 2. A new population-based term prediction model vs. two traditional sample based models: validation on 9046 ultrasound examinations. Ultrasound Obstet Gynecol 2011; 37: 207-213. 3. Advantages of the population-based approach, two pregnancy dating Demonstrated with results from 23,020 ultrasound examinations Ultrasound Obstet Gynecol 2011. DOI: 10.1002 / uog.10081. 4. Bias in second-trimester ultrasound dating related to prediction models and fetal measurements. Thesis 2012 NTNU Inger Økland main challenge is: an evaluation of the two methods used in Norway today and an overview of the most commonly used methods in Western Europe, how they are validated and how they are in relation to our two Norwegian methods?"
Directorate of Health's Official Request to NOKC
Included below is the electronically filed request made to the Norwegian Knowledge Centre for the Health Services (kunnskapssenteret) (NOKC) by Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, on behalf of the Norwegian Ministry of Health & Care Services and Norwegian Directorate of Health. Some of the text has been color-coded to assist the reader in context tracking and analysis of the issues of: gestational age (GA) & estimated date of delivery (EDD or term) and the issues of pregnancy & abortion. A quick look at the Issues Table below identifies Gestational Age and Pregnancy as the overwhelming, dominant issues, i.e., at least numerically.
- Issues Table
Issue Count Percent
Gestational Age (GA) 24 86%
Term (EDD) 4 14%
Total 28 100%
Pregnancy 20 74%
Abortion 7 26%
Total 27 100%
Additionally, the purple text in Directorate of Health's formal request to NOKC (below) identifies specific instances where Grøgaard & Sommerstad directed NOCK to deliver the answer Directorate of Health wanted, needed and expected. In fact, Grøgaard & Sommerstad provided the answer to NOKC and directed NOKC to deliver the provided answer (i.e., "the fix") back to Directorate of Health as NOKC's official answer. The Issue Table does not include issues located within these purple text sections. To be specific, "the fix" is in purple, underlined, text. NOKC's online request form's fields & questions are presented in black bold text.
- Request to NOKC (Forslagsnr: 792, 15.11.2013) on behalf of Directorate of Health and Ministry of Health & Care Services
Forslagsnr: 792
received: 15.11.2013
Contact: Jens Grøgaard, Cecilie Sommerstad
Title (max 100 characters): Assessment of the most accurate and research-based tools of pregnancy duration and term.
Background and reasons for the proposal: Directorate of Health has been commissioned by the Ministry of Health to clarify which method is most accurate and research-based assessment for pregnancy duration. Ministry of Health refers to the report Independent expert for assessment of abortions which was submitted on 8 April 2013. Norway has today two different ultrasound methods that underlie the assessment of pregnancy duration; Forward wheel and new e-snurra. Both methods are research-based and developed respectively at UiB and NTNU. Internationally, both methods well recognized and used in several countries. It is desirable that services for pregnant women are equal so pregnancy duration is evaluated with the same method nationally. Today the various methods are causing discrimination in border areas for late abortions, post-term pregnancies and lower limits of extreme prematurity (intensive care or not).
Issues (possibly with precise questions):
There is currently a disagreement in professional circles in Norway in terms of how pregnancy duration is to be determined. It used different methods / tools that have different margins of error when calculating the exact number of weeks / days of a pregnancy. We want the Knowledge Centre to collect research that exists on the subject of calculation of pregnancy duration. We want an overview of the most commonly used methods in Western Europe, how they are validated and how they are in relation to our two Norwegian methods. We need evidence of the / the method (s) at any time of pregnancy provides the least uncertainty and "wiggle room" on the number of days when the duration of pregnancy is calculated. In a recently published doctorate degree in 2012 (Inger Økland, SUS) compared both methods. Can KS issue a statement about which method is considered to be the best science and that can be the basis for selecting the method for health authorities?
Further description of the patient population / area that the measure is aimed at, for example."Overweight Children" or "patients with first myocardial infarction": The choice of ultrasound method for determination of pregnancy length and term applies to around 60,000 pregnant women annually in Norway. The goal is equitable services across the country so that the four following conditions are not treated differently in the country. The following states are affected by various methods for pregnancy length and term: - Absolute upper limit for late abortion is legal to 21 weeks + 6 days. - National guidance for post-term pregnancy has fixed limits for added control and induction of labor. - Lower limit for intensive care of extremely premature infants should be equal nationally. - The upper limit for prematurity 36 weeks + 6 days and not premature baby 37 weeks.
Intervention / actions to be considered, for example."Training" or "percutaneous coronary intervention (PCI)": Term wheel and new e-snurra
Alternative measures, appropriate. Compared with, for example."Advice on diet" or "thrombolysis" or "no intervention": various ultrasonic methods that underlie the assessment of gestation
Endpoints / outcomes, i.e. what we want to measure the impact of the measure on, for example."Weight development", "survival" or "quality of life": proper assessment of pregnancy duration
General criteria::
State of seriousness
Expected benefit for patient and society
Includes many patients
Professional disagreement / variation in practice
Uncertain effect
General interest
Impact on resource use
International commitment
What product should be used, how the findings will be followed up. Study can lead to changes in Norwegian practice ?: What product should be used, how will the findings be followed up? Can the investigation method change Norwegian practice? The knowledge summary will be used to revise the Handbook on abortion work, and to ensure that health authorities who handle abortion cases use the same tool for estimating gestational age. This is significant when there is an application for abortion. By using various calculation methods of the various health authorities will be a risk that women in Norway do not get equal opportunities. The product could be the basis for recommendations in revised guidelines for pregnancy monitoring. Furthermore, the national statistics for births in Norway, MFR, was more consistent and accurate with regard to delimitation of late abortions, the lower limit of extreme prematurity, the upper limit of prematurity and post-term pregnancies.
