NGF & Bergen Group
NGF & Bergen Group Doctor-Scientists Warned Directorate of Health of the Risks & Consequences
Five of Norway's venerated doctor-scientists of obstetric medicine, fetal medicine and obstetric clinical care, collectively known as Bergen Group (led by Torvid Kiserud, MD, PhD) coauthored the 2015 article "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Journal of the Norwegian Medical Association: Tidsskrift for Den norske legeforening. This seminal article stated Directorate of Health's 2014 Recommendation was "medically flawed" and "critical mistakes may follow." More specifically, this seminal article identified specific risks and consequences of Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" within a government-mandated protocol of evidence-obviated medicine.
Included below are the names of the 5 doctor-scientists of Bergen Group who spoke truth to power, the medical community and the public when they clearly and explicitly informed Directorate of Health, "critical mistakes may follow from the failure to include all available information when fetal age is assessed" in the practice of evidence-based medicine.
These 5 Bergen Group doctor-scientists clearly and explicitly warned Directorate of Health their 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine was medically flawed. More specifically, Directorate of Health were clearly and explicitly warned of the risks and consequences of their 2014 Recommendation in Bergen Group's article "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Norwegian Medical Association's Tidsskrift for Den norske legeforening. Some of the risks and consequences and their causes are included in the excerpts below. Note: the red bold text is used to identify consequences and issues which directly apply to the increased medical risks, critical medical mistakes and grievous medical harms which were inflicted, unnecessarily, upon Laila and her baby, and other women and their babies, by the implementation of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation.
Five of Norway's venerated doctor-scientists of obstetric medicine, fetal medicine and obstetric clinical care, collectively known as Bergen Group (led by Torvid Kiserud, MD, PhD) coauthored the 2015 article "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Journal of the Norwegian Medical Association: Tidsskrift for Den norske legeforening. This seminal article stated Directorate of Health's 2014 Recommendation was "medically flawed" and "critical mistakes may follow." More specifically, this seminal article identified specific risks and consequences of Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's "method" within a government-mandated protocol of evidence-obviated medicine.
Included below are the names of the 5 doctor-scientists of Bergen Group who spoke truth to power, the medical community and the public when they clearly and explicitly informed Directorate of Health, "critical mistakes may follow from the failure to include all available information when fetal age is assessed" in the practice of evidence-based medicine.
- Bergen Group Coauthors
Cathrine Ebbing, MD, PhD
Synnøve Lian Johnsen, MD, PhD
Jørg Kessler, MD, PhD
Torvid Kiserud, MD, PhD
Svein Rasmussen, MD, PhD
These 5 Bergen Group doctor-scientists clearly and explicitly warned Directorate of Health their 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine was medically flawed. More specifically, Directorate of Health were clearly and explicitly warned of the risks and consequences of their 2014 Recommendation in Bergen Group's article "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Norwegian Medical Association's Tidsskrift for Den norske legeforening. Some of the risks and consequences and their causes are included in the excerpts below. Note: the red bold text is used to identify consequences and issues which directly apply to the increased medical risks, critical medical mistakes and grievous medical harms which were inflicted, unnecessarily, upon Laila and her baby, and other women and their babies, by the implementation of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation.
- "We hold the opinion that this recommendation is medically flawed and that the Directorate has conducted a muddled investigation process."
- "We have the impression that users of the Trondheim method have been routinely using the 18-week routine measurements to calculate the pregnancy term and overrule any fetal age determination based on known time of ovulation, in-vitro fertilisation or first-trimester ultrasound."
- "The noise around these matters has subsided in the course of this autumn’s debate, but unilateral reliance on routine ultrasound examinations is unwarranted."
- "If this procedure were to be implemented, the sickest fetuses would suffer the most from incorrect predictions, as they are often small for their age. Ultrasound measurements taken in the second trimester will therefore suggest a lower than true age."
- "We argue that critical mistakes may follow from the failure to include all available information when fetal age is assessed."
- "Had the Directorate of Health listened to the expert opinion expressed by the Norwegian Society of Gynaecology and Obstetrics (2), the recommendation would have been better balanced and based on sound knowledge."
- "In this instance we feel that the Directorate of Health has acted beyond their competence and that they have simplified the issues beyond all understanding."
“It's not what you don't know that kills you, it's what you know for sure that ain't true.”
― Mark Twain
― Mark Twain
Bergen Group did not predict the consequences (i.e., increased medical risks, critical medical mistakes and grievous medical harms) caused by Directorate of Health's 2014 Recommendation because neither Bergen Group nor NGF needed to predict risks and consequences which were already known from their expert medical and scientific knowledge; the same expert knowledge Bergen Group and NGF used to clearly and explicitly warn Ministry of Health & Care Services, Directorate of Health, the medical community and the public. Ministry of Health & Care Services and Directorate of Health knew, or reasonably should have known, of the risks and consequences for their 2014 Recommendation from the clear, explicit, published warnings identified by Bergen Group, NGF and others. Consequently, Ministry of Health & Care Services and Directorate of Health, in conscious disregard of the risks and consequences identified by Norway's obstetric & fetal medicine experts, international practice guidelines and Norway's epidemiological experts, implemented their knowledge-obviated, medically and ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's EDD estimation "method" (i.e. the appropriated, plagiarized, misused Hutchon Method of PDEE) with a government-mandated protocol of evidence-obviated medicine; a policy, protocol and "method" proven to cause increased medical risks, critical medical mistakes and grievous medical harms for some of Norway's women and their fetuses/babies.]]
The excerpt below is from a thought provoking 2012 article in Tidsskrift for Den norske legeforening authored by Torvid Kiserud, MD, PhD, Department of Obstetrics and Gynaecology, Haukeland University Hospital, Bergen, Norway; professor at University of Bergen’s Department of Clinical Science at Haukeland University Hospital; external advisor to WHO and member of the Steering Committee of the WHO Fetal Growth Study; leader of Bergen Group and developer of the Terminhjulet (Term wheel) method for fetal & gestational age determination.
Norway's government health authorities have implemented Directorate of Health's science-bending, knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's suboptimal, unilateral ultrasound-based EDD estimation "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) with a government-mandated protocol of evidence-obviated medicine which causes misclassifications of gestational age. And, in so doing, Ministry of Health & Care Services and Directorate of Health have created the same perinatal mortality problems identified by Larssen et al 1982, as discussed in Stray-Pedersen 1991, below.
Norwegian Society for Gynecology & Obstetrics (Norsk gynekologisk forening (NGF)
Norsk gynekologisk forening (NGF) (Norwegian Society for Gynecology & Obstetrics) were excluded from the decision-making process and ignored by Directorate of Health. Following is a relevant excerpt from Bergen Group's article: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age."
)
NGF: Directorate of Health's Recommendation is "highly reprehensible" & "can be directly dangerous"
Included below (emphasis added) is the NGF article: "NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin" written in response to the Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. The article was authored by: Jone Trovik, Leder i NGF (President of NGF), Rolf Kirschner, Leder Kvalitetsutvalget (Head of Quality Committee) and Pål Øian, Hovedredaktør Veileder i fødselshjelp (Chief Editor: Guidelines in Obstetrics). The article is included in its entirety due to its significance. (Source: NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin, Jone Trovik, Rolf Kirschner, Pål Øian. Norsk gynekologisk forening, Den Norske Legeforening Nyheter, 2014) (Note: The source is in Norwegian; this translation is via Google Translate.)
"Directly Dangerous"
NGF's medical experts explicitly warned Directorate of Health of the risks and consequences of their 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine to effect unilateral reliance on NCFM Group's ultrasound-based EDD estimation "method" to establish gestational age for all pregnancies and abortions in Norway. Specifically, NGF warned Directorate of Health that their 2014 Recommendation "can be directly dangerous." The plethora of obstetric and fetal medicine evidence assembled and presented within LailasCase.com proves NGF were, and remain, right.
The following year NGF national representatives coauthored the 16.02.2015 article "The Directorate of Health overrules national, professional guidelines" in Dagens Medisin, Kronikk og debatt. Listed below are the NGF coauthors.
