NCFM eSnurra Group
"«It can never happen here» has been the traditional saying in Norway when incidents of scientific dishonesty have been disclosed around the world. In a small country with a limited number of medical researchers, traditions for transparency and a strong belief in honesty, there has been a more or less naïve attitude to fraud and research misconduct." (Source: "Research misconduct: lessons to be learned?" Magne Nylenna. Michael 2007;4:7–9. or see PDF)
The Confusion Surrounding NCFM eSnurra Is Significant
The webpage for Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine (Nasjonal behandlingstjeneste for avansert invasiv fostermedisin) states:
Engineered Confusion
One is given the distinct impression that the Norwegian National Center for Fetal Medicine (NCFM) and the Norwegian National Treatment Service for Advanced Invasive Fetal Medicine (Nasjonal behandlingstjeneste for avansert invasiv fostermedisin) are two separate 'national treatment services' located at St. Olavs Hospital HF (Trondheim University Hospital). Apparently, this engineered confusion has been officially recognized and documented by Directorate of Health in their Evaluering av nasjonal- og flerregional behandlingstjenester 2014 (Evaluation of national and multi-regional treatment services 2014).
Obvious Questions: Since NCFM/NSFM "was formally shut down July 7, 2011," is NCFM/NSFM operating as a rogue or private, virtual medical group outside the authority of Directorate of Health and Ministry of Health and Care Services? If NCFM/NSFM was "formally shut down July 7, 2011," as stated in Directorate of Health's "Evaluering av nasjonal- og flerregional behandlingstjenester 2014", for whom do the 38 employees identified on the NSFM website work, and from whose budget(s) are they paid? Is it possible Sturla H. Eik-Nes et al. are appropriating the formally retired NCFM/NSFM brand name to provide brand affiliation or halo benefits to promote their privately copyrighted (© 2007 Eik-Nes, Grøttum og Gjessing) 'eSnurra' product/service? Or, is the NCFM/NSFM name being used as some sort of cover? Again, Directorate of Health states: "When the service itself uses different designations in its annual report, it will confuse the reader." However, this same confusion is understandably amplified "when the service itself uses different designations" within various doctoral theses, academic journals and media channels for the marketing and promotion of the eSnurra "method" using the formally retired NCFM/NSFM brand name. In the absence of an explanation, it would appear this is another case of the tail wagging the dog.
Wikipedia & eSnurra
The 5 excerpts below constitute the Wikipedia entry for "eSnurra":
NCFM eSnurra Group vs. Wikipedia: Ethical Code for Wikipedians
Wikipedia identifies Morten Dreier (see: https://no.wikipedia.org/wiki/Bruker:Mortendreier) as the primary editor of the Wikipedia entry for "eSnurra" (see: https://no.wikipedia.org/w/index.php?title=ESnurra&action=history)." Interestingly, Morten Dreier, prosjektleder IKT, is listed as an employee of NCFM. Moreover, Morten Dreier is an NCFM eSnurra Group coauthor and the developer of the NCFM eSnurra Group's mobile APPs.
eSnurra, NTNU & St Olavs Hospital (Trondheim University Hospital)
There is no information about "eSnurra" on either the NTNU or St Olavs Hospital website.
Apparently, the National Center for Fetal Medicine, NCFM (Nasjonalt senter for fostermedisin, NSFM) announced a name change in 2015 to "Norwegian National Unit for Advanced Intervention and Invasis Therapy in Fetal Medicine" ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin.") Interestingly, the name change had been ordered by Directorate of Health and Ministry of Health and Care in 2011, with NCFM apparently loathe to implement it.
NSFM Website
Also, there is an NSFM website URL: http://www.nsfm.no/ which redirects to St. Olavs website: https://stolav.no/avdelinger/kvinneklinikken/fodeavdelingen/senter-for-fostermedisin-nsfm
However, the 21 NSFM.no webpages listed below do not redirect to: https://stolav.no/avdelinger/kvinneklinikken/fodeavdelingen/senter-for-fostermedisin-nsfm
On the NSFM webpage: http://www.nsfm.no/web/nb/forskning/esnurra/ (item 11 from the list above) "eSnurra" is defined as follows.
On the NSFM webpage: http://www.nsfm.no/web/nb/international-activities/who-senter/ (item 14 from the list above) NSFM's international activities are described as follows:
eSnurra Website (Norwegian) (http://www.nsfm.no/esnurra/). Interestingly, the URL: http://www.nsfm.no/ redirects to St Olavs website, however, the following URLs: http://www.nsfm.no/esnurra/, http://www.nsfm.no/web/nb/forside/ and others do not redirect to the St Olavs website.
eSnura Website (English) (http://www.esnurra.com/)
On the eSnurra Facebook page "eSnurra" is identified as a "Medical Company in Trondheim, Norway" (https://www.facebook.com/pg/esnurra/). Interestingly, the eSnurra Facebook page neither mentions nor identifies any association between eSnurra and the Norwegian National Center for Fetal Medicine (NSFM/NCFM) or St Olavs Hospital (Trondheim University Hospital). Specifically, the National Center for Fetal Medicine's eSnurra website (http://www.nsfm.no/esnurra/) is not identified on the eSnurra Facebook page. In short, "eSnurra" is presented and promoted on its Facebook page as a private, "Medical Company in Trondheim, Norway." which is consistent with the claimed copyright ownership of "eSnurra" by the 3 original members of NCFM eSnurra Group (© eSnurra, Eik-Nes, Gjessing og Grøttum) who were also the 3 supervisors of Inger Økland's 2012 NTNU dr.philos. Thesis.