What is (if any) already done. Is it part of a major assignment, must the assignment be coordinated ?:
When must it be done, clear definition of meeting points and deadlines with justification:
Other comments / explanations / questions: Other comments: Knowledge Centre in 2010 delivered a preliminary report on post-term pregnancies. This report has an overview of the knowledge base for overtime issue until 2010. References: 1. bias of traditional term prediction models: results from different sample based models evaluated on 41,343 ultrasound examinations. Ultrasound Obstet Gynecol 2010; 36: 728-734. 2. A new population-based term prediction model vs. two traditional sample based models: validation on 9046 ultrasound examinations. Ultrasound Obstet Gynecol 2011; 37: 207-213. 3. Advantages of the population-based approach, two pregnancy dating demonstrated with results from 23,020 ultrasound examinations Ultrasound Obstet Gynecol 2011. DOI: 10.1002 / uog.10081. 4. Bias in second-trimester ultrasound dating related to prediction models and fetal measurements. Thesis 2012 NTNU Inger Økland main challenge is: an evaluation of the two methods used in Norway today and an overview of the most commonly used methods in Western Europe, how they are validated and how they are in relation to our two Norwegian methods? (Perhaps report from 2010 gives something there?) One important point is different methodologies ability to determine duration of pregnancy at any time of pregnancy, not just determination of the term as well was the central issue in 2010.
File attachments 1: Booking the Knowledge Centre ( Best term and svskapslengde) .docx
(http://www.kunnskapssenteret.no/186868/vurdering-av-det-mest-presise-og-forskningsbaserte-verktoy-forsvangerskapets-varighet-og-termin)
[Note 1: This URL is included for completeness. It redirects to Norwegian Institute of Public Health (NIPH) without returning the requested page/file.]
[Note 2: The reference made via: "Knowledge Centre in 2010 delivered a preliminary report on post-term pregnancies" is as follows: "Effekten av induksjon av fødsel etter termin for forebygging av død, komplikasjoner og overtidighet i sangerskapet"]
(Source: Knowledge Centre for Health Services in Public Health, Assessment of the most accurate and research-based tools of gestation and term, Jens Grøgaard, Cecilie Sommerstad, Forslagsnr: 792, 15.11.2013) (Note: The source is in Norwegian; the English translation is via Google Translate with edits.)
NOKC's Official Reply to Directorate of Health's 15.11.2013 Request
Included below is NOKC's official reply to Directorate of Health's official request made on behalf of Ministry of Health & Care Services and Directorate of Health by Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health. NOKC's official reply cited 5 references: 1 Bergen Group publication from the Bergen Group's trilogy regarding femur length (FL) and 4 NCFM eSnurra Group publications (presented in red text) of which all 4 publications had appropriated and plagiarized the Hutchon Method of Population-based Direct EDD Estimation (PDEE) as part of NCFM eSnurra Group's 12 years of ongoing research misconduct via plagiarism. A link has been appended to each of the 5 references for, wait for it... easy reference.
NOKC's References
If NOKC had included Bergen Group's Johnsen et al. 2004, i.e., fetal head biometery (HC & BPD) and gestational age) in with Johnsen et al. 2005 (femur length (FL) and gestational age with FL and fetal head ratios) in their assessment, there would have been a chance the problematic, unreliable BPD measurement would have been included as a discussion point in NOKC's "comprehensive assessment" ("helhetsvurdering"). Bergen Group's Terminhjulet or Term wheel relied/relies on the more robust fetal head circumference (HC) measurement, with the BPD measurement used as a cross-check and to assess fetal head shape when appropriate. Bergen Group's Terminhjulet or Term wheel uses HC & BPD to directly estimate gestational age and, therefrom, calculate EDD using the equivalent of Naegele's rule. (See: Warnings > BPD PROBLEMATIC) That said, comparing NCFM eSnurra Group's method (i.e., the appropriated, plagiarized Hutchon Method of PDEE) with the Bergen Group's Terminhjulet or Term wheel "really amounts to comparing apples to pears," as was stated by Bergen Group in conjunction with the problematic BPD with respect to NCFM eSnurra Group's unexplained BPD-based inclusions, exclusions and BPD measurement adjustments criteria and methods in their Gjessing et al. 2007 study.
NOKC & Evidence-informed Health Policy Using Research
Interestingly, in a 2008 study Norwegian Knowledge Centre for the Health Services (NOKC) explicitly stated: 1) NOKC's purpose with respect to "Evidence-informed Health Policy Using Research" and 2) NOKC's supposed scientific and professional independence from Directorate of Health. [Note: In January of 2016, NOKC separated from Directorate of Health and joined the Norwegian Institute of Public Health (NIPH).] It would appear NOKC's 2008 study was ignored with respect to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation.
NOKC's Knowledge delivery (or knowledge provisioning) in response to the official request (Forslagsnr: 792, 15.11.2013) made by Directorate of Health and Ministry of Health and Care Services was inadequate or nonexistent on multiple levels. A 2016 Norwegian study, Malterud et al. 2016, examined NOKC's process with the following results:
Corrupted Process: Torunn Janbu of Directorate of Health
In the excerpt below, Torunn Janbu, dr.med. (MD, PhD), Head of the Department of Hospital Services, Norwegian Directorate of Health, falsely stated it was NOKC who had "pointed out" the "validation strategy" (i.e, Økland's 2012 NTNU dr.philos. Thesis, "the fix").
Corrupted Process: The Directorate of Health's Letter
Jens Grøgaard, Senior Adviser, Directorate of Health signed the Directorate's 10.12.2014 letter with Torunn Janbu, then Acting Division Director, Directorate of Health; a letter which was distributed to Helse Midt-Norge RHF, Helse Nord RHF, Helse Sør-Øst RHF and Helse Vest RHF to enact Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care. In this letter Økland's 2012 NTNU dr.philos. Thesis (not a PhD as degree as Torunn Janbu would have people believe) was the one and only document discussed, cited and footnoted in Directorate's 10.12.2014 letter; and, it was the one and only document presented as independent, academic justification for Directorate of Health's selection of NCFM eSnurra Group's eSnurra "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) as the exclusive implementation vehicle of Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation. At no time did Torunn Janbu or anyone else from Directorate of Health disclose:
Jens Grøgaard: Breech of Medical Ethics: NMA Ethics Council
In 2012, Jens Grøgaard coauthored a report titled "Age estimation in youths and young adults" as part of a Norwegian Directorate of Immigration (UDI) commissioned and since-completed study; a study managed by Norwegian Computing Center (Norsk Regnesentral) titled: 'Development of improved methods or basis for medical age assessments of minors and young adults," which listed BarneSak AS, Jens B. Grøgaard's company, as a Project Partner as follows:
Medical Ethics: Cost & Benefit Analysis
Jens Grøgaard's company, BarneSak AS (Org No. 912283224) was founded in 2013 and reported operating profits (in 1,000 NOK) of: 1,290, 3,831 & 3, 627 in 2014, 2015 & 2016, respectively, for a cumulative reported operating profit of 8,748 NOK (in 1,000 NOK) or 8,748,000 NOK. For U.S. readers, that was a little more than $1 million. Ergo, the cost-benefit analysis is straightforward: Cost = ethical criticism amounting to a wrist slap; Benefit = $1,000,000 USD or 8,748,000 NOK, which may only serve to quantify a key economic distinction between Doctors with Borders and Doctors Without Borders.