The excerpt below is from a thought provoking 2012 article in Tidsskrift for Den norske legeforening authored by Torvid Kiserud, MD, PhD, Department of Obstetrics and Gynaecology, Haukeland University Hospital, Bergen, Norway; professor at University of Bergen’s Department of Clinical Science at Haukeland University Hospital; external advisor to WHO and member of the Steering Committee of the WHO Fetal Growth Study; leader of Bergen Group and developer of the Terminhjulet (Term wheel) method for fetal & gestational age determination.
- "Knowing the correct fetal age is crucial for treatment and monitoring during the pregnancy:
- chorionic villus sampling (CVS) after week 10,
- targeted diagnostic testing in weeks 11 – 13,
- amniocentesis after week 15,
- routine ultrasound examination at 18 weeks,
- discussion of viability and delivery after 24 weeks,
- lung maturity injection prior to 34 weeks."
- "Children born prior to 37 weeks are considered premature and after 42 weeks post-term. Fetal age reflects fetal development and is a key determinant of morbidity and perinatal death. Therefore all available information must be included to determine fetal age as correctly as possible." (Source "How Long Does a Pregnancy Last?" Torvid Kiserud. Tidsskrift for Den norske legeforening nr. 1, 2012; 132. p. 8. Published: 10 January 2012. HTML version)
- "However, the basis for determining gestational age is not the end of the pregnancy, but its beginning." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Bergen Group. Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "However, the issue at stake is not the accuracy of the predicted date of a normal delivery, it is the accuracy of the fetal age, which is an essential factor in clinical situations throughout the pregnancy." (Source: ibid.)
- "Fetal age, fetal size, length of pregnancy and date of delivery are obviously all related data. However, it is impossible to deduce fetal age routinely from the predicted date of delivery. Only 4 per cent of women give birth at their estimated due date; in order to determine gestational age, it is clearly necessary to take account of the time of conception. The Directorate of Health have demonstrated their lack of understanding of these differences, and they have failed to appreciate that the Trondheim Group [NCFM eSnurra Group] looked only at term prediction (3)." (Source: ibid.)
- "For a successful technology, reality must take precedence over public relations, for nature cannot be fooled."
Norway's government health authorities have implemented Directorate of Health's science-bending, knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's suboptimal, unilateral ultrasound-based EDD estimation "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) with a government-mandated protocol of evidence-obviated medicine which causes misclassifications of gestational age. And, in so doing, Ministry of Health & Care Services and Directorate of Health have created the same perinatal mortality problems identified by Larssen et al 1982, as discussed in Stray-Pedersen 1991, below.
- "In order to improve our perinatal care, a survey of approximately half of all perinatal deaths during 1 year (1980) was performed [2]. The results indicated that 30% of the perinatal deaths could be ascribed to a non-satisfactory antenatal service and therefore could have been avoided. The main problems were no reaction to obvious clinical signs and not instituting appropriate care in risk pregnancies." (Source: "Perinatal mortality in Norway: experience with perinatal audit" Babill Stray-Pedersen. European Journal of Obstetrics and Gynecology and Reproductive Biology, Vol. 41, Issue 1, p20–22 Published in issue: August 20, 1991 ) [Note: Citation 2: "2 Larssen KE, Bakketeig LS, Bergsjo P et al. Perinatal audit in Norway 1980. NIS rapport 7/82 Norwegian Institute for Hospital Research, Trondheim, Norway.]
- "no reaction to obvious clinical signs": In Laila's case, there was a 15-day discrepancy between Laila's LMPD-based EDD and Laila's assigned, suboptimal, unilateral ultrasound-based NCFM eSnurra BPD-based EDD. However, this medical evidence of a known 15-day discrepancy was obviated from all medical evidence and, consequently, it was obviated from all medical thinking, medical decision-making and medical actions in accordance with the government-mandated protocol of evidence-obviated medicine implemented by Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation. [Note: The discrepancy between Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD and and Laila's assigned, suboptimal, unilateral ultrasound-based NCFM eSnurra BPD-based EDD was 14 days.]
- "not instituting appropriate care in risk pregnancies": as a result of "no reaction to obvious clinical signs" due to the government-mandated protocol of evidence-obviated medicine, the medical evidence needed to identify "risk pregnancies" (i.e., accurate gestational age) is eliminated from all medical evidence and therefore, eliminated from all thinking, medical decision-making and medical actions, thereby making "instituting appropriate care" impossible.
- "a non-satisfactory antenatal service": Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2014 Recommendation has mandated a "a non-satisfactory antenatal service."
- "Correct fetal age acts in the difficult cases of life or death. We expect all available information to be used to arrive at the safest or most likely age of the fetus, and it can not be based on routine ultrasound alone." (Source: "Abort: Ultralyd er ikke nok for å bestemme fosterets alder" ("Abortion: Ultrasound is not enough to determine fetal age") Cathrine Ebbing, Synnøve Lian Johnsen, Jørg Kessler, Torvid Kiserud. Aftenposten Kronikk, Published: 16.okt.2014 14:28 updated: 17.okt.2014 11:49.)
Norwegian Society for Gynecology & Obstetrics (Norsk gynekologisk forening (NGF)
Norsk gynekologisk forening (NGF) (Norwegian Society for Gynecology & Obstetrics) were excluded from the decision-making process and ignored by Directorate of Health. Following is a relevant excerpt from Bergen Group's article: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age."
- Running roughshod over medical expertise
"The Norwegian Society of Gynaecology & Obstetrics recently reviewed available knowledge about the determination of gestational age. They gave their resulting recommendations in a revised edition of their birthing guidelines for the medical profession, Veileder i fødselshjelp 2014 (2). They recommend routine ultrasound examination in the second trimester, and that the gestational age in cases of in-vitro fertilisation be based on the time of conception. They also recommend that if the gestational age has been determined earlier in the pregnancy, this should never be changed as a consequence of later ultrasound examinations. This is entirely in line with international guidelines – and both Norwegian methods are included." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093) Note: the specific reference (2) in the excerpt above is: "Ultralydundersøkelser i den alminnelige svangerskapsomsorgen" or "Ultrasonography in the general antenatal care" is located on pdf pages 15-18 of Veileder i fødselshjelp 2014.)
)
- Norwegian Gynecological Association (NGF) says Directorate of Health's handling of new recommendations "can be directly dangerous."
The Norwegian Gynecological Association (NGF) rages against the Directorate of Health's (Hdir) management of the new recommendations for the determination of pregnancy length and term, and believes that Hdir has handled this in a critical and low-confidence manner.
Norsk gynekologisk forening (NGF) raser mot Helsedirektoratets (Hdir) håndtering av de nye anbefalingene for fastsetting av svangerskapslengde og termin, og mener Hdir har håndtert dette på en kritikkverdig og lite tillitsvekkende måte.
"May be directly dangerous"
NGF also believes that the way Hdir has handled the case can be directly dangerous in dealing with difficult clinical issues. "
«Kan være direkte farlig»
NGF mener også at måten Hdir har håndtert saken på «kan være direkte farlig i forhold til håndtering av vanskelige kliniske problemstillinger.»
Now, they ask their members instead to use the recommendations given in the Guide to Childbirth.
Nå ber de sine medlemmer om i stedet å bruke anbefalingene gitt i Veileder i fødselshjelp.
In October, Hdir stated that the entire country should use the same method for calculating pregnancy length and term.
I oktober fastslo Hdir at hele landet skal bruke samme metode for utregning av svangerskapslengde og termin.
The reason is that in Norway different methods are used to determine the length of pregnancy and that this leads to systematic differences around the country.
Bakgrunnen er at det i Norge brukes ulike metoder for å bestemme svangerskapets lengde, og at dette fører til systematiske forskjeller rundt om i landet.
However, obstetricians have strongly disagreed in the choice of method, and now the Norwegian gynecological association is strongly criticized.
Fødselsleger har imidlertid vært sterkt uenige i valget av metode, og nå kommer Norsk gynekologisk forening med sterk kritikk.
- Have not been involved at all
While Hdir claims that the decision is well-grounded, including in a report from the Knowledge Center, meets with the academic communities and input from national and international expertise - NGF considers the opposite, saying "they have not been involved in this case".