The webpage for Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine (Nasjonal behandlingstjeneste for avansert invasiv fostermedisin) states:
- "eSnurra is developed by NSFM and in 2014 the Directorate of Health has decided that eSnurra will be the national method for predicting the term." ("eSnurra er utviklet ved NSFM og Helsedirektoratet har i 2014 bestemt at eSnurra skal være nasjonal metode for å predikere termin.") (Source: eRapport Nasjonal behandlingstjeneste for avansert invasiv fostermedisin, Oppgaver og resultat)
- "In October 2014, the Directorate of Health appointed eSnurra as the only approved national method for term determination." ("Helsedirektoratet utpekte i oktober 2014 eSnurra som eneste godkjente nasjonale terminbestemmelsesmetode.") (Source: Wikipedia: https://no.wikipedia.org/wiki/ESnurra; accessed 03.03.2018)
- "National Treatment Service for Advanced Invasive Fetal Medicine performs diagnostics and treatment in sickness conditions during pregnancy. The treatment service includes blood transfusions to the fetus, drainage of abnormal fluid accumulation, and selective and ineffective fetal reduction. The service also includes palliative care in fetal life." ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin driver diagnostikk og behandling ved sykelige tilstander under svangerskap. Behandlingstjenesten omfatter blodtransfusjoner til foster, drenering av unormale væskeansamlinger, og selektiv og uselektiv fosterreduksjon. Tjenesten omfatter også palliasjon i fosterlivet.") (Source: Nasjonal behandlingstjeneste for avansert invasiv fostermedisin 2017)
[Note: There is no mention of ultrasound-based GA or EDD prediction/estimation methods for pregnancy dating.]
Engineered Confusion
One is given the distinct impression that the Norwegian National Center for Fetal Medicine (NCFM) and the Norwegian National Treatment Service for Advanced Invasive Fetal Medicine (Nasjonal behandlingstjeneste for avansert invasiv fostermedisin) are two separate 'national treatment services' located at St. Olavs Hospital HF (Trondheim University Hospital). Apparently, this engineered confusion has been officially recognized and documented by Directorate of Health in their Evaluering av nasjonal- og flerregional behandlingstjenester 2014 (Evaluation of national and multi-regional treatment services 2014).
- "According to the annual report, the Competence Service for Fetal Medicine is part of the National Treatment Service for Advanced Invasive Fetal Medicine. This is wrong. The National Center for Fetal Medicine was formally shut down July 7, 2011. National Treatment Service for Advanced Invasive Fetal Medicine was approved by new regulations and new working rules on the same day. When the service itself uses different designations in its annual report, it will confuse the reader." ("Det fremgår av årsrapport at Kompetansetjeneste for fostermedisin inngår i Nasjonal behandlingstjeneste for avansert invasiv fostermedisin. Dette er feil. Nasjonalt senter for fostermedisin ble formelt lagt ned 7. juli 2011. Nasjonal behandlingstjeneste for avansert invasiv fostermedisin ble godkjent etter ny forskrift og nytt regelverk fra samme dag. Når tjenesten selv bruker ulike betegnelser i sin årsrapport, vil det forvirre leseren.") (Source: Evaluering av nasjonal- og flerregional behandlingstjenester 2014, Navn på tjenesten: Nasjonal behandlingstjeneste for avansert invasiv fostermedisin, Lokalisering: St. Olavs Hospital HF)
- Leger (Doctors) (7)
- Jordmødre (Midwives) (19)
- Administration (9)
- Sosionomer (Social workers) (2) www.nsfm.no/web/nb/om-nsfm/
- Undervisning (Education) (0)
- Informasjon og IKT (Information and Information & Communication Technology) (1)
- TOTAL NCFM Employees (Ansatte) (38)
(Source: NSFM Website: www.nsfm.no/web/nb/om-nsfm/ © 2018 NSFM)
Obvious Questions: Since NCFM/NSFM "was formally shut down July 7, 2011," is NCFM/NSFM operating as a rogue or private, virtual medical group outside the authority of Directorate of Health and Ministry of Health and Care Services? If NCFM/NSFM was "formally shut down July 7, 2011," as stated in Directorate of Health's "Evaluering av nasjonal- og flerregional behandlingstjenester 2014", for whom do the 38 employees identified on the NSFM website work, and from whose budget(s) are they paid? Is it possible Sturla H. Eik-Nes et al. are appropriating the formally retired NCFM/NSFM brand name to provide brand affiliation or halo benefits to promote their privately copyrighted (© 2007 Eik-Nes, Grøttum og Gjessing) 'eSnurra' product/service? Or, is the NCFM/NSFM name being used as some sort of cover? Again, Directorate of Health states: "When the service itself uses different designations in its annual report, it will confuse the reader." However, this same confusion is understandably amplified "when the service itself uses different designations" within various doctoral theses, academic journals and media channels for the marketing and promotion of the eSnurra "method" using the formally retired NCFM/NSFM brand name. In the absence of an explanation, it would appear this is another case of the tail wagging the dog.
Wikipedia & eSnurra
The 5 excerpts below constitute the Wikipedia entry for "eSnurra":
- "eSnurra is a method for calculating term, gestational age and fetal growth developed by Sturla Eik-Nes (NTNU), Per Grøttum (UiO) and Håkon Gjessing (Norwegian Institute of Public Health)." (
"eSnurra er en metode for beregning av termin, gestasjonsalder og fostervekst utviklet av Sturla Eik-Nes (NTNU), Per Grøttum (UiO) og Håkon Gjessing (Folkehelseinstituttet).")
[Note: The eSnurra "method" does not calculate gestational age. The eSnurra "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) predicts/estimates the remaining days until birth/delivery from the date of the ultrasound exam to establish EDD from which gestational age must be calculated using the equivalent of Naegele's rule, in reverse. Moreover, Dr. Hutchon, whose original idea and method of PDEE explicitly stated 3 critically important points in his seminal Hutchon 1998; 3 critically important points NCFM eSnurra Group decided to ignore. Those 3 critically important points are as follows :
1) "The chart is only for estimating the date of delivery. "
2) "Just as Boerhaave was not actually measuring the length of pregnancy, and the word "gestation" is used to describe the measurement of time from the last menstrual period to reflect this, so also there is no pretence that this method is determining fetal age."