An 04.01.2016 article in VG NYHETER titled "Uses millions for controversial age tests" ("Bruker millioner på omstridte alderstester") identified the process, some of the participants and some of the costs (below) as well as the full story.
A 2017 University of Oslo Masters Thesis by Aisha Munir titled "Age examination of single minor asylum seekers" ("Aldersundersøkelse av enslige mindreårige asylsøkere") provides a
In a 05.03.2018 article in Tidsskrift for Den norske legeforening, the ethical issues of age assessment of young asylum seekers were discussed with respect to medical harm and prior, informed, voluntary consent of dubious age assessment methods which use harmful ionizing radiation (x-rays) for no medical benefit. (Source: "While we are waiting for a new method for the age determination of young asylum seekers" Norwegian: "Mens vi venter på en ny metode for aldersbestemmelse av unge asylsøkere" SVEIN AARSETH, STINE KATHRIN TØNSAKER. Publisert: 5. mars 2018, Utgave 5, 6. mars 2018. Tidsskr Nor Legeforen 2018. DOI: 10.4045/tidsskr.17.0960. Mottatt 5.11.2017, første revisjon innsendt 10.12.2017, godkjent 25.1.2018.)
Grøgaard's Breaches of Medical Ethics
Included below are 2 excerpts from the article "Criticism to the doctor for age testing" ("Kritikk til lege for alderstesting") by Tove Myrbakk, Nordland legeforening, Den Norske Legeforening 12. desember 2016, which articulates Jens Grøgaard's breaches of medical ethics and the associated criticisms delivered by the Medical Ethics Council of the Norwegian Medical Association.
Included below are the relevant sections and paragraphs of the Code of Ethics for Doctors which Grøgaard breached, as published by Den norske legeforening "Code of Ethics for Doctors - Adopted by the Representative Body in 1961 and subsequently amended, most recently in 2015."
While profiting, handsomely, from BarneSak AS, Grøgaard made a lateral expansion into a new market where he could leverage the same strategy but with one, 180-degree twist. He used his knowledge and experience from establishing an exclusive provider of medically & ethically flawed evidence-manufactured medicine (i.e., dubious x-ray-based "official certification" of medical age) for Norwegian Directorate of Immigration (UDI) to establishing an exclusive provider of evidence-obviated medicine for Norwegian Directorate of Health's knowledge-obviated, medially & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care. All without securing a pregnant woman's prior, informed, voluntary, explicit consent; thereby, placing control of all age-related pregnancy and abortion decisions under the control of Directorate of Health with their exclusive NCFM eSnurra Group implementation; an implementation for which 3 NCFM eSnurra Group members Sturla H. Eik-Nes, Per Grøttum and Håkon K. Gjessing claim to be the "copyright owners," (© 2007 EikNes, Grøttum og Gjessing), as stated on the NCFM eSnura website, of which It would appear Jens Grøgaard, Senior Adviser, Directorate of Health, was able to make his lateral expansion into the market of establishing estimated date of delivery (EDD), gestational age (GA) and fetal age for all pregnancies and abortions in Norway, effortlessly, because Jens Grøgaard was neither burdened nor conflicted by his knowledge of the fact that what he was doing was medically & ethically flawed and willfully negligent.
Included below is NOKC's official reply to Directorate of Health's official request made on behalf of Ministry of Health & Care Services and Directorate of Health by Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health. NOKC's official reply cited 5 references: 1 Bergen Group publication from the Bergen Group's trilogy regarding femur length (FL) and 4 NCFM eSnurra Group publications (presented in red text) of which all 4 publications had appropriated and plagiarized the Hutchon Method of Population-based Direct EDD Estimation (PDEE) as part of NCFM eSnurra Group's 12 years of ongoing research misconduct via plagiarism. A link has been appended to each of the 5 references for, wait for it... easy reference.
- NOKC's Official Reply to Directorate of Health's Official Request
Memo To: Health Directorate by Cecilie Sommerstad and Jens Grøgaard
Cc: Torunn Janbu, Postmottak Directorate of Health
Date: 2nd July 2014
Case number: Booking 792, 14/00171
From: Knowledge Center Senior Lecturer: Kjetil Gundro Bruberg Sign .: [Enter Here]
Contact: Liv Merete Reinar, Gro Jamtvedt Sign .: [Enter here]
Method to estimate gestational age and term
Metoder for å estimere svangerskapslengde og termin
Background
Gestational age and term currently have direct implications for the definition of absolute upper limit for late abortion (21 weeks + 6 days), lower limit for intensive care of premature birth, upper limit for prematurity and premature pregnancy. In Norway, term is predicted on the basis of routine ultrasound exams in weeks 17 to 19. Two different ultrasound-based methods are used, respectively, the "term wheel" (1) and "esnurra" (2), and the two methods are based on different prediction models that do not provide identical result (3).
BakgrunnSvangerskapslengde og termin har i dag direkte implikasjoner for definisjonen av absolutt øvre grense for senabort (21 uker + 6 dager), nedre grense for intensivbehandling av ekstremt prematurfødte, øvre grense for prematuritet og overtidige svangerskap. I Norge predikeres termin på bakgrunn av rutinemessige ultralydundersøkelser i uke 17 til 19. To ulike ultralydbaserte metoder er i bruk, henholdsvis «terminhjulet» (1) og «esnurra» (2), og de to metodene baserer seg på ulike prediksjonsmodeller som ikke gir identisk resultat (3).
To ensure equality across areas and regions, the health authorities want to define which methods and prediction models to be used to determine the gestational age and the term in Norway. This is the reason why the Knowledge Center received an order from the Directorate of Health in November 2013, where the Knowledge Center was asked to evaluate the precision of different tools for determining the gestational age and the term.