- Har overhodet ikke vært involvert
Mens Hdir hevder at avgjørelsen er grundig forankret, blant annet i en rapport fra Kunnskapssenteret, møter med fagmiljøene og innspill fra nasjonal og internasjonal ekspertise – mener NGF det motsatte, og sier de «overhodet ikke vært involvert i denne saken.»
Norsk gynekologisk forening says Hdir's handling of new recommendations "can be directly dangerous".
Hdir: - Has had open contact
Torunn Janbu, Department Director for Hospital Services in Hdir, says to Dagens Medisin that "Hdir has had an open contact with national and international experts" in the process.
Hdir: - Har hatt åpen kontakt
Torunn Janbu, avdelingsdirektør for sykehustjenester i Hdir, sier til Dagens Medisin at «Hdir har hatt en åpen kontakt med nasjonale og internasjonale eksperter» i prosessen.
She says she detects that NGF disagrees with Herdir's conclusion.
Hun sier hun registrerer at NGF er uenig i Hdirs konklusjon.
"It is disturbing that NGF does not choose to follow the Directorate-General's scientific reasoned recommendation. The Directorate of Health misses scientific evidence for the allegations promoted, says Janbu.
– Det er urovekkende at NGF velger ikke å følge Helsedirektoratets vitenskapelig begrunnede anbefaling. Helsedirektoratet savner vitenskapelig dokumentasjon for de påstander som fremmes, sier Janbu.
NGF: - No dialogue
However, NGF's Pål Øian, who is the main editor of a supervisor in childbirth, refutes that the Directorate of Health has had dialogue with NGF:
NGF: - Ikke dialog
Men NGFs Pål Øian, som er hovedredaktør for veileder i fødselshjelp, tilbakeviser at Helsedirektoratet har hatt dialog med NGF:
– Probably they have talked to gynecologists who are members of the association, but who do not represent it," Øian says to Dagens Medisin.
He shows that he and colleagues in the meeting with Hdir did not get information about who Hdir had talked to during the process, neither in terms of national or international professionals.
Han viser til at han og kolleger i møte med Hdir ikke fikk informasjon om hvem Hdir hadde snakket med under prosessen, verken når det gjelder nasjonale eller internasjonale fagfolk.
- This despite the fact that we explicitly asked for this, says Øian.
– Dette til tross for at vi spurte eksplisitt etter dette, sier Øian.
In response to Øian's claims, Janbu writes in an email to Dagens Medisin:
- As you can see from our response, they got their name.
Som svar på Øians påstander skriver Janbu i en epost til Dagens Medisin:
– Som du ser av svaret vårt, fikk de navn.
Read the opinion of Torunn Janbu and the Norwegian Directorate of Health in its entirety here.
Les uttalelsen fra Torunn Janbu og Helsedirektoratet i sin helhet her.
Read the statement by Pål Øian and the Norwegian Gynecological Society in full here.
Les uttalelsen fra Pål Øian og Norsk Gynekologisk forening i sin helhet her.
The abortions were not illegal
Abortene var ikke ulovlige
It was earlier this year that health and safety minister Bent Høie asked for a review of late abortion, on suspicion that the abortions had taken place in violation of the law.
Det var tidligere i år at helse- og omsorgsminister Bent Høie ba om en gransking av senaborter, på bakgrunn av mistanke om at abortene hadde skjedd i strid med loven.
Following a massive debate on the limit of late-onset, following the finding that some women were aborted after the 22st week of pregnancy, the Directorate of Health stated that the absolute limit was 21 weeks and 6 days.
Etter en massiv debatt om grensen for senabort, etter at det kom frem at noen kvinner fikk ta abort etter 22. svangerskapsuke, presiserte Helsedirektoratet at den absolutte grensen er på 21 uker og 6 dager.
Early in November this year, however, the investigation showed that the fetus had such malformations that it was legal to abort them - even after the absolute limit for abortion, according to NRK.
Tidlig i november i år viste imidlertid granskingen at fostrene hadde så store misdannelser at det var lovlig å abortere dem – også etter den absolutte grensen for abort, ifølge NRK.
(Source: "Gynekologer raser mot Helsedirektoratet" Anne Grete Storvik. Dagens Medisin Published: 2014-12-08 14.04)
- Dagens Medisin 2014-12-08 14.04: "Read the statement by Torunn Janbu and the Norwegian Directorate of Health in full here."
Les uttalelsen fra Torunn Janbu og Helsedirektoratet i sin helhet her.
Answer from Torunn Janbu, Directorate of Health
Svar fra Torunn Janbu, Helsedirektoratet
The Norwegian Directorate of Health has had an open contact with national and international experts. It also includes members of the Norwegian Gynecological Association (NGF). We are well acquainted with NGF's standpoints. The Norwegian Directorate of Health recently met with representatives from the NGF where they were informed of the process, experts and where we had a good discussion about future cooperation.
Helsedirektoratet har hatt en åpen kontakt med nasjonale og internasjonale eksperter. Det inkluderer også medlemmer av Norsk gynekologisk forening (NGF). Vi er godt kjent med NGFs standpunkter. Helsedirektoratet hadde nylig møte med representanter fra NGF hvor de ble informert både om prosessen, eksperter og hvor vi hadde en god diskusjon om fremtidig samarbeid.
The Directorate of Health's mission from the Ministry of Health and Care Services (last autumn) was to present a recommendation on which tool is the most precise and research-based tool.
Helsedirektoratets oppdrag fra Helse- og omsorgsdepartementet (i fjor høst) var å legge frem en anbefaling om hvilket verktøy som er det mest presise og forskningsbaserte verktøyet.
There is a need for one national method for determining birth term. Today we have two (eSnurra and Terminhjulet) that yield different results. The Abortion Act is an important justification for one method. It sets the limit for late abortion to gestational age of 21 weeks and 6 days. It may not be that if the abortion is granted or not, it will depend on where you live in the country and which term tool is used. Term determinations also affect decisions and follow-up of premature babies and post-term pregnancies.
Det er behov for én nasjonal metode for å bestemme fødetermin. I dag har vi to (eSnurra og Terminhjulet) som gir forskjellige resultater. Abortloven er en viktig begrunnelse for én metode. Den setter grensen for seinabort til svangerskapslengde 21 uker og 6 dager. Det kan ikke være slik at om aborten blir innvilget eller ikke, skal avhenge av hvor i landet du bor og hvilket terminbestemmelsesverktøy som brukes. Terminbestemmelse har også betydning for avgjørelser og oppfølging av for tidlig fødte barn og overtidige svangerskap.
eSnurra is a population-based robust method and developed after measurements of about 40,000 women while the Termin wheel was developed after examination of 650 selected women. These methods have widely different statistical properties.
eSnurra er en populasjonsbasert robust metode og utviklet etter målinger på omtrent 40 000 kvinner mens Terminhjulet er utviklet etter undersøkelse av 650 selekterte kvinner. Disse metodene har vidt forskjellige statistiske egenskaper.
The guide to NGF does not point out which tool to use, but opens up the use of different methods for determining the term. It does not match the law for abortion-seeking women.
I veilederen til NGF tar man ikke standpunkt hvilket verktøy som skal brukes, men åpner for bruk av forskjellige metoder for å bestemme termin. Det gir ikke likhet for loven for abortsøkende kvinner.
To be on a safe scientific basis, the Directorate of Health ordered a summary of publications from the Knowledge Center. They concluded in meetings and letters with a procedure that we have followed:
"After an overall assessment, it seems unlikely that a systematic overview carried out in accordance with the Knowledge Center's method handbook will help to highlight the problem beyond what is already known. When the Directorate of Health determines which prediction model should be used to estimate the pregnancy length and term, it seems reasonable to base the decision on the findings presented in Inger Økland's doctoral thesis."