3) "The approach mimics, in modern terms, the method originally formulated by Boerhaave. By adopting this approach we do not need to concern ourselves about the length of the cycle nor the certainty of the dates. Provided the fetus can be assessed as normal using other criteria, this chart can be used to provide the best estimate of the date of delivery (EDD)." (Source: "'Back to the Future' for Hermanni Boerhaave' or 'A rational way to generate ultrasound scan charts for estimating the date of delivery'" Hutchon DJR, ObGyn Ultrasound, Obgyn.net 1998: http://www.obgyn.net/obgyn-ultrasound/back-future-hermanni-boerhaave-or-rational-way-generate-ultrasound-scan-charts-estimating-date [Note: URL updated from published original by ObGyn.net])
Dr. Hutchon made it explicitly clear that the prediction/estimation of fetal age is not the same as the prediction/estimation of EDD using the Hutchon Method of PDEE. - "It is based on a Norwegian population material consisting of about 40000 pregnancies. Unlike older models (e.g., Naegel's rule ), eSnurra does not count back to the last menses while then adding a number of days, but calculates remaining time directly based on the fetus's thigh and head diameter measurements."
(Den er basert på et norsk populasjonsmateriale bestående av om lag 40000 graviditeter. I motsetning til eldre modeller (som f.eks Naegeles regel), regner eSnurra seg ikke tilbake til siste mens for så å legge til et antall dager, men beregner gjenværende tid direkte basert på mål av fosterets lårben og hodediameter.)
[Note: NCFM eSnurra is based, entirely, on the appropriated, plagiarized, misused Hutchon Method of Population-based Direct EDD Estimation (PDEE), i.e., the original idea and method of Dr. David J. R. Hutchon (Hutchon 1998).] - "eSnurra is based on the older Snurra model, which has been standard in Norway since 1984."
("eSnurra bygger på den eldre modellen Snurra, som har vært standard i Norge siden 1984.")
[Note: Again, NCFM eSnurra is based, entirely, on the appropriated, plagiarized, misused Hutchon Method of Population-based Direct EDD Estimation (PDEE), i.e., the original idea and method of Dr. David J. R. Hutchon (Hutchon 1998). Moreover, the "older Snurra model" is based on Stuart Campbell's Method of Gestational Age Estimation (Campbell 1969), which is a completely different prediction/estimation method with a completely different objective than the Hutchon Method of PDEE. Consequently, the NCFM eSnurra "method" is not "based on the older Snurra model" and anyone who claims otherwise is engaging in a conflate-to-obfuscate strategy for the purpose of bending policy-relevant science. The NCFM eSnurra "method" is an implementation of the Hutchon Method of Population-based Direct EDD Estimation (Hutchon 1998) just as the old NCFM Snurra method was an implementation of the Stuart Campbell Method of Gestational Age Estimation (Campbell 1969). Consequently, NCFM eSnurra Group's Wikipedia entry for "eSnurra" is an engineered exercise of conflate-to-obfuscate for the purpose of bending policy-relevant science and to obscure the true origins of the PDEE method.] - "In October 2014, the Directorate of Health appointed eSnurra as the only approved national term determination method."
("Helsedirektoratet utpekte i oktober 2014 eSnurra som eneste godkjente nasjonale terminbestemmelsesmetode.")
[Note: Directorate of Health's knowledge-obviated, science-bending, medically & ethically flawed 2104 Recommendation is a national medical policy for obstetric & fetal medicine which was implemented against the explicit, published warnings of the risks and consequences identified by Norway's obstetric & fetal medicine experts; a flawed national medical policy which implemented the suboptimal, unilateral ultrasound-based pregnancy-dating "method"of NCFM eSnurra Group within a government-mandated protocol of evidence-obviated medicine; a protocol which causes suboptimal obstetric & fetal awareness, which causes suboptimal obstetric & fetal management, which is proven to cause increased medical risks, critical medical mistakes, and grievous medical harms (including perinatal death), unnecessarily, for some of Norway's women and their fetuses/babies.]
- "eSnurra is available as a traditional calculator wheel, as a web-based calculator, as an App for iOS and Android and integrated into the ultrasound device and record systems."
("eSnurra er tilgjengelig som tradisjonelt regnehjul, som web-basert kalkulator, som App for iOS og Android og integrert i ultralydapparater og journalsystemer." (Source: Wikipedia entry for "eSnurra": https://no.wikipedia.org/wiki/ESnurra)
[The gestational age (GA) calculated by NCFM eSnurra Group's eSnurra "method" from the estimated end of pregnancy (i.e., the wrong end) using the equivalent of Naegele's rule, but in reverse, provides different results depending on which NCFM eSnurra Group platform is used (i.e., NCFM eSnurra pregnancy calculator wheel, website, iOS app or Android app).
- eSnurra kalkulator
- eSnurra nettsted
- eSnurra publikasjoner
- eSnurra iOS App
- Helsedirektoratet om esnurra [Norwegian Directorate of Health's 10.12.2014 letter issuing their knowledge-obviated, science-bending, medically & ethically flawed 2104 Recommendation; a national medical policy for obstetric & fetal medicine which was implemented against the explicit, published warnings of the risks and consequences identified by Norway's obstetric & fetal medicine experts; a flawed national medical policy which implemented the suboptimal, unilateral ultrasound-based pregnancy-dating "method"of NCFM eSnurra Group within a government-mandated protocol of evidence-obviated medicine; a protocol which cause suboptimal obstetric & fetal awareness, which causes suboptimal obstetric & fetal management, which causes increased medical risks, critical medical mistakes, and grievous medical harms (including perinatal death), unnecessarily, for some of Norway's women and their fetuses/babies.]
- Helsedirektoratet om valg av terminmetode [Norwegian Directorate of Health's statement regarding: "eSnurra as a method of calculating pregnancy length and term" ("eSnurra som metode for beregning av svangerskapslengde og termin"), included below]
"The Directorate of Health recommends using one method, eSnurra, for the calculation of pregnancy length and term (letter of December 2014, PDF) . eSnurra is the best research-based method, and the most precise tool for evaluation of the term and duration of pregnancy. When using eSnurra, overtime (294 days) will occur 11 days over the estimated term date.
The use of one method nationally ensures abortion-seeking women similarity to the law (avoiding geographical variations), will give a similar assessment of prematurity and unambiguous assessment of premature pregnancies.
eSnurra as a national tool is readily available as a plastic wheel, mobile and tablet app and an open available web version (esnurra.no) .