For å sikre likhet på tvers av landsdeler og regioner, ønsker helsemyndighetene å definere hvilke metoder og prediksjonsmodeller som skal ligge til grunn for fastsettelse av svangerskapslengde og termin i Norge. Dette er bakgrunnen for at Kunnskapssenteret i november 2013 mottok en bestilling fra Helsedirektoratet der Kunnskapssenteret ble bedt om å vurdere presisjonen til ulike verktøy for å bestemme svangerskapslengde og termin.
Rating of the booking
The primary objective of the Directorate's order is to obtain comparative data for the diagnostic accuracy of the "terminhjulet" versus "esnurra", which means the ability to predict the right term and the ability to provide correct measurements throughout the current measurement window. Traditional diagnostic validation studies require access to an unconventional reference standard for calculation of sensitivity and specificity, etc., but for term estimation there is no reference standard. It is natural to compare the predicted term with the actual date of birth, but since birth is premature and overtime, the date of birth is not a reference standard in the traditional sense. In the absence of the reference standard, other ways to validate the different prediction models must be found.
Vurdering av bestillingen
Den primære målsetningen med bestillingen fra Helsedirektoratet er å innhente sammenligningsdata for den diagnostiske treffsikkerheten til «terminhjulet» versus «esnurra», det vil her si evnen til å predikere rett termin og evnen til å gi riktige målinger over hele det aktuelle målevinduet. Tradisjonelle diagnostiske valideringsstudier krever tilgang til en omforent referansestandard for beregning av sensitivitet og spesifisitet m.m., men for terminfastsettelse finnes det ingen referansestandard. Det er naturlig å sammenligne predikert termin med faktisk fødselsdato, men siden barn fødes både prematurt og overtidig er ikke fødselsdato en referansestandard i tradisjonell forstand. I fravær av referansestandard må man finne andre måter å validere de ulike prediksjonsmodellene på.
One possible solution is to compare different prediction models within the framework of controlled studies or time series analyzes to see whether choice of prediction model affects measurable outcomes. It is possible to conduct a systematic search for such studies, but it is unlikely that such a search will lead to relevant findings.
Én mulig løsning er å sammenligne ulike prediksjonsmodeller innenfor rammene av kontrollerte studier eller tidsserieanalyser for å se om valg av prediksjonsmodell påvirker målbare utfall. Det er mulig å gjennomføre et systematisk søk etter slike studier, men det er lite trolig at et slikt søk vil lede til relevante funn.
Another validation strategy goes through studies where the properties of current methods are compared directly through measurements in the same population. In her doctoral dissertation from 2012 (4), Inger Økland conducted validation studies of three different prediction models ("snurra", "term wheel" and "esnurra"), a work that provides a good basis for assessing actual differences between different prediction models that are relevant in Norwegian context. Interesting projects are underway, among other things, new reference curves for symfyse fundus measurements (5) have been created that are calibrated for use in Norway with "esnurra". Preliminary searches do not indicate, however, that after 2012, validation studies have been published, where "term wheel" and "esnurra" are directly compared.
En annen valideringsstrategi går via studier der egenskapene til aktuelle metoder sammenlignes direkte gjennom målinger i samme populasjon. I sin doktorgradsavhandling fra 2012 (4) gjennomførte Inger Økland valideringsstudier av tre ulike prediksjonsmodeller («snurra», «terminhjulet» og «esnurra»), et arbeid som gir godt grunnlag for å vurdere faktiske forskjeller mellom ulike som prediksjonsmodeller som er relevante i norsk sammenheng. Interessante prosjekter er i gang, blant annet er det laget nye referansekurver for symfyse-fundusmål (5) som er kalibrert for bruk i Norge med «esnurra». Foreløpige søk tyder imidlertid ikke på at det, etter 2012, er publisert valideringsstudier der «terminhjulet» og «esnurra» sammenlignes direkte.
Conclusion
After an overall assessment, it seems unlikely that a systematic overview carried out in accordance with the Knowledge Center's method handbook will help to highlight the problem beyond what is already known. When the Directorate of Health determines which prediction model should be used to estimate the pregnancy length and term, it seems reasonable to base the decision on the findings presented in Inger Økland's doctoral thesis (4).
Konklusjon
Etter en helhetsvurdering virker det lite sannsynlig at en systematisk oversikt gjennomført i tråd med Kunnskapssenterets metodehåndbok vil bidra til å belyse problemstillingen utover det som allerede er kjent. Når Helsedirektoratet skal beslutte hvilken prediksjonsmodell som bør benyttes for å estimere svangerskapslengde og termin virker det følgelig rimelig å basere avgjørelsen på funnene som er presentert i Inger Øklands doktorgradsavhandling (4).
References
Referanser
1. Johnsen SL. Rasmussen S, Sollien R, Kiserud T. fetal age assessment based on femur length that 10 to 25 weeks of gestation, and reference ranges for femur length to head circumference ratios. Acta Obstet Gynecol Scand 2005; 84: 725-733 (Johnsen et al. 2005)
2. Gjessing HK Grøttum P, Eik-Nes SH. A direct method for ultrasound prediction of day of delivery: a new population based approach. Ultrasound Obstet Gynecol 2007; 30: 19-27 (Gjessing et al. 2007)
3. Øakland I, Nakling J Gjessing HK Grøttum P, Eik-Nes SH. Advantages of the population-based approach, two pregnancy dating: results from 23020 ultrasound examinations. Ultrasound Obstet Gynecol 2012; 39: 563-568 (Økland et al. 2012)
4. Økland I. Bias in second-trimester ultrasound dating related to prediction models and fetal measurements. Doctoral thesis, NTNU: 2012 (Økland 2012 NTNU dr.philos. Thesis)
5. Pay AS, Frøen JF, Staff AC, Jacobsson B, Gjessing HK. A new population-based reference curve for symphysis-fundus height. Acta Obstet Gynecol Scand 2013; 92: 925-33 (Pay et al. 2013)
[Note: The "Knowledge Center's method handbook" ("Kunnskapssenterets metodehåndbok") is available via NIPH: "Slik oppsummerer vi forskning".]