For å være på trygg vitenskapelig grunn, bestilte Helsedirektoratet en oppsummering av publikasjoner fra Kunnskapssenteret. De konkluderte i møter og brev med en fremgangsmåte som vi har fulgt:
"Etter en helhetsvurdering virker det lite sannsynlig at en systematisk oversikt gjennomført i tråd med Kunnskapssenterets metodehåndbok vil bidra til å belyse problemstillingen utover det som allerede er kjent. Når Helsedirektoratet skal beslutte hvilken prediksjonsmodell som bør benyttes for å estimere svangerskapslengde og termin virker det følgelig rimelig å basere avgjørelsen på funnene som er presentert i Inger Øklands doktorgradsavhandling."
Økland's PhD thesis from 2012 provides a concrete basis for assessing differences between the methods that have been used: Snurra (phased out in 2007), Terminhjulet and eSnurra. The methods are validated on data from 3 regions (Trondheim, Stavanger and Oppland), totaling 73,409 pregnancies. The midwives who performed the ultrasound measurements all had the same special education and obtained corresponding results in all three places.
Øklands doktorgradsavhandling fra 2012 gir et konkret grunnlag for å vurdere forskjeller mellom metodene som har vært/er i bruk: Snurra (utfaset i 2007), Terminhjulet og eSnurra. Metodene er validert på data fra 3 regioner (Trondheim, Stavanger og Oppland), til sammen 73.409 graviditeter. Jordmødrene som foretok ultralydmålingene hadde alle samme spesialutdannelse og fikk samsvarende resultater alle tre steder.
The old Snurra showed systematic error (bias) with a median prediction error between 2 and 4 days in the lower range of measurements. The tire wheel showed similar systematic errors in the prediction of the term both before and after week 18 (developed in the same method as Old Snurra). Average error was approx. 2 days, most pronounced after week 18; up to 5 days in the upper part of the measuring range, corresponding to week 22. The results were also comparable here for the three geographical populations.
Den gamle Snurra viste systematiske feil (bias) med en median prediksjons feil mellom 2 og 4 dager i det nedre området av målingene. Terminhjulet viste likeartede systematiske feil i prediksjonen av termin både før og etter uke 18 (utviklet på samme metode som gamle Snurra). Gjennomsnittlig feil var ca. 2 dager, mest uttalt etter uke 18; opp mot 5 dager i øvre del av måleområdet, tilsvarende uke 22. Resultatene var også her samsvarende for de tre geografiske populasjonene.
The Directorate of Health has discussed the topic of fetal age in detail as it has been said that the Termin wheel has better fetal age prediction than, for example, eSnurra. In Økland's work based on data from Lillehammer it is shown that age prediction made with eSnurra is best of the three methods. We have requested a presentation of age prediction on data from Stavanger and Trondheim as well, and they show the same. The old Snurra and Terminal Wheel work smoothly, eSnurra preaches age best. The Directorate of Health has not found any scientific evaluation that shows that the Terminal Wheel is better for predicting age than other methods.
Helsedirektoratet har gått detaljert inn på temaet fosteralder da det er blitt påstått at Terminhjulet har bedre fosteraldersprediksjon enn f. eks. eSnurra. I Øklands arbeider basert på data fra Lillehammer er det vist at aldersprediksjon gjort med eSnurra er best av de tre metodene. Vi har bedt om presentasjon av aldersprediksjon på data også fra Stavanger og Trondheim og de viser det samme - den gamle Snurra og Terminhjulet fungerer likeartet, eSnurra predikerer alder best. Helsedirektoratet har ikke funnet noen vitenskapelig evaluering som viser at Terminhjulet er bedre til å predikere alder enn andre metoder.
In Norway, since 1986 we have had a very well-organized offer for routine ultrasound examinations in weeks 17-19 to all pregnant women - something almost 100% is against. Survey with calculation of term and fetal age is mainly done by midwives with the same special education. The practice is documented as valid (validated) in over 70,000 pregnant women from three different places in Norway.
I Norge har vi siden 1986 hatt et meget godt organisert tilbud om rutinemessig ultralydundersøkelse i uke 17-19 til alle gravide – noe nesten 100 % tar i mot. Undersøkelse med beregning av termin og fosteralder gjøres i all hovedsak av jordmødre med samme spesialutdanning. Praksisen er dokumentert som god (validert) på over 70 000 gravide fra tre ulike steder i Norge.
If you were to switch to early-stage measurement (CRL in the first trimester) as the basis for the termination of term and fetal age, such studies would be done by a variety of doctors and midwives and will not be validated at the same quality level as we have today. It is important that investigations are allowed to be verified and validated.
Dersom man skulle gå over til måling tidlig i svangerskapet (CRL i første trimester) som grunnlag for fastsetting av termin og fosteralder, ville slike undersøkelser bli gjort av en rekke ulike leger og jordmødre og vil ikke kunne etterprøves (valideres) på samme kvalitetsnivå som vi har i dag. Det er viktig at undersøkelser lar seg etterprøve og validere.
There is little knowledge-based assessment of the term and age prediction of the fetus in week 12 and in week 18 of the same population. This should be done before we may leave systematic age prediction in week 18.
Det foreligger lite kunnskapsbasert vurdering av termin og aldersprediksjon av fosteret i uke 12 og i uke 18 på samme populasjon. Dette bør gjøres før vi evt forlater systematisk aldersprediksjon i uke 18.
The Directorate of Health reports that NGF disagrees with the Directorate's conclusion. It is disturbing that NGF does not choose to follow the Directorate-General's scientific reasoned recommendation. The Directorate of Health misses scientific evidence for the claims submitted. Helsedirektoratet registrere at NGF er uenig i direktoratets konklusjon. Det er urovekkende at NGF velger ikke å følge Helsedirektoratets vitenskapelig begrunnede anbefaling. Helsedirektoratet savner vitenskapelig dokumentasjon for de påstander som fremlegges.
The Norwegian Directorate of Health recommends, following a thorough process, that eSnurra is used nationally to determine the duration of pregnancy, birth term and fetal age. Our recommendation is based on solid scientific evidence of what is today the most accurate and research-based tool.
Helsedirektoratet anbefaler etter en grundig prosess at eSnurra brukes nasjonalt til å bestemme svangerskapslengde, fødetermin og fosteralder. Vår anbefaling bygger på solid vitenskapelig dokumentasjon av hva som per dags dato er det mest presise og forskningsbaserte verktøyet.
In a letter of 23.10.2014, the Ministry of Health and Social Affairs has asked the Directorate of Health to "take the necessary measures to implement this recommendation."
Helse – og omsorgsdepartementet har i brev av 23.10.2014 bedt Helsedirektoratet «om å sette i verk nødvendig tiltak for å gjennomføre denne anbefalingen».
(Source: "Gynekologer raser mot Helsedirektoratet" Dagens Medisin SPESIALISTHELSETJENESTE. Anne Grete Storvik. Publisert: 2014-12-08 14.04. Les uttalelsen fra Torunn Janbu og Helsedirektoratet i sin helhet her.)
- Dagens Medisin 2014-12-08 14.04: "Read the statement by Pål Øian and the Norwegian Gynecological Society in full here."
Les uttalelsen fra Pål Øian og Norsk Gynekologisk forening i sin helhet her.
Answer from Pål Øian, Norwegian Gynecological Association (NGF)
Svar fra Pål Øian, Norsk gynekologisk forening (NGF)
It is good that the Directorate of Health reports that NGF disagrees with their conclusion. The Directorate of Health considers that ultrasound testing in weeks 17-19, where the biological variation is quite large, is the only thing to add weight. Information on exact time of fertilization as in assisted fertilization or findings in ultrasound examination early in pregnancy (where biological variation is less) should not be emphasized. This is contrary to well-documented knowledge and international guidelines. The Directorate of Health can not present to us a single new research study or summary of knowledge that was not known to us when we published our revised "Guidelines for Childbirth" earlier this year. It is obvious to us that the Directorate of Health's decision must be based on other motives than evidence-based knowledge. It seems that the Directorate of Health unilaterally emphasizes arguments from the group behind eSnurra. However, they do not take into account research and arguments from the group behind the other method used in Norway (Terminhjulet), by the way, a research group with great international recognition.