After making traditional ultrasound measurements of the head and thigh, the data can be used in all modern ultrasound machines." (Source: Directorate of Health's website: https://helsedirektoratet.no/folkehelse/graviditet-fodsel-og-barsel/graviditet-og-svangerskap/overtidige-svangerskap)
NCFM eSnurra Group vs. Wikipedia: Ethical Code for Wikipedians
Wikipedia identifies Morten Dreier (see: https://no.wikipedia.org/wiki/Bruker:Mortendreier) as the primary editor of the Wikipedia entry for "eSnurra" (see: https://no.wikipedia.org/w/index.php?title=ESnurra&action=history)." Interestingly, Morten Dreier, prosjektleder IKT, is listed as an employee of NCFM. Moreover, Morten Dreier is an NCFM eSnurra Group coauthor and the developer of the NCFM eSnurra Group's mobile APPs.
- "Håkon K. Gjessing, Per Grøttum, Inger Økland, J. Morten Dreier and Sturla H. Eik-Nes are the authors of the booklet on the growth calculation method in eSnurra. The booklet is available as PDF, interactive iBook for iPad and soon also for ePub, eBook and other read-only platforms." ("Håkon K. Gjessing, Per Grøttum, Inger Økland, J. Morten Dreier og Sturla H. Eik-Nes er forfatterene av hefte om vekstberegningsmetoden i eSnurra. Heftet er tilgjengelig som PDF, interaktiv iBook for iPad og snart også som ePub eBok for andre lesebrett-plattformer.") (Source: eSnurra Website: http://www.esnurra.no/publikasjoner/esnurra-vekst-metodebeskrivelse/)
- "Neutral Point of View" (NPOV) (https://en.wikipedia.org/wiki/Wikipedia:Neutral_point_of_view),
- "Verifiability" (https://en.wikipedia.org/wiki/Wikipedia:Verifiability) and
- "No original research" (NOR) (https://en.wikipedia.org/wiki/Wikipedia:No_original_research) [However, since NCFM eSnurra Group appropriated, plagiarized and misused Dr. David J. R. Hutchon's original idea, method and research , i.e., the Hutchon Method of PDEE, NCFM eSnurra Group could argue, technically, that Wikipedia's policy of "No original research" was not violated.]
eSnurra, NTNU & St Olavs Hospital (Trondheim University Hospital)
There is no information about "eSnurra" on either the NTNU or St Olavs Hospital website.
- NTNU Website: When one searches for "eSnurra" on the NTNU website, only 2 webpages are returned, the NTNU employee (Ansatte) webpage for Sturla H. Eik-Nes and the NTNU employee (Ansatte) webpage for Harm-Gerd Blass (See: https://www.ntnu.no/sok?query=eSnurra).
- St. Olavs Hospital Website: When one searches for "eSnurra" on the St. Olavs Hospital (Trondheim University Hospital) website, only 1 webpage is returned (see: https://stolav.no/sok?k=eSnurra). The single word "eSnurra" is listed as the last bullet point under the heading "Research" ("Forskning"); just the one word "eSnurra," no description nor additional information of any type. (See: St Olavs Hospital website: Nasjonal behandlingstjeneste for avansert invasiv fostermedisin)
Apparently, the National Center for Fetal Medicine, NCFM (Nasjonalt senter for fostermedisin, NSFM) announced a name change in 2015 to "Norwegian National Unit for Advanced Intervention and Invasis Therapy in Fetal Medicine" ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin.") Interestingly, the name change had been ordered by Directorate of Health and Ministry of Health and Care in 2011, with NCFM apparently loathe to implement it.
- "The Ministry of Health and Care requires that national services use the approved name and offer services in accordance with the description of the content. This also applies to the approved English titles for national treatment services and national competency services." ("Helse- og omsorgsdepartementet forutsetter at nasjonale tjenester bruker det godkjente navn og tilbyr tjenester i hht. beskrivelsen av innholdet. Dette gjelder også for de godkjente engelske titler for nasjonale behandlingstjenester og nasjonale kompetansetjenester.") (Source: Veileder: Nasjonale tjenester i spesialisthelsetjenesten. (National services in specialist health services) Veileder til Forskrift nr. 1706 av 17. desember 2010 om godkjenning av sykehus, bruk av betegnelsen universitetssykehus og nasjonale tjenester i spesialisthelsetjenesten - kapittel 4 - (Revidert 31. januar 2017 ) p. 7)
- Official Norwegian Title: Nasjonal behandlingstjeneste for avansert invasiv fostermedisin
Official English Title: Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine
(Source: ibid., p. 45)
- "The department was the National Center for Fetal Medicine from 1989 to 2015, but had to change its name for formal reasons. The functions, treatments and skills are the same as before the name change."