NOKC's References
If NOKC had included Bergen Group's Johnsen et al. 2004, i.e., fetal head biometery (HC & BPD) and gestational age) in with Johnsen et al. 2005 (femur length (FL) and gestational age with FL and fetal head ratios) in their assessment, there would have been a chance the problematic, unreliable BPD measurement would have been included as a discussion point in NOKC's "comprehensive assessment" ("helhetsvurdering"). Bergen Group's Terminhjulet or Term wheel relied/relies on the more robust fetal head circumference (HC) measurement, with the BPD measurement used as a cross-check and to assess fetal head shape when appropriate. Bergen Group's Terminhjulet or Term wheel uses HC & BPD to directly estimate gestational age and, therefrom, calculate EDD using the equivalent of Naegele's rule. (See: Warnings > BPD PROBLEMATIC) That said, comparing NCFM eSnurra Group's method (i.e., the appropriated, plagiarized Hutchon Method of PDEE) with the Bergen Group's Terminhjulet or Term wheel "really amounts to comparing apples to pears," as was stated by Bergen Group in conjunction with the problematic BPD with respect to NCFM eSnurra Group's unexplained BPD-based inclusions, exclusions and BPD measurement adjustments criteria and methods in their Gjessing et al. 2007 study.
- "We hold the opinion that the comparison conducted by the Trondheim Group suffers from conflicts of interest, but the Directorate of Health appears not to have realized that the comparative evaluation of the two methods really amounts to comparing apples to pears. The Directorate of Health also ignores the criticism raised against the Trondheim study (4): selection bias before and after weeks 18 – 20 of gestation; unclear exclusion criteria for fetuses with potentially hampered growth; and failing to account for the inclusion of fetuses with an elongated head whose biparietal diameter was adjusted based on the longitudinal axis of the skull." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "The midwives trained at the center in Trondheim have been recommended to measure the fronto-occipital diameter in fetuses considered to be dolichocephalic, and to use this information in order to assign an expanded virtual BPD for the calculation of gestational age and day of confinement. We cannot see that the authors have given any account of these fetuses or how this procedure influenced the statistics." (Source: Correspondence, Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, Ultrasound Obstet Gynecol 2008; 31: 225–228:)
NOKC & Evidence-informed Health Policy Using Research
Interestingly, in a 2008 study Norwegian Knowledge Centre for the Health Services (NOKC) explicitly stated: 1) NOKC's purpose with respect to "Evidence-informed Health Policy Using Research" and 2) NOKC's supposed scientific and professional independence from Directorate of Health. [Note: In January of 2016, NOKC separated from Directorate of Health and joined the Norwegian Institute of Public Health (NIPH).] It would appear NOKC's 2008 study was ignored with respect to Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation.
- "Norwegian Knowledge Centre for the Health Services summarizes and disseminates evidence concerning the effect of treatments, methods, and interventions in health services, in addition to monitoring health service quality. Our goal is to support good decision making in order to provide patients in Norway with the best possible care. The Centre is organized under The Directorate for Health and Social Affairs, but is scientifically and professionally independent. The Centre has no authority to develop health policy or responsibility to implement policies." (Source: "Evidence-Informed Health Policy: Using Research to Make Health Systems Healthier" Ray Moynihan, Andrew David Oxman, John N. Lavis, and Elizabeth Paulsen Rapport Nr 1-2008, Project number 265. Oslo: Nasjonalt kunnskapssenter for helsetjenesten, January 2008. ISBN 978-82-8121-187-2, ISSN 1890-1298)
- "The study’s seven main implications for those establishing or administering organisations to produce clinical practice guidelines or health technology assessments or organisations to support the use of research evidence in developing health policy include:
1. Collaborate with other organisations
2. Establish strong links with policymakers and involve stakeholders in the work
3. Be independent and manage conflicts of interest among those involved in the work
4. Build capacity among those working in the organisation
5. Use good methods and be transparent in the work
6. Start small, have a clear audience and scope, and address important questions
7. Be attentive to implementation considerations even if implementation is not a remit"
(Source: ibid.)
NOKC's Knowledge delivery (or knowledge provisioning) in response to the official request (Forslagsnr: 792, 15.11.2013) made by Directorate of Health and Ministry of Health and Care Services was inadequate or nonexistent on multiple levels. A 2016 Norwegian study, Malterud et al. 2016, examined NOKC's process with the following results:
- Results "From a total sample of 151 SRs published by the NOKC in the period 2004–2013, a purposive subsample from 2012 (14 publications) advised major caution about their conclusions because of the quality or relevance of the underlying documentation. Although the case study did not include a systematic investigation of uptake and policy consequences, SRs were found to be inappropriate as universal tools for health policy decision-making."
- "We believe that current EBM-based NOKC studies seek to provide a legitimate basis for health policy decision-making in Norway, and we endorse the idea that certain domains of inquiry may be well suited to such approaches. However, given the large proportion of recent NOKC deliveries that lack substantial conclusions, we must also reflect on the potential policy consequences of ‘empty’ knowledge deliveries. As a broad range of complex interventions cannot be adequately evaluated by the EBM format, there will be limited availability of ‘authorized’ research documentation, and SRs will be unable to offer strong conclusions about positive effects. This is not the same as documentation of negative or zero intervention effects. Often, the issues leading to SR commissions are controversial, and the delivery is expected to recommend a direction or choice. The present findings highlight the possibility of policy decision-making in which political interests (as in “this government does not want to support such a reform”) may be legitimized by SRs that draw weak or deficient conclusions, which are then interpreted as evidence-based warnings against the intervention in question. In this way, the EBM evidence hierarchy may actually contribute to concealing the foundation of policy decision-making rather than providing transparency."
- Conclusion In this case study exploring selected publications from the NOKC, we have demonstrated that EBM is not universally suited to knowledge provision for every kind of health policy decision-making. Our analysis raises the question of whether the EBM, represented here by an independent government organization, undertakes too broad a range of commissions using a range of strategies that seem too confined. As far as possible, healthcare policymaking should be based on relevant and transparent knowledge, taking account of the context of the intervention. However, we do not share a belief that the complex and messy nature of policy processes in general is compatible with the standards of EBM. (Source: "Evidence-based medicine – an appropriate tool for evidence-based health policy? A case study from Norway" Kirsti Malterud, Anne Karen Bjelland, Kari Tove Elvbakken. Health Research Policy and Systems 2016 14:15. https://doi.org/10.1186/s12961-016-0088-1 Received: 2 October 2015, Accepted: 22 February 2016, Published: 5 March 2016)
Corrupted Process: Torunn Janbu of Directorate of Health
In the excerpt below, Torunn Janbu, dr.med. (MD, PhD), Head of the Department of Hospital Services, Norwegian Directorate of Health, falsely stated it was NOKC who had "pointed out" the "validation strategy" (i.e, Økland's 2012 NTNU dr.philos. Thesis, "the fix").