Det er bra at Helsedirektoratet registrerer at NGF er uenig i deres konklusjon. Helsedirektoratet mener at ultralydundersøkelse i uke 17-19 der den biologiske variasjon er ganske stor, er det eneste som skal tillegges vekt. Informasjonen om eksakt befruktningstidspunkt som ved assistert befruktning eller funn ved ultralydundersøkelse tidlig i svangerskapet (der biologisk variasjon er mindre) skal ikke vektlegges. Dette er i strid med godt dokumentert kunnskap og internasjonale retningslinjer. Helsedirektoratet kan ikke presentere for oss en eneste ny undersøkelse eller kunnskapsoppsummering som ikke var kjent for oss da vi publiserte vår reviderte «Veileder i fødselshjelp» tidligere i år. Det er åpenbart for oss at Helsedirektoratets beslutning må bygge på andre motiver enn evidensbasert kunnskap. Det kan synes som Helsedirektoratet ensidig legger vekt på argumenter fra gruppen som står bak eSnurra. Derimot tar de ikke hensyn til forskning og argumenter fra den gruppen som står bak den andre metoden som brukes i Norge (Terminhjulet), for øvrig en forskergruppe med stor internasjonal anerkjennelse.
What is critical is that the Directorate of Health have had a process without involving NGF whatsoever. What is clear is that the Directorate of Health has not had dialogue with representatives of NGF. Probably they have talked to gynecologists who are members of NGF but who do not represent NGF.
Det som er kritikkverdig er at Helsedirektoratet har hatt en prosess uten å involvere NGF overhodet. Det som er helt klart er at Helsedirektoratet ikke har hatt dialog med representanter for NGF. Trolig har de snakket med gynekologer som er medlem av NGF, men som ikke representerer NGF.
A week ago, NGF President Jone Trovik and I had a meeting with the Directorate of Health, a meeting held on our initiative. The Directorate of Health's Directorate-General Janbu refused to have a discussion about the scientific basis for the Health Directorate's decision. We also received no information about which people they had talked to during the process, neither in terms of national nor international professionals. This despite the fact that we explicitly asked for this.
For en uke siden var NGF ved leder Jone Trovik og jeg i møte med Helsedirektoratet, et møte som ble avholdt etter initiativ fra oss. Helsedirektoratet, ved nettopp avdelingsdirektør Janbu, avviste da blankt å ha en diskusjon om det vitenskapelige grunnlaget for Helsedirektoratets beslutning. Vi fikk heller ingen informasjon om hvilke personer de hadde snakket med under prosessen, verken når det gjelder nasjonale eller internasjonale fagfolk. Dette til tross for at vi spurte eksplisitt etter dette.
NGF find that the Directorate of Health has handled this case very badly and little confidence in both in terms of process and professional decision. Unfortunately, this is not the first time we have experienced this. We hope the Directorate of Health in the future will show in action, and not only in words, that they want good processes and factual discussion with NGF.
NGF synes at Helsedirektoratet har håndtert denne saken svært dårlig og lite tillitsvekkende, både når det gjelder prosess og faglig beslutning. Det er dessverre ikke første gang vi opplever dette. Vi håper Helsedirektoratet i framtiden viser i handling, og ikke bare i ord, at de ønsker gode prosesser og saklig diskusjon med NGF.
(Source: "Gynekologer raser mot Helsedirektoratet" Dagens Medisin SPESIALISTHELSETJENESTE. Anne Grete Storvik. Publisert: 2014-12-08 14.04. Les uttalelsen fra Pål Øian og Norsk Gynekologisk forening i sin helhet her.)
NGF: Directorate of Health's Recommendation is "highly reprehensible" & "can be directly dangerous"
Included below (emphasis added) is the NGF article: "NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin" written in response to the Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. The article was authored by: Jone Trovik, Leder i NGF (President of NGF), Rolf Kirschner, Leder Kvalitetsutvalget (Head of Quality Committee) and Pål Øian, Hovedredaktør Veileder i fødselshjelp (Chief Editor: Guidelines in Obstetrics). The article is included in its entirety due to its significance. (Source: NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin, Jone Trovik, Rolf Kirschner, Pål Øian. Norsk gynekologisk forening, Den Norske Legeforening Nyheter, 2014) (Note: The source is in Norwegian; this translation is via Google Translate.)
- NGF disagrees with Directorate of Health's recommendation for determination of gestational length and term
NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin
Directorate of Health (Hdir) has in a press release on 16 October 2014 recommended a method (eSnurra) be used to determine gestational length and term. The rationale is that it would ensure an equitable health care across the country, especially in relation to the application for abortion, prematurity and assessment of overtime and growth anomalies.
Helsedirektoratet (Hdir) har i en pressemelding 16. oktober 2014 anbefalt at det skal brukes en metode (eSnurra) for å fastsette svangerskapslengde og termin. Begrunnelsen er at det vil sikre et likeverdig helsetilbud over hele landet, spesielt i forhold til søknad om abort, prematuritet og vurdering av overtid og vekstavvik.
Directorate of Health argues that the decision is rooted in a thorough process that started in autumn 2013 and is based in part on a report from the Knowledge Centre, meetings with specialists and input from national and international expertise.
Helsedirektoratet hevder at avgjørelsen er forankret i en grundig prosess som startet høsten 2013 og baseres blant annet på en rapport fra Kunnskapssenteret, møter med fagmiljøene og innspill fra nasjonal og internasjonal ekspertise.
The Norwegian Gynecological Association (NGF) has responded both in writing and in a meeting with Hdir on 28 November 2014 on their handling of the matter, both in terms of process, professional decision-making and recommendation. In particular the process was unacceptable in this case.
Norsk Gynekologisk Forening (NGF) har reagert både skriftlig og i møte med Hdir den 28.november 2014 på deres behandling av saken både når det gjelder prosess, faglig beslutningsgrunnlag og anbefaling.
After many years of a positive program of scientific dialogue, experiencing the medical specialty association to be overruled. NGF has not been involved in this matter at all. We think this is unacceptable, especially because it is our members who treat patients with issues encompassing abortion, premature birth, growth discrepancies and post-term. During the meeting with Hdir they would not disclose which professionals had been involved, with whom they have had meetings, either nationally or internationally, or the existence of any written assessments from these individuals.
Det er særlig prosessen som er uakseptabel i dette tilfellet. Etter mange års positive opplegg med faglig dialog, opplever den fagmedisinske foreningen å bli overkjørt. NGF har overhodet ikke vært involvert i denne saken. Det synes vi er uakseptabelt, spesielt fordi det er våre medlemmer som behandler pasienter med problemstillinger rundt abort, for tidlig fødsel, vekstavvik og overtid. I møtet med Hdir ville de ikke opplyse om hvilke fagpersoner som har vært involvert og de har hatt møter med, hverken nasjonalt eller internasjonalt eller om det foreligger noen skriftlig vurdering fra disse personene.
Directorate of Health said the case was considered in the Knowledge Centre. There is a two-page response to Directorate of Health in which they conclude that it is unlikely a systematic review carried out in accordance with NOKC's method handbook would help to highlight the issue beyond what was already known. They refer to a Norwegian PhD thesis from 2012.
Hdir sier saken er vurdert i Kunnskapssenteret. Derfra foreligger et tosiders svar til Hdir der de konkluderer med at det er lite sannsynlig at en systematisk oversikt gjennomført i tråd med Kunnskapssenterets metodehåndbok vil bidra til å belyse problemstillingen utover det som allerede er kjent. De viser til en norsk PhD avhandling fra 2012.
Directorate of Health believes that gestational age should be determined on the basis of ultrasound in week 17-19. By exclusively emphasizing ultrasound at this point, natural biological variation is disregarded. Ultrasound in early pregnancy (where the biological variation is less) carried out by a competent person or where we know exactly when conception has taken place (as in assisted reproduction), shall not be taken into account. We believe this is incorrect in relation to good documented knowledge and international guidelines. It also goes against evidence-based recommendations in the newly completed and revised Guidelines in obstetrics 2014.