Avdelingen het Nasjonalt senter for Fostermedisin fra 1989 til 2015, men måtte av formelle årsaker skifte navn. Funksjonene, behandlingene og kompetansen er den samme som før navneskiftet. (Source: St. Olavs website: Nasjonal behandlingstjeneste for avansert invasiv fostermedisin, bottom of page)
NSFM Website
Also, there is an NSFM website URL: http://www.nsfm.no/ which redirects to St. Olavs website: https://stolav.no/avdelinger/kvinneklinikken/fodeavdelingen/senter-for-fostermedisin-nsfm
However, the 21 NSFM.no webpages listed below do not redirect to: https://stolav.no/avdelinger/kvinneklinikken/fodeavdelingen/senter-for-fostermedisin-nsfm
- Velkommen til Nasjonalt senter for fostermedisin (http://www.nsfm.no/web/nb/forside/)
- Ultralyd poliklinikk (http://www.nsfm.no/web/nb/poliklinikk/)
- Fosterdiagnostikk (http://www.nsfm.no/web/nb/fosterdiagnostikk/)
- Undersøkelser (http://www.nsfm.no/web/nb/undersokelser/)
- Tidlig ultralyd (http://www.nsfm.no/web/nb/undersokelser/tidlig_ultralyd/)
- Rutine Ultralyd (http://www.nsfm.no/web/nb/undersokelser/rutine_ultralyd/)
- Sen ultralyd (http://www.nsfm.no/web/nb/undersokelser/sen-ultralyd/)
- Invasive prøver (http://www.nsfm.no/web/nb/undersokelser/invasive-prover/)
- Forskning og undervisning (http://www.nsfm.no/web/nb/forskning/)
- Ultralydstudiet (http://www.nsfm.no/web/nb/forskning/ultralydstudiet/)
- eSnurra (http://www.nsfm.no/web/nb/forskning/esnurra/)
- Umoja (http://www.nsfm.no/web/nb/forskning/umoja/)
- Internasjonalt arbeide (http://www.nsfm.no/web/nb/international-activities/)
- WHO-senter (http://www.nsfm.no/web/nb/international-activities/who-senter/)
- Om nsfm (http://www.nsfm.no/web/nb/om-nsfm/)
- Ansatte (http://www.nsfm.no/web/nb/om-nsfm/ansatte/)
- Introduksjon til eSnurra (http://www.nsfm.no/esnurra/0.php)
- Beregning av gestasjonsalder (GA) (http://www.nsfm.no/esnurra/1.php)
- Beregning av termin ultralyd (TUL) ved rutineundersøkelse (http://www.nsfm.no/esnurra/2.php)
- Beregning av vekst (http://www.nsfm.no/esnurra/3.php)
- Tabeller (http://www.nsfm.no/esnurra/4.php)
On the NSFM webpage: http://www.nsfm.no/web/nb/forskning/esnurra/ (item 11 from the list above) "eSnurra" is defined as follows.
- "eSnurra is the new, population-based methodology for term prediction and growth monitoring which was developed by NSFM. The method is the official method for term prediction and growth monitoring in Norway. Read more at http://www.esnurra.no/"
"eSnurra er den nye, populasjonsbaserte metoden for terminprediksjon og vekstkontroll som er utviklet ved NSFM. Metoden er i dag offisiell metode for terminsetting og vekstkontroll i Norge. Les mer på http://www.esnurra.no/" (Source: NSFM Website: http://www.nsfm.no/web/nb/forskning/esnurra/)
On the NSFM webpage: http://www.nsfm.no/web/nb/international-activities/who-senter/ (item 14 from the list above) NSFM's international activities are described as follows:
- "International work has been an important part of NSFM's work since the early 1990s. We have participated in outreach programs, both in collaboration with ISOUG [sic] and WHO, and have taught and trained midwives and doctors both in field and from our base in Trondheim.
"Internasjonalt arbeid har vært en viktig del av NSFMs arbeid siden tidlig 90-tall. We har deltatt på outreach-programmer både i samarbeid med ISOUG og WHO og har undervist og trent opp jordmødre og leger både i felt og fra vår base i Trondheim." (Source: http://www.nsfm.no/web/nb/international-activities/) - "NSFM has been a WHO teaching and training center since 1996." (Source: http://www.nsfm.no/web/nb/international-activities/who-senter/)
eSnurra Website (Norwegian) (http://www.nsfm.no/esnurra/). Interestingly, the URL: http://www.nsfm.no/ redirects to St Olavs website, however, the following URLs: http://www.nsfm.no/esnurra/, http://www.nsfm.no/web/nb/forside/ and others do not redirect to the St Olavs website.
- "Introduction to eSnurra
eSnurra is the new Norwegian method for term estimation and growth control. Instead of collecting data from a smaller group of pregnant women selected, supposedly, with reliable LMP date and use these data as the basis for the calculation of term and fetal weight, we have built in information from about 40,000 pregnancies into eSnurra. Thus, in the preparation of eSnurra, we have avoided basing ourselves on uncertain information about when the pregnancy started; term is instead calculated from the remaining pregnancy length from ultrasound examination to birth. This process is thoroughly described in the article (ref Gjessing et al. 2007)."
"Introduksjon til eSnurra
eSnurra er den nye, norske metoden for terminprediksjon og vekstkontroll. I stedet for å samle data fra en mindre gruppe selekterte gravide med antatt sikre menstruasjonsdata og bruke disse som grunnlag for beregning av termin og fostervekt, har vi i eSnurra bygd inn opplysninger fra ca 40 000 svangerskap. Dermed har vi i utarbeidingen av eSnurra unngått å basere oss på usikre opplysninger om når svangerskapet startet; termin er i stedet beregnet ut fra gjenværende svangerskapslengde fra ultralydundersøkelse til fødsel. Denne prosessen er grundig beskrevet i artikkelen (ref Gjessing et al.2007)" (Source: Introduksjon til eSnurra, http://www.nsfm.no/esnurra/0.php) - "eSnurra
eSnurra is a new, population based method of determening [sic] the gestational age, the birth term and the weight of a fetus. It is available as an app for iOS, Android and Microsoft mobile, as well as a web version (in norwegian) and as preloaded datasets in ultrasound machines from GE, Siemens, Hitatchi and others. Read more at http://www.esnurra.com/" (Source: http://www.nsfm.no/web/en/research-and-teaching/126-2/)
eSnura Website (English) (http://www.esnurra.com/)
- "What is eSnurra?
eSnurra is a new method for calculating Estimated Date of Delivery(EDD), gestational age and fetal growth. It is based on a Norwegian population material consisting of approximately 40,000 pregnancies. You can use eSnurra in many ways – as “classical” plastic wheel version, a web version, built into a variety of ultrasonic devices as well as apps for iOS, Android, Windows Mobile, and a variety of other formats. eSnurra is an evolution of the old “Snurra” that has been in use in Norway from 1984 until eSnurra came in the first edition in 2007. Snurra has dated about 1.7 million pregnancies in Norway." (Source: http://www.esnurra.com/)
On the eSnurra Facebook page "eSnurra" is identified as a "Medical Company in Trondheim, Norway" (https://www.facebook.com/pg/esnurra/). Interestingly, the eSnurra Facebook page neither mentions nor identifies any association between eSnurra and the Norwegian National Center for Fetal Medicine (NSFM/NCFM) or St Olavs Hospital (Trondheim University Hospital). Specifically, the National Center for Fetal Medicine's eSnurra website (http://www.nsfm.no/esnurra/) is not identified on the eSnurra Facebook page. In short, "eSnurra" is presented and promoted on its Facebook page as a private, "Medical Company in Trondheim, Norway." which is consistent with the claimed copyright ownership of "eSnurra" by the 3 original members of NCFM eSnurra Group (© eSnurra, Eik-Nes, Gjessing og Grøttum) who were also the 3 supervisors of Inger Økland's 2012 NTNU dr.philos. Thesis.