- "The Norwegian Knowledge Centre for the Health Services pointed out that one possible validation strategy to assess different term prediction models consists in comparing the characteristics of the methods in question through measurements within one and the same population. This was done in a PhD thesis in 2012 (2), and the work has been presented in three international publications (7 – 9)." (Source: "One Norwegian national tool for estimating date of delivery and fetal age" Torunn Janbu, MD, PhD, specialist in general and orthopaedic surgery, Head of the Department of Hospital Services, Norwegian Directorate of Health. The author has completed the ICMJE form and declares no conflicts of interest., Tidsskr Nor Legeforen nr. 9, 2016; 136, p. 790)
- "..."the fix" itself is typically handled subtlety, with finesse (albeit with all the implied penalties or benefits), not with visible arrogance, and never, ever in a publicly available document." This is an example of another competence having been exceeded. [Note: Since the publication of LailasCase.com, the NOKC documents referenced above are, strangely, no longer publicly available. In fact, the entire searchable database of requests to NOKC is no longer publicly available.]
Corrupted Process: The Directorate of Health's Letter
Jens Grøgaard, Senior Adviser, Directorate of Health signed the Directorate's 10.12.2014 letter with Torunn Janbu, then Acting Division Director, Directorate of Health; a letter which was distributed to Helse Midt-Norge RHF, Helse Nord RHF, Helse Sør-Øst RHF and Helse Vest RHF to enact Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care. In this letter Økland's 2012 NTNU dr.philos. Thesis (not a PhD as degree as Torunn Janbu would have people believe) was the one and only document discussed, cited and footnoted in Directorate's 10.12.2014 letter; and, it was the one and only document presented as independent, academic justification for Directorate of Health's selection of NCFM eSnurra Group's eSnurra "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) as the exclusive implementation vehicle of Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation. At no time did Torunn Janbu or anyone else from Directorate of Health disclose:
- Økland had been a published member of NCFM eSnurra Group since 2007
- Økland's 2012 NTNU dr.philos. Thesis had been supervised by NCFM eSnurra Group: Principal Supervisor: Sturla H. Eik-Nes, MD, PhD , Co-supervisors: Håkon K. Gjessing, PhD and Per Grøttum, MD, PhD, the 3 original members of the NCFM eSnurra Group and the 3 NCFM eSnurra claimed "copyright owners" (© 2007 EikNes, Grøttum og Gjessing) as stated on the NCFM eSnura website
- Økland's 2012 NTNU dr.philos. Thesis' Assessment Committee included Jens Grøgaard, Senior Adviser, Directorate of Health
- Økland's 2012 NTNU dr.philos. Thesis' public defense on 13.01.2012 had been adjudicated by Jens Grøgaard, Senior Adviser, Directorate of Health
- Økland was, and is, a medical doctor with a specialty in obstetric medicine
- Inger Økland is presently in her 2nd year of employment with Directorate of Health and, simultaneously, a member of NCFM eSnurra Group [Note: Clearly, Torunn Janbu could not have disclosed this last point before it had actually occurred. Nevertheless, Økland's employment with Directorate of Health is decidedly relevant and is included for conflict-of-interest completeness.]
Jens Grøgaard: Breech of Medical Ethics: NMA Ethics Council
In 2012, Jens Grøgaard coauthored a report titled "Age estimation in youths and young adults" as part of a Norwegian Directorate of Immigration (UDI) commissioned and since-completed study; a study managed by Norwegian Computing Center (Norsk Regnesentral) titled: 'Development of improved methods or basis for medical age assessments of minors and young adults," which listed BarneSak AS, Jens B. Grøgaard's company, as a Project Partner as follows:
- "BarneSak AS. MD and PhD Jens B. Grøgaard is a pediatrician who has participated in the age estimation of young asylum seekers in Norway from 2009 to 2013."
- used harmful ionizing radiation (x-rays) on unaccompanied asylum-seeking minors,
- for no medical benefit, whatsoever
- to estimate medical age using a highly dubious, medically & ethically flawed protocol,
- without prior, informed, voluntary consent of the asylum seekers,
- to generate highly questionable "medical" results,
- which Grøgaard certified and signed as an expert medical opinion,
- while working as a Medical Doctor and Senior Adviser, Norwegian Directorate of Health,
- to manufacture and certify a product of "medical evidence of medical age" for sale to UDI
- which UDI purchased form Grøgaard's company, BarneSak AS,
- for UDI to use as official, certified, medical evidence of asylum seekers' age
- to use as justification in their rendering of asylum decisions
- until Grøgaard was found to have breached multiple tenants of medical ethics by the Medical Ethics Council of the Norwegian Medical Association (below).
Medical Ethics: Cost & Benefit Analysis
Jens Grøgaard's company, BarneSak AS (Org No. 912283224) was founded in 2013 and reported operating profits (in 1,000 NOK) of: 1,290, 3,831 & 3, 627 in 2014, 2015 & 2016, respectively, for a cumulative reported operating profit of 8,748 NOK (in 1,000 NOK) or 8,748,000 NOK. For U.S. readers, that was a little more than $1 million. Ergo, the cost-benefit analysis is straightforward: Cost = ethical criticism amounting to a wrist slap; Benefit = $1,000,000 USD or 8,748,000 NOK, which may only serve to quantify a key economic distinction between Doctors with Borders and Doctors Without Borders.
An 04.01.2016 article in VG NYHETER titled "Uses millions for controversial age tests" ("Bruker millioner på omstridte alderstester") identified the process, some of the participants and some of the costs (below) as well as the full story.