Hdir mener at svangerskapslengde skal fastsettes ut i fra ultralydundersøkelse i uke 17-19. Ved utelukkende å legge vekt på ultralydundersøkelse på dette tidspunkt, ser man bort fra naturlig biologisk variasjon. Ultralyd tidlig i svangerskapet (der den biologiske variasjon er mindre) utført av kompetent person eller der vi kjenner eksakt når befruktning har foregått (som ved assistert befruktning), skal det ikke tas hensyn til. Dette mener vi er feil i forhold til god dokumentert kunnskap og internasjonale retningslinjer. Det strider også mot kunnskapsbaserte anbefalinger i den nettopp ferdigstilte og reviderte Veileder i fødselshjelp 2014.
In Norway two ultrasound methods were developed and used - one primarily designed to determine gestational age, the other to determine date of delivery. We, as academics, are well experienced in clinical practice. Directorate of Health's recommendation is to use a method that solves none of the clinical problems related to abortion, premature birth, growth abnormalities or post-term. There is far more to take into account than the ultrasound method used.
I Norge er det utviklet og i bruk to ultralydmetoder – den ene primært laget for å bestemme alder på svangerskapet, den andre for å beregne termin. Dette har vi som fagmiljø levd godt med i klinisk praksis. Hdirs anbefaling om å bruke en metode løser ingen av de kliniske problemstillinger knyttet til abort, for tidlig fødsel, vekstavvik eller overtid. Her må langt mer tas hensyn til enn hvilken ultralydmetode som brukes.
Both from a technical and procedural point of view NGF believes that Directorate of Health's handling of this matter is highly reprehensible, does not inspire confidence and unfortunately can be directly dangerous in dealing with difficult clinical issues. NGF will therefore recommend its members to deal with the recommendations given in the Guidelines in obstetrics in 2014 which are based on the best scientific knowledge after a long and thorough process, in which Directorate of Health was also instrumental."
Både fra et faglig og prosessuelt synspunkt mener NGF at Directorate of Health's håndtering av denne saken er sterkt kritikkverdig, lite tillitsvekkende og dessverre kan være direkte farlig i forhold til håndtering av vanskelige kliniske problemstillinger. NGF vil derfor anbefale sine medlemmer å forholde seg til anbefalinger gitt i Veileder i fødselshjelp 2014 som er basert på den beste faglige kunnskap etter en lang og grundig prosess, der også Hdir var medvirkende.
Bergen, Oslo, Tromsø 03.12.14
Jone Trovik Rolf Kirschner Pål Øian
Leder i NGF Leder Kvalitetsutvalget Hovedredaktør Veileder i fødselshjelp
Kopi:
DnL v/ president Hege Gjessing
Helsedirektoratet v/ direktør Bjørn Guldvog
(Source: NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin, Bergen, Oslo, Tromsø 03.12.14, Norsk gynekologisk forening, Nyheter, 2014) (Note: The source is in Norwegian; translation via Google Translate with edits.)
"Directly Dangerous"
NGF's medical experts explicitly warned Directorate of Health of the risks and consequences of their 2014 Recommendation with a government-mandated protocol of evidence-obviated medicine to effect unilateral reliance on NCFM Group's ultrasound-based EDD estimation "method" to establish gestational age for all pregnancies and abortions in Norway. Specifically, NGF warned Directorate of Health that their 2014 Recommendation "can be directly dangerous." The plethora of obstetric and fetal medicine evidence assembled and presented within LailasCase.com proves NGF were, and remain, right.
The following year NGF national representatives coauthored the 16.02.2015 article "The Directorate of Health overrules national, professional guidelines" in Dagens Medisin, Kronikk og debatt. Listed below are the NGF coauthors.
- Jone Trovik, physician at Haukeland University Hospital and President of Norwegian Gynecological Association (NGF)
- Rolf Kirschner, Head of Quality Committee at NGF
- Pål Øian, Chief Editor, Guidelines for obstetrics
- Anne Flem Jacobsen, Editor, Guidelines for obstetrics
- Jørg Kessler, Editor, Guidelines for obstetrics
- "Our gynecological environment devotes considerable effort to prepare well-founded academic supervisors, which health authorities ignore and overrule. For reasons of patient safety, this is very demotivating.
Our gynecological environment devotes considerable effort to prepare well-founded academic supervisors, as health authorities ignoring and over running.For reasons of patient safety, this is very demotivating. - "Ministry of Health sent a request in September 2013 to Directorate of Health asking them to consider what at the time is the most precise and research-based tool "to calculate gestation of pregnancy."
"Helse- og omsorgsdepartementet (HOD) rettet så i september 2013 en henvendelse til Helsedirektoratet (Hdir) og ba dem om å vurdere det til enhver tid mest presise og forskningsbaserte verktøy, «for å beregne svangerskapets varighet». - "Directorate of Health then sent a letter in October 2014 which recommended all gynecologists use a specific ultrasound methodology (eSnurra), exclusively, in weeks 16 to 19. This was determined without any prior contact with the Norwegian Gynecological Association or persons who have been editors for Guidelines in obstetrics. Neither the relevant authors of ultrasound chapter nor Supervisor Board for pregnancy, birth and postnatal care were approached. In a meeting with Hdir in November 2014, we received no documented basis on how the directorate had made such a decision - nor identity of the experts who had been instrumental/contacted. No new method assessments were revealed that were not already known at the time when the Guideline for obstetrics was revised in spring 2014."
Helsedirektoratet sendte så et brev i oktober 2014, der man anbefaler at alle landets gynekologer utelukkende skal benytte en spesifikk ultralydmetodikk (eSnurra), utført i 16-19. uke. Dette er bestemt uten noen forutgående kontakt med Norsk Gynekologisk Forening eller personene som har vært redaktører for Veileder i fødselshjelp. Verken de aktuelle forfattere av ultralydkapittelet eller Fagråd for svangerskaps-, fødsels- og barselomsorg er kontaktet. I et møte med Hdir i november 2014 fikk vi ikke fremlagt dokumentasjon på hvilket grunnlag direktoratet hadde fattet et slikt vedtak – eller hvilke eksperter som hadde vært medvirkende/kontaktet. Det ble ikke vist til noen nye metodevurderinger som ikke allerede var kjent på tidspunktet da Veileder for fødselshjelp ble revidert våren 2014. - "At the time of the routine ultrasound in weeks 16 to 19 eSnurra and Terminhjulet show little difference in dating (0.88 days) when measuring biparietal diameter (BPD). This difference is quite insignificant, given the underlying biological variation, namely that fetuses of the same age may actually have different ultrasound measurements. Please refer to the article's illustration."
På tidspunkt for rutineultralyd i uke 16–19 viser eSnurra og Terminhjulet liten forskjell i datering (0.88 dag) når en måler hodemålet biparietal diameter (BPD). Denne forskjellen er helt betydningsløs, gitt den underliggende biologiske variasjonen, nemlig at foster med samme alder faktisk kan ha ulikt ultralydmål. Det henvises til artikkelens illustrasjon.
(Source: "Directorate of Health overrides national professional counselors" ("Helsedirektoratet overkjører nasjonale faglige veiledere") Kronikk og debatt, Dagens Medisin, Published: 2015-02-16 13.14 Written by: Jone Trovik / Rolf Kirschner / Pål Øian / Anne Flem Jacobsen / Jørg Kessler)
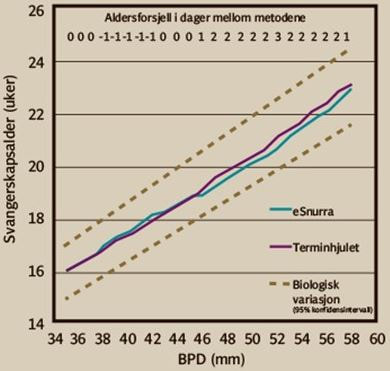
GRAPHIC: BPD-verdien er hentet fra eSnurra og Terminhjulet respektivt, 95% konfidensintervall
fra Papageorghiou, A.T et al. (2014). – Lancet, 384(9946), 869-879. (GRAFIKK: Per Corneliussen)
fra Papageorghiou, A.T et al. (2014). – Lancet, 384(9946), 869-879. (GRAFIKK: Per Corneliussen)
"What a Diff'rence a Day Makes"
It is interesting to note NGF authors pointed out, via an excellent graphic, that 0.88 days difference is "quite insignificant" when measuring biparietal diameter (BPD). It is also interesting to note this exact same point had been made previously by NCFM Snurra Group; twice by Tunón, Eik-Ness and Grøttum in 2 of their NCFM Snurra Group papers: Tunón et al. 1998 and Tunón et al. 1999 (excerpts below).