(Source: eSnurra Facebook page: https://www.facebook.com/pg/esnurra/)
The only "Contact" website identified on the eSnurra Facebook page is that of the eSnurra "Medical Company": http://www.esnurra.no/, and the only contact email address identified is that of the eSnurra "Medical Company": [email protected]. The National Center for Fetal Medicine's eSnurra website (http://www.nsfm.no/esnurra/) is not identified on the eSnurra Facebook page. However, and quite strangely, the telephone number (72 57 59 25) identified as the contact telephone number in the "Contact" section of the eSnurra Facebook page is the phone number to the "National Treatment Service for Advanced Invasive Fetal Medicine" ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin") at St Olavs Hospital (Trondheim University Hospital): https://stolav.no/avdelinger/kvinneklinikken/fodeavdelingen/senter-for-fostermedisin-nsfm. Consequently, it would appear eSnurra, a private "Medical Company in Trondheim, Norway," uses the telephone number and telephone services of the National Treatment Service for Advanced Invasive Fetal Medicine for business purposes. Moreover, this telephone number (72 57 59 25) is answered by an employee of St Olavs Hospital (Trondheim University Hospital), not an employee of the eSnurra "Medical Company in Trondheim, Norway."
(Source: eSnurra Facebook page: https://www.facebook.com/pg/esnurra/about/)
Incredibly Confusing
All of this is incredibly confusing and raises some interesting questions regarding the legal entity and functional entity definitions of: eSnurra, National Center for Fetal Medicine (NCFM/NSFM) and Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine relative to each other and relative to St. Olavs Hospital HF (Trondheim University Hospital), NTNU and Helse Midt-Norge RHF. For example, what are the respective competence and treatment domains of National Center for Fetal Medicine (NCFM/NSFM) and "Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine" ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin.")?
All of this is incredibly confusing and raises some interesting questions regarding the legal entity and functional entity definitions of: eSnurra, National Center for Fetal Medicine (NCFM/NSFM) and Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine relative to each other and relative to St. Olavs Hospital HF (Trondheim University Hospital), NTNU and Helse Midt-Norge RHF. For example, what are the respective competence and treatment domains of National Center for Fetal Medicine (NCFM/NSFM) and "Norwegian National Unit for Advanced Intervention and Invasive Therapy in Fetal Medicine" ("Nasjonal behandlingstjeneste for avansert invasiv fostermedisin.")?
Additionally, Inger Økland's 2012 NTNU dr.philos. Thesis, an ethically and academically compromised document, is promoted on the eSnurra Facebook page. Økland's thesis is the one and only publicly available document used by Directorate of Health to justify their knowledge-obviated, medically & ethically flawed 2014 Recommendation with their exclusive selection and implementation of NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine in the form of unilateral ultrasound-based pregnancy dating.
Source: eSnurra Facebook page: https://www.facebook.com/esnurra/)
|
English Translation
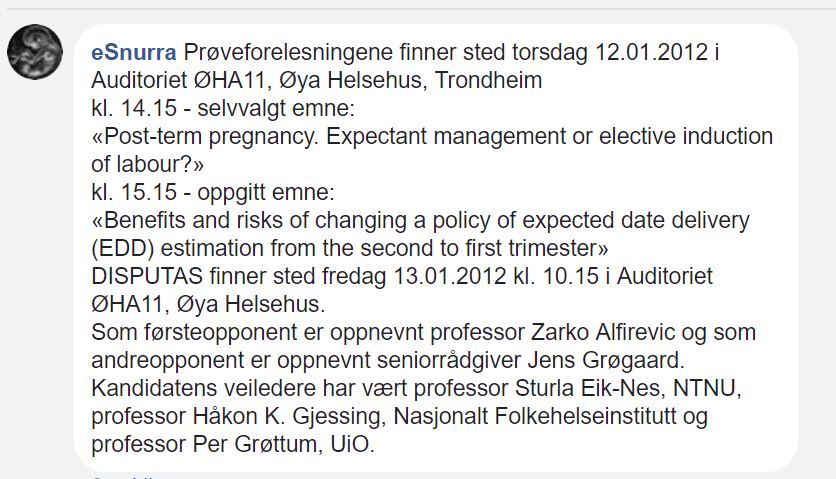
eSnurra The test lectures will take place on Thursday, 12 January 2012 in Auditorium ØHA11, Øya Helsehus, Trondheim at: 14.15 - self-selected topic: «Post-term pregnancy. Expectant management or elective induction of labor?» at: 15.15 - Specified topic: «Benefits and risks of changing a policy of expected date delivery (EDD) estimate from the second to first trimester» DISPUTATION takes place Friday, 13.01.2012 at: 10.15 in Auditorium ØHA11, Øya Helsehus. Professor Zarko Alfirevic is appointed as the first opponent and Senior Adviser Jens Grøgaard is appointed as the second opponent. The candidate's supervisors have been Professor Sturla Eik-Nes, NTNU, Professor Håkon K. Gjessing, National Institute of Public Health and Professor Per Grøttum, UiO. |
Research Misconduct via Plagiarism
The NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, appropriated and plagiarized Dr. Hutchon's original idea and method of Population-based Direct EDD Estimation, from Dr. Hutchon's seminal Hutchon 1998, his other publications, his website, Hutchon.net and, likely, from his manuscript(s). NCFM eSnurra Group claimed Dr. Hutchon's original idea and method of PDEE as NCFM eSnurra Group's own original idea and method, thereby engaging in what is now 13 years of ongoing research misconduct via plagiarism.
Gjessing et al. 2007 cited and referenced Taipale & Hiilesmaa 2001 via citation 22 as follows.