- How the surveys are done
** Unilabs: Do X-rays of the hand carpus. Cost: 0.8 mill
** Institute of Clinical Dentistry at the University of Oslo: 9 mill
** Barnesak AS: Former child doctor with Oslo University Hospital, Jens Grøgaard (75), summarizes the studies and gives an evaluation to UDI. 3.2 million (Source: UDI) - Slik foregår undersøkelsene
** Unilabs: Gjør røntgenundersøkelse av håndroten. Kostnad: 0,8 mill
** Institutt for klinisk odontologi ved Universitetet i Oslo: 9 mill
** Barnesak AS: Tidligere barnelege ved Oslo Universitetssykehus, Jens Grøgaard (75), sammenfatter undersøkelsene og gir en vurdering til UDI. 3,2 mill (Kilde: UDI)
(Source: "Bruker millioner på omstridte alderstester" Av MARIA MIKKELSEN, HELGE MIKALSEN og TROND SOLBERG. VG NYHETER. 04.01.2016 05:25 - oppdatert 04.01.2016 09:57)
- "The doctor Jens Grøgaard terminates the agreement with Immigration about age testing of unaccompanied minor asylum seekers following criticism from the Council for Medical Ethics, reports TV2."
"Legen Jens Grøgaard har sagt opp avtalen med Utlendingsdirektoratet om alderstesting av enslige, mindreårige asylsøkere etter kritikk fra Rådet for legeetikk, melder TV 2." - "There has been a great strain on the family, and I want to put this behind me, the doctor says to TV2 ."
"Det har vært en stor påkjenning for familien, og jeg ønsker å legge dette bak meg, sier legen til TV 2."
(Source: "While we are waiting for a new method for the age determination of young asylum seekers" Norwegian: "Lege gir seg etter kritikk av alderstester for UDI" ABC Nyheter 23. des. 2016 18:58 – Oppdatert 23. des. 2016 18:58)
A 2017 University of Oslo Masters Thesis by Aisha Munir titled "Age examination of single minor asylum seekers" ("Aldersundersøkelse av enslige mindreårige asylsøkere") provides a
- "Former head of the children's department at Ullevål Hospital, Jens Grøgaard, elected 1700 children in 2016. He is now chairman and director of the private company Barnesak AS. The company had a turnover of 4 million in 2015 with a profit of 2 million (purehelp.no). Unilabs who perform X-rays of minors left wrists and the Faculty of Odontology as X-rays photograph the teeth of the children, both send their reports to Grøgaard. Furthermore, he delivered an overall assessment to the UDI about the children's age, without having met them. Grøgaard has been heavily criticized by colleagues for the past three years with assignments from the UDI to use an unsuitable age test."
"Tidligere leder av barneavdelingen på Ullevål sykehus, Jens Grøgaard, alderstestet 1700 barn i 2016. Han er nå styreleder og direktør i privatselskapet Barnesak AS. Selskapet hadde en omsetning på 4 millioner i 2015 med et overskudd på 2 millioner (purehelp.no). Unilabs som utfører røntgen av mindreåriges venstre håndledd og det Odontologiske fakultet som røntgenfotograferer tennene til barna, sender begge hver sin rapport til Grøgaard. Videre leverer han en samlet vurdering til UDI om barnas alder, uten å ha møtt dem. Grøgaard har de tre siste årene med oppdrag fra UDI blitt kraftig kritisert av kollegaer for å bruke en uegnet alderstest." - "The leader of the Child Radiology Association says that resistance is strong against the method because the child's living conditions, diet, ethnicity, and health conditions affect the age. Everyone who knows teenagers knows that they are developing at an uneven pace. It is not possible to take an X-ray of the carpus of a child of unknown age, compare with the image atlas, to determine the age of the child. The error margin appears to be up to five years (Sæther, 2016)."
"Lederen av Barneradiologisk forening sier at motstanden er sterk mot metoden fordi barnets levekår og kosthold, etnisitet, og helsemessige forhold påvirker alderen. Alle som kjenner tenåringer, vet at de utvikler seg i ujevn takt. Det er ikke mulig å ta et røntgenbilde av en håndrot til et barn med ukjent alder, sammenligne med billedatlaset, for så å fastsette barnets alder. Feilmarginen vises å være opptil fem år (Sæther, 2016)." (Source: "Age examination of single minor asylum seekers" "I did not come here to find out how old I am" ("Aldersundersøkelse av enslige mindreårige asylsøkere" «Jeg kom ikke hit for å finne ut hvor gammel jeg er») Aisha Munir. Master's thesis in Social Anthropology, Department of Social Anthropology, UNIVERSITY IN OSLO, Spring 2017)
In a 05.03.2018 article in Tidsskrift for Den norske legeforening, the ethical issues of age assessment of young asylum seekers were discussed with respect to medical harm and prior, informed, voluntary consent of dubious age assessment methods which use harmful ionizing radiation (x-rays) for no medical benefit. (Source: "While we are waiting for a new method for the age determination of young asylum seekers" Norwegian: "Mens vi venter på en ny metode for aldersbestemmelse av unge asylsøkere" SVEIN AARSETH, STINE KATHRIN TØNSAKER. Publisert: 5. mars 2018, Utgave 5, 6. mars 2018. Tidsskr Nor Legeforen 2018. DOI: 10.4045/tidsskr.17.0960. Mottatt 5.11.2017, første revisjon innsendt 10.12.2017, godkjent 25.1.2018.)
Grøgaard's Breaches of Medical Ethics
Included below are 2 excerpts from the article "Criticism to the doctor for age testing" ("Kritikk til lege for alderstesting") by Tove Myrbakk, Nordland legeforening, Den Norske Legeforening 12. desember 2016, which articulates Jens Grøgaard's breaches of medical ethics and the associated criticisms delivered by the Medical Ethics Council of the Norwegian Medical Association.
- "The letter from the Council for Medical Ethics states: "The Council would like to note that the accused physician performs a very specific case-law mission for the UDI. It is not a medical indication for the investigations, and the method used is controversial. Age assessment with X-ray of hand rot and dental examination requires valid consent, ie the consent is given on the informed basis of a consent person. There is reason to question whether voluntary informed consent is possible for these investigations.""