Others Also Warned Directorate of Health of the Risks & Consequences
It is important to note in addition to NGF and Bergen Group, others published public warnings of the risks and consequences of Directorate of Health's medically & ethically flawed 2014 Recommendation. For example, Dr. Dag Bratlid's 2016 article "Estimating date of delivery and gestational age – technology, biology or both?" ("Bestemmelse av termin og fosteralder – teknologi, biologi eller begge deler?") calls for an evidence-based medicine protocol in which all available information is considered.
NGF and Others Were Excluded from Decision-making Process
NGF made it clear Directorate of Health conducted their decision-making process to select NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, intentionally misused Hutchon Method of PDEE) behind closed doors with the alleged participation of national and international experts; experts Directorate of Health refuses to identify. Moreover, Directorate of Health refuses to share any assessments these alleged national and international experts may have provided. If there had been independent, valid national and international assessments, then Directorate of Health's subversive operation, headed by Jens Grøgaard, colloquially known as "the fix," would not have been necessary. See "The Fix"
NGF: Neither Agreement on Academic Basis nor Decision-making Process for eSnurra Recommendation
Conscious Disregard of the Risks & Consequences
Directorate of Health excluded NGF from the decision-making process and ignored the explicit, published warnings of the risks and consequences identified by NGF, just as Directorate of Health ignored the explicit, published warnings of the risks and consequence by Bergen Group. Consequently, Directorate of Health acted in conscious disregard of the risks and consequences identified by Norway's obstetric & fetal medicine experts when they implemented their science-banding, knowledge-obviated, medically & ethically flawed 2014 Recommendation. Not only did Directorate of Health and NCFM eSnurra Group ignore the Health Technology Assessment (HTA) process and and NOKC's published guidelines for "Ethics in Health Technology Assessment, they also ignored (i.e., violated) the Precautionary Principle. Moreover, given the fact the consequences included actual grievous harms, this was a criminal act. Additionally, Directorate of Health's "omission to act" (i.e., failure to act on their knowledge of experts' warnings of the risks and consequences (Expected Harms = Risks x Consequences) which were made known to Directorate of Health by Norway's medical experts (NGF & Bergen Group), is well established in Norwegian law.
See "The Fix"
It is interesting to note NGF authors pointed out, via an excellent graphic, that 0.88 days difference is "quite insignificant" when measuring biparietal diameter (BPD). It is also interesting to note this exact same point had been made previously by NCFM Snurra Group; twice by Tunón, Eik-Ness and Grøttum in 2 of their NCFM Snurra Group papers: Tunón et al. 1998 and Tunón et al. 1999 (excerpts below).
- "The difference in day of delivery according to ultrasound for the various factors was in the range of 1 day which must be considered to be of negligible clinical importance." (Source: "The impact of fetal, maternal and external factors on prediction of the day of delivery by the use of ultrasound" K. Tunon, S. H. Eik-Nes and P. Grøttum. Ultrasound Obstet Gynecol 1998;11:99-103, p. 102)
- "Such a shift of 3 days may be caused by the BPD being 1–2 mm smaller than the median. Consequently, small but genetically normal fetuses introduce only a small error in the prediction of gestational age; this error is clinically insignificant." (Source: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" K. Tunon, S. H. Eik-Nes and P. Grøttum. Ultrasound Obstet Gynecol 1999;14:17-22, p. 22)
Others Also Warned Directorate of Health of the Risks & Consequences
It is important to note in addition to NGF and Bergen Group, others published public warnings of the risks and consequences of Directorate of Health's medically & ethically flawed 2014 Recommendation. For example, Dr. Dag Bratlid's 2016 article "Estimating date of delivery and gestational age – technology, biology or both?" ("Bestemmelse av termin og fosteralder – teknologi, biologi eller begge deler?") calls for an evidence-based medicine protocol in which all available information is considered.
- "A national standard for estimating date of delivery and gestational age must include both technological and biological information. Ultrasound-based methods such as Terminhjulet or eSnurra will, when used together with a good clinical assessment of menstrual history, provide pregnant women with a better prediction of date of delivery than either approach used alone." (Source: Comment and Debate: "Estimating date of delivery and gestational age – technology, biology or both?" ("Bestemmelse av termin og fosteralder – teknologi, biologi eller begge deler?") Dag Bratlid. Tidsskr Nor Legeforen nr. 16, 2016; 136, p. 1332)
- "Moreover, an ultrasound-based EDD will always be wrong because it relies on the impossible assumption that all fetuses are the same size at the time of the ultrasound examination (2). This means that women whose fetuses are larger or smaller than average will receive erroneous over- or underestimates of fetal age. When a fetus is slightly smaller than average, the ultrasound examination will interpret the pregnancy as less advanced than is actually the case, and the EDD will be pushed further into the future. Similarly, if the fetus is larger than average, the pregnancy will be considered more advanced than it really is, and an earlier EDD will be indicated." (Source: ibid.)
- "Moreover, there has been little discussion of the fact that there are major differences between departments with respect to how they handle discrepancies between clinical and technological EDDs. Some departments consistently show a complete disregard for the EDD entered by the GP on the health card, and often do not add this date to the ultrasound records either. Other departments attach varying degrees of importance to the biological EDD when deciding upon the final EDD. This should of course be standardised." (Source: ibid.)
NGF and Others Were Excluded from Decision-making Process
NGF made it clear Directorate of Health conducted their decision-making process to select NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, intentionally misused Hutchon Method of PDEE) behind closed doors with the alleged participation of national and international experts; experts Directorate of Health refuses to identify. Moreover, Directorate of Health refuses to share any assessments these alleged national and international experts may have provided. If there had been independent, valid national and international assessments, then Directorate of Health's subversive operation, headed by Jens Grøgaard, colloquially known as "the fix," would not have been necessary. See "The Fix"
NGF: Neither Agreement on Academic Basis nor Decision-making Process for eSnurra Recommendation
- "Term Determination
Final report of meetings with the Directorate of Health
NGF has been in contact with the Directorate of Health twice after publishing its recommendation that only eSnurra should be used in the second trimester for term determination. Our understanding of both the academic basis and the decision-making process is so different from the Directorate of Health that even writing a final report (see link) from the last meeting on April 17, 2015 has taken over four months. The board of NGF is not unaware that some departments have changed their routines with respect to ultrasound method. We would still recommend that you relate to the current Supervisor in Birth Aid."
See the minutes (in English & Norwegian) here >>; See the minutes (original file, in Norwegian) here >>.
Terminbestemmelse
Endeleg referat frå møter med Helsedirektoratet
NGF har vært i møte med Helsedirektoratet to ganger etter de publiserte sin anbefaling om at kun eSnurra i andre trimester skulle brukes for terminbestemmelse. Vår forståelse av både faglig grunnlag for og selve beslutningsprosessen er så vidt forskjellig fra Helsedirektoratets at selv det å fremformulere et endelig referat (se link) fra sist møte 17. april 2015 har tatt over fire måneder. Styret i NGF er fortsatt ikke kjent med at noen avdelinger har endret sine rutiner mhp ultralydmetode. Vi vil fortsatt anbefale at man forholder seg til gjeldende Veileder i Fødselshjelp.
Sjå referatet her >>
(Source: "Terminbestemmelse: Endeleg referat frå møter med Helsedirektoratet" Den norske legeforening, Norsk gynekologisk forening (NGF) 18. september 2015)
Conscious Disregard of the Risks & Consequences
Directorate of Health excluded NGF from the decision-making process and ignored the explicit, published warnings of the risks and consequences identified by NGF, just as Directorate of Health ignored the explicit, published warnings of the risks and consequence by Bergen Group. Consequently, Directorate of Health acted in conscious disregard of the risks and consequences identified by Norway's obstetric & fetal medicine experts when they implemented their science-banding, knowledge-obviated, medically & ethically flawed 2014 Recommendation. Not only did Directorate of Health and NCFM eSnurra Group ignore the Health Technology Assessment (HTA) process and and NOKC's published guidelines for "Ethics in Health Technology Assessment, they also ignored (i.e., violated) the Precautionary Principle. Moreover, given the fact the consequences included actual grievous harms, this was a criminal act. Additionally, Directorate of Health's "omission to act" (i.e., failure to act on their knowledge of experts' warnings of the risks and consequences (Expected Harms = Risks x Consequences) which were made known to Directorate of Health by Norway's medical experts (NGF & Bergen Group), is well established in Norwegian law.