Importantly, when Norway's NCFM Group's Gjessing et al. 2007 cited and referenced Norway's NCFM Group's Taipale & Hiilesmaa 2001, Norway's NCFM Group had cited and referenced themselves. This combined strategy of: 1) self-referencing, 2) fact invention and 3) dead end citation created a provenance barrier to my idea and method of PDEE (Hutchon 1998) within the literature. Taipale & Hiilesmaa 2001 was used as a red herring to distract and mislead from the true provenance chain for the idea and method of PDEE. Norway's NCFM group, headed by Sturla H. Eik-Nes, exploited and continue to exploit Taipale & Hiilesmaa 2001 as a red herring to the true provenance of Dr. Hutchon's idea and method of PDEE in order to claim his original idea and method as their own original idea and method. While citation 22 (or, maybe, Catch-22) in Gjessing et al. 2007 helped to embolden Norway's NCFM Group, headed by Sturla H. Eik-Nes, to engage in long-term, ongoing research misconduct via plagiarism (2001 – Present), it was UOG & ISUOG's complete inaction regarding my letters and other communications of misconduct in Gjessing et al. 2007 that enabled the long-term, ongoing research misconduct via plagiarism by Norway's NCFM Group, headed by Sturla H. Eik-Nes, President ISUOG (1998 – 2002).
To further make the point about citation distortions, consider the excerpt below from Taipale & Hiilesmaa 2001 (p. 192).
Given the stated aim of Taipale & Hiilesmaa 2001 was a methods or metrics comparison study...
The NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, appropriated and plagiarized Dr. Hutchon's original idea and method of Population-based Direct EDD Estimation, from Dr. Hutchon's seminal Hutchon 1998, his other publications, his website, Hutchon.net and, likely, from his manuscript(s). NCFM eSnurra Group claimed Dr. Hutchon's original idea and method of PDEE as NCFM eSnurra Group's own original idea and method, thereby engaging in what is now 13 years of ongoing research misconduct via plagiarism.
Gjessing et al. 2007 cited and referenced Taipale & Hiilesmaa 2001 via citation 22 as follows.
- Citation 22: "Population prediction of remaining time has been used previously only to assess prediction quality 22." (p.23)
- Reference 22: "22. Taipale P, Hiilesmaa V. Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol 2001; 97: 189–194."
- "Dead end citation—support of a claim with citation to papers that do not contain content addressing the claim" (Source: "How citation distortions create unfounded authority: analysis of a citation network" Steven A Greenberg. BMJ 2009;339:b2680)
Importantly, when Norway's NCFM Group's Gjessing et al. 2007 cited and referenced Norway's NCFM Group's Taipale & Hiilesmaa 2001, Norway's NCFM Group had cited and referenced themselves. This combined strategy of: 1) self-referencing, 2) fact invention and 3) dead end citation created a provenance barrier to my idea and method of PDEE (Hutchon 1998) within the literature. Taipale & Hiilesmaa 2001 was used as a red herring to distract and mislead from the true provenance chain for the idea and method of PDEE. Norway's NCFM group, headed by Sturla H. Eik-Nes, exploited and continue to exploit Taipale & Hiilesmaa 2001 as a red herring to the true provenance of Dr. Hutchon's idea and method of PDEE in order to claim his original idea and method as their own original idea and method. While citation 22 (or, maybe, Catch-22) in Gjessing et al. 2007 helped to embolden Norway's NCFM Group, headed by Sturla H. Eik-Nes, to engage in long-term, ongoing research misconduct via plagiarism (2001 – Present), it was UOG & ISUOG's complete inaction regarding my letters and other communications of misconduct in Gjessing et al. 2007 that enabled the long-term, ongoing research misconduct via plagiarism by Norway's NCFM Group, headed by Sturla H. Eik-Nes, President ISUOG (1998 – 2002).
To further make the point about citation distortions, consider the excerpt below from Taipale & Hiilesmaa 2001 (p. 192).
- "It has been suggested that the prediction error between the estimated day of delivery and the actual day of delivery should be 7 to 8 days. 14 In our study, the prediction error at 11–16 weeks’ gestation was 7.3 days for the best ultrasound determinant, when premature deliveries were excluded."
- "The prediction error (SD) should be kept between 7 and 8 days." (Source: "Ultrasound dating of pregnancy—Still controversial?" Persson PH. Ultrasound Obstet Gynecol 1999;14:9–11. p. 11)
- "Citation diversion—citing content but claiming it has a different meaning, thereby diverting its implication" (Source: "How citation distortions create unfounded authority: analysis of a citation network" Steven A Greenberg. BMJ 2009;339:b2680)
- "The mean duration of pregnancy was 278.6 days with standard deviation (SD) of 12.5." (Source: "Predicting delivery date by ultrasound and last menstrual period in early gestation" Taipale P, Hiilesmaa V. Obstetrics & Gynecology 2001; 97: 189–194. p. 190)
- "...estimate which ultrasound measurement, crown-rump length, BPD, or FL, is best for predicting the day of delivery..."
Given the stated aim of Taipale & Hiilesmaa 2001 was a methods or metrics comparison study...
- "The aim of our study was to estimate which ultrasound measurement, crown-rump length, BPD, or FL, is best for predicting the day of delivery at 8–16 weeks' gestation. We also compared them to prediction by certain and uncertain LMP." (Source: "Predicting delivery date by ultrasound and last menstrual period in early gestation" Taipale P, Hiilesmaa V. Obstetrics & Gynecology 2001; 97: 189–194)
- "the ultrasound estimate was the significantly better predictor of day of delivery in 52% of cases, and the last menstrual period estimate was the better predictor in 46% of cases." (Source: Tunón et al. 1996 p. 178)
Figure 1 of Taipale & Hiilesmaa 2001 shows a plot of average prediction error for CRL, BPD, FL and certain LMP on the y-axis, with 6 bins for 6 gestational weeks on the x-axis, with 3 weeks (8w+0 through 10w+6) excluded, without a reason. Nevertheless, if this same plot had been created for the SDs of the prediction errors for CRL, BPD, FL and certain LMP, the information illustrated in the example graphic above would have been available, but a similar SD vs. GA plot was excluded.