("I brevet fra Rådet for legeetikk står det blant annet: «Rådet vil bemerke at innklaget lege utfører et meget spesielt sakssyndigeoppdrag for UDI. Det er ikke medisinsk indikasjon for undersøkelsene, og metoden som benyttes er omstridt. Aldersvurdering med røntgen av håndrot og tannundersøkelse forutsetter gyldig samtykke, altså at samtykket er gitt på informert grunnlag av en samtykkekompetent person. Det er grunn til å stille spørsmål ved om frivillig informert samtykke er mulig å oppnå for disse undersøkelsene.»") - "They further state that "the evaluating physician has a special responsibility to ensure that the requirements according to ethical rules for chapter 1, sections 1 and 2 are taken care of. The Council of Medical Ethics finds that the accused doctor, by conducting the age-testing of minors, single asylum seekers based on unsafe methods that he himself states are "not as good as desired" and without the opportunity to secure a valid consent, has acted contrary to ethical Rules for doctors chapter 1, §! 2 and 9. In addition, the Council considers that he has issued expert statements which, in the opinion of the Council, are not based on "as extensive surveys as the purpose suggests, cf. Chapter IV, Section 3. The Council of Medical Ethics, on this basis, gives criticism to the accused doctor for violation of Ethics rules.""
("De skriver videre at det «påhviler vurderende lege et særlig ansvar for å sikre at kravene etter Etiske regler for kap. 1, §§ 1 og 2 er ivaretatt. Rådet for legeetikk finner at innklaget lege ved å gjennomføre alderstesting av mindreårige, enslige asylsøkere basert på usikre metoder som han selv uttaler at «ikke er så gode som ønsket», og uten mulighet for å sikre et gyldig samtykke, har opptrått i strid med Etiske regler for leger kap 1, §! 2 og 9. Videre mener Rådet at han har avgitt sakkyndige erklæringer som etter Rådets vurdert ikke bygger på «så omfattende undersøkelser som formålet tilsier, jf. kap IV § 3. Rådet for legeetikk gir på denne bakgrunnen kritikk til innklaget lege for brudd på Etiske regler».")
Included below are the relevant sections and paragraphs of the Code of Ethics for Doctors which Grøgaard breached, as published by Den norske legeforening "Code of Ethics for Doctors - Adopted by the Representative Body in 1961 and subsequently amended, most recently in 2015."
- I. General provisions
§ 1 A doctor shall protect human health. A doctor shall cure, alleviate and console. A doctor shall help the ill to regain their health and the healthy to preserve theirs.
A doctor shall base his practice on respect for fundamental human rights, and on truth and justice in relations with patients and to society.
§ 2 A doctor shall safeguard the interests and integrity of the individual patient. Patients must be treated with caring and respect. Cooperation with patients should be based on mutual trust and, where possible, on informed consent.
Doctors have different roles as treatment provider, expert and administrator of welfare benefits. These roles have a bearing on how doctors behave, and how they treat sensitive information. A clear distinction must be made between their roles of treatment provider and expert. Doctors are responsible for providing necessary information and appropriate information about their role and the purpose of the contact.
§ 9 In examinations and treatment a doctor shall only employ methods indicated by sound medical practice. Methods which expose the patient to unnecessary risk shall not be employed.
If a doctor does not possess the skill a method calls for, he or she shall ensure that the patient receives other competent treatment.
§ 3 A doctor shall base his/her certificates on the necessary information and on examinations that are sufficiently extensive for the purpose.
While profiting, handsomely, from BarneSak AS, Grøgaard made a lateral expansion into a new market where he could leverage the same strategy but with one, 180-degree twist. He used his knowledge and experience from establishing an exclusive provider of medically & ethically flawed evidence-manufactured medicine (i.e., dubious x-ray-based "official certification" of medical age) for Norwegian Directorate of Immigration (UDI) to establishing an exclusive provider of evidence-obviated medicine for Norwegian Directorate of Health's knowledge-obviated, medially & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine with respect to obstetric medicine, fetal medicine and obstetric clinical care. All without securing a pregnant woman's prior, informed, voluntary, explicit consent; thereby, placing control of all age-related pregnancy and abortion decisions under the control of Directorate of Health with their exclusive NCFM eSnurra Group implementation; an implementation for which 3 NCFM eSnurra Group members Sturla H. Eik-Nes, Per Grøttum and Håkon K. Gjessing claim to be the "copyright owners," (© 2007 EikNes, Grøttum og Gjessing), as stated on the NCFM eSnura website, of which It would appear Jens Grøgaard, Senior Adviser, Directorate of Health, was able to make his lateral expansion into the market of establishing estimated date of delivery (EDD), gestational age (GA) and fetal age for all pregnancies and abortions in Norway, effortlessly, because Jens Grøgaard was neither burdened nor conflicted by his knowledge of the fact that what he was doing was medically & ethically flawed and willfully negligent.
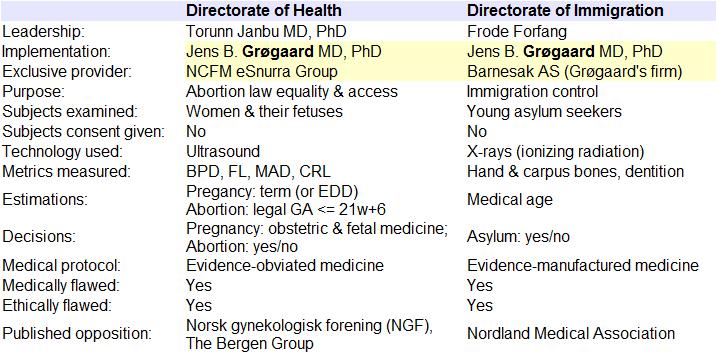
It is interesting to note that the last word from the Norwegian Medical Association's description of their free, online course "Fundamentals of Medical Ethics" states:
- "Lastly a word on the centrality of the patient in any discussion on medical ethics. Most medical associations acknowledge in their foundational policies that ethically, the best interests of the individual patient should be the first consideration in any decision on care. This course will only succeed if it amplifies this imperative – TO PUT THE PATIENT FIRST."
This "Fundamentals of Medical Ethics" course was authored by John R. Williams, former Director of Ethics at the World Medical Association (WMA). Interestingly, Torunn Janbu, Director of Hospital Services of the Specialized Health Care Services, Norwegian Directorate of Health is a former President, Norwegian Medical Association (2005-2007) and a former Chairperson, Medical Ethics Committee of the WMA (2010-2013). Consequently, one can only wonder how the wheels came off Torunn Janbu's medical ethics wagon with respect to her leadership role in promoting, deciding and implementing Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation; a Recommendation that implemented a protocol of evidence-obviated medicine; a Recommendation which serves as a textbook example of systemic, harms-causing misconduct, manipulation and corruption.