- The General Civil Penal Code
"Part I. General Provisions
Introductory Provisions
Section 4. Wherever this code uses the word act, it thereby also includes omission to act unless it is otherwise expressly provided or evident from the context. (Source: "Act of 22 May 1902 No. 10, The General Civil Penal Code" With subsequent amendments, the latest made by Act of 21 December 2005 No. 131. Det Kongelige Justis- Og Politidepartment, Ministry of Justice and the Police. p. 6)
See "The Fix"
Included below is the interview with Torvid Kiserud, MD, PhD, leader of Bergen Group from the 24 April 2018 article in FORSKNING.NO titled "Different methods for calculating when a baby is to be born creates trouble for both research and fetal care"; "Ulike metoder for å regne ut når en baby skal bli født skaper trøbbel for både forskning og foster"
Included below are comments attributed to Håkon K. Gjessing of NCFM Group and first author of Gjessing et al. 2007 from the 24 April 2018 article in FORSKNING.NO titled "Different methods for calculating when a baby is to be born creates trouble for both research and fetal care"; "Ulike metoder for å regne ut når en baby skal bli født skaper trøbbel for både forskning og foster"
- "Many women have a very good overview of menstruation"
– Mange kvinner har veldig god oversikt over mensen
One of the objections to placing a lot of weight on menstruation when calculating the term is that cycles have different lengths, ovulation does not necessarily come after 14 days, and not everyone can answer accurately when they received their the last menstrual period before pregnancy.
En av innvendingene til å legge mye vekt på mensen når man beregner termin, er at sykluser har forskjellig lengde, eggløsninger kommer ikke nødvendigvis etter 14 dager, og ikke alle kan svare skråsikkert på når de fikk mensen for siste gang før graviditeten.
But quite a few can actually do that, says Torvid Kiserud, Professor at the Clinical Institute at the University of Bergen. He is behind the development of the Terminhjulet method, which is used in Oslo, Tromsø and Bergen.
Men ganske mange kan faktisk det, mener Torvid Kiserud, professor ved Klinisk institutt på Universitetet i Bergen. Han står bak utviklingen av metoden Terminhjulet, som brukes i Oslo, Tromsø og Bergen.
"Many women today have control with a calendar, usually have APPs and can monitor their own menstruation quite well," he says.
– Mange kvinner i dag har kontroll med kalender, har gjerne apper og kan monitorere sin egen menstruasjon ganske godt, sier han.
There is no scientific evidence that ultrasound is better than certain, documented regular last menstrual period, according to the UiB professor.
Det er ikke vitenskapelig belegg for at ultralyd er bedre enn certain dokumentert regelmessig siste menstruasjon, ifølge UiB-professoren.
"How great a difference in risk will this pose for the child, when one calculates the term and the age from the last menstruation and from ultrasound?"
– Hvor stor forskjell vil det utgjøre for risikoen for barnet, og man beregner termin og alder ut ifra siste menstruasjon og ut ifra ultralyd?
"In countries with low mortality around birth we depend on large data to respond to such a registry. If you shift the term somewhat, your risk profile may look different in the population. And in this context, someone in the registry has to say if one should use the last menstrual period to calculate the term or whether one should uses ultrasound."
– I land med lav dødelighet rundt fødselen er vi avhengig av store data for å svare på slikt, det vil si et register. Hvis du forskyver termin noe, vil risikoprofilen kunne se annerledes ut i befolkningen. Og i denne sammenhengen har det noen å si om man i registeret bruker siste mens til å beregne termin eller om man bruker ultralyd.
"That is why the researchers have focused on this in the new article. We must be aware of what we use as a basis for age determination of the fetus. Because if you have a child that grows a little and the woman knows exactly when she had the last menstrual period, when she had ovulation and intercourse just after ovulation, one can make a serious mistake by basing the age determination on ultrasound."
– Det er derfor forskerne har satt fokus på dette i den nye artikkelen. Vi må være klar over hva vi bruker som grunnlag for aldersbestemmelse på fostret. For hvis du har et barn som vokser lite og kvinnen vet akkurat når hun hadde siste mens, når hun hadde eggløsning og samleie like etter eggløsning, så kan en gjøre en alvorlig feil ved å bygge aldersbestemmelsen på ultralyd.
"The child is incorrectly classified as younger. Then it will be a system error," says Kiserud.
– Barnet blir feilaktig klassifisert som yngre. Da blir det egentlig en systemfeil, sier Kiserud.
"We must use all available information if it is necessary to determine the age of the fetus as accurately as possible. It is more important than the term when something is at stake."
– Vi må bruke all tilgjengelig informasjon hvis det trengs for å sikrest mulig bestemme fosterets alder. Det er viktigere enn termin når noe står på spill. (Source: "Different methods for calculating when a baby is to be born creates trouble for both research and fetal care"; "Ulike metoder for å regne ut når en baby skal bli født skaper trøbbel for både forskning og foster" Marianne Nordahl. FORSKNING.NO PUBLISHED April 24. 2018)
Included below are comments attributed to Håkon K. Gjessing of NCFM Group and first author of Gjessing et al. 2007 from the 24 April 2018 article in FORSKNING.NO titled "Different methods for calculating when a baby is to be born creates trouble for both research and fetal care"; "Ulike metoder for å regne ut når en baby skal bli født skaper trøbbel for både forskning og foster"
- "The date of last menstruation is a core variable in the Medical Birth Register, and it has laid the foundation for many of the large and solid studies that have come from the register over the years," says Håkon Gjessing.
– Dato for siste menstruasjon er en kjernevariabel i Medisinsk fødselsregister, og den har ligget til grunn for veldig mange av de store og solide studiene som er kommet fra registeret gjennom årene, sier Håkon Gjessing.
"There's probably a tendency to think it's less important to report the last menstrual period when you have ultrasound, but in research, last menstrual period may be equally important."
Det er nok en tendens til å tenke at det er mindre viktig å rapportere siste mens når man har ultralyd, men i forskning kan siste mens være like viktig.
Gjessing agrees that the date of last menstrual period must be included, but he believes it is difficult to give it a formal role in the term setting itself.
Gjessing er enig i at datoen for siste mens må med, men han mener det er vanskelig å gi den en formell rolle i selve terminsettingen.
"The last menstrual period is unfortunately difficult to use in individual dating since it can sometimes be very wrong - there is great individual uncertainty and it can be difficult to know in advance what pregnancies can be incorrectly dated with the last menstrual period."
– Siste mens er dessverre vanskelig å bruke i individuell datering siden den noen ganger kan være veldig feil – det er stor individuell usikkerhet, og det kan være vanskelig å vite på forhånd hvilke svangerskap som kan bli feildatert med siste mens.
But if a doctor or midwife finds one age for the fetus when calculating it from the last menstrual period and another when calculating it with ultrasound, this is a warning signal. Then mother and fetus may have to be carefully monitored to determine if the child grows and develops as it should, according to Gjessing.
Men hvis lege eller jordmor finner én alder på fosteret når de beregner den ut ifra siste mens og en helt annen når de beregner den med ultralyd, er dette et varselsignal. Da kan det hende at mor og foster må følges nøye for å finne ut om barnet vokser og utvikler seg som det skal, ifølge Gjessing. (Source: "Different methods for calculating when a baby is to be born creates trouble for both research and fetal care"; "Ulike metoder for å regne ut når en baby skal bli født skaper trøbbel for både forskning og foster" Marianne Nordahl. FORSKNING.NO PUBLISHED April 24. 2018)