Figure 2 of Taipale & Hiilesmaa 2001 does not explain the decision criteria for selecting CRL or BPD for inclusion in the stacked column charts.
A key consideration in a prediction/estimation method, such as NCFM Snurra or the Hutchon Method of PDEE, is not whether the method or the metric(s) deliver a correct GA or EDD prediction/estimation on average, but what the likely error is for GA or EDD assigned to individual pregnancies that is important, especially to pregnant women. What good is a method or fetal metric predictor if it is correct on average but delivers inaccurate or grossly inaccurate GA or EDD predictions/estimations 60% of the time. It is the consideration and discussion of the likely error for individual predictions which is completely missing in Tunón et al. 2000 and Taipale & Hiilesmaa 2001 because standard deviations (SD) of prediction errors (random errors) were not discussed, intentionally. Again, consideration and discussion of the likely errors for individual GA or EDD predictions/estimations assigned to individual pregnancies were excluded, intentionally, in NCFM Snurra Group's Tunón et al. 2000 and Taipale & Hiilesmaa 2001.
Figure 2 of Taipale & Hiilesmaa 2001 does not explain the decision criteria for selecting CRL or BPD for inclusion in the stacked column charts.
- "Figure 2. Comparison between ultrasound (according to crown-rump length or biparietal diameter) and certain last menstrual period 1 280 or 1 282 days in estimating the day of delivery."
- "...estimate which ultrasound measurement, crown-rump length, BPD, or FL, is best for predicting the day of delivery..."
A key consideration in a prediction/estimation method, such as NCFM Snurra or the Hutchon Method of PDEE, is not whether the method or the metric(s) deliver a correct GA or EDD prediction/estimation on average, but what the likely error is for GA or EDD assigned to individual pregnancies that is important, especially to pregnant women. What good is a method or fetal metric predictor if it is correct on average but delivers inaccurate or grossly inaccurate GA or EDD predictions/estimations 60% of the time. It is the consideration and discussion of the likely error for individual predictions which is completely missing in Tunón et al. 2000 and Taipale & Hiilesmaa 2001 because standard deviations (SD) of prediction errors (random errors) were not discussed, intentionally. Again, consideration and discussion of the likely errors for individual GA or EDD predictions/estimations assigned to individual pregnancies were excluded, intentionally, in NCFM Snurra Group's Tunón et al. 2000 and Taipale & Hiilesmaa 2001.
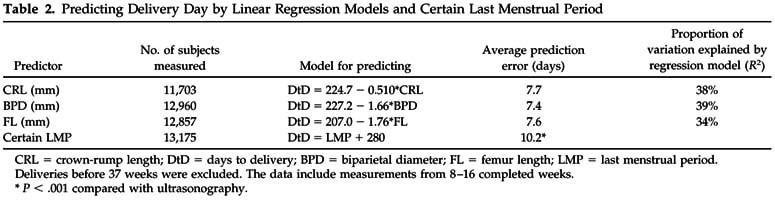
CRL = crown-rump length; DtD = days to delivery; BPD = biparietal diameter; FL = femur length; LMP = last menstrual period.
Deliveries before 37 weeks were excluded. The data include measurements from 8–16 completed weeks.
* P < .001 compared with ultrasonography. (Source: ibid., p. 191)
Deliveries before 37 weeks were excluded. The data include measurements from 8–16 completed weeks.
* P < .001 compared with ultrasonography. (Source: ibid., p. 191)
NCFM eSnurra Group's Taipale & Hiilesmaa 2001 was published 4-years and 6-years prior to NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, while Sturla H. Eik-Nes, founder and leader of NCFM eSnurra Group, was President of ISUOG.
(see Plagiarism > HUTCHON TIMELINE 00.02.2001
Whatever the intent or strategy of NCFM Snurra Group, it was and remains a well-documented fact Dr. Hutchon's original idea and method of PDEE had been published 19.07.1998 in Dr. Hutchon's seminal Hutchon 1998 in OBGYN.net, 2.5 years, 7 years and 9 years before NCFM Snurra/eSnurra Group's Taipale & Hiilesmaa 2001, Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, were published.
Interestingly, the bottom line conclusion of Taipale & Hiilesmaa 2001 was completely consistent with NCFM Snurra Group's agenda of excluding a pregnant woman's key pregnancy dates from medical evidence to ensure unilateral reliance on ultrasound for GA & EDD assignments in the second-trimester, i.e., the routine 18-week ultrasound exam which is widely reported to be less accurate than first-trimester ultrasound and, is completely consistent with NCFM eSnurra Group's current "method' (i.e., an appropriated, plagiarized & misused implementation of Dr. Hutchon's idea and method of PDEE) within a government-mandated protocol of evidence-obviated medicine which obviates all key pregnancy dates, without a pregnant woman's prior, informed, voluntary, explicit consent.
Consider the "Conclusion" presented in the abstract of Taipale & Hiilesmaa 2001 in the excerpt below:
While the statement below speaks for itself with respect to evidence-obviated medicine it is literally the last sentence, the bottom line of the NCFM Snurra Group's recognized, documented collaboration on Taipale & Hiilesmaa 2001, which deserves a modicum of consideration.
NCFM eSnurra Group Claimed the Hutchon Method of PDEE as Their Own Idea & Method
The first sentence of the first page of both the English and Norwegian versions of NCFM eSnurra Group's websites state: "eSnurra is a new method for calculating Estimated Date of Delivery (EDD)"
Interestingly and strangely, in the very first sentence of both their English and Norwegian websites for 'eSnurra', NCFM eSnurra Group state "eSnurra is a new method for calculating (beregning) EDD, GA and fetal growth." What happened to predicting/estimating EDD or GA?
The NCFM eSnurra Group made several patently false statements (emphasis added) in: 1) their Økland et al. 2007, an 08.10.2007 Poster Abstract at the 17th World Congress on Ultrasound in Obstetrics and Gynecology and 2) in NCFM eSnurra Group'S Gjessing et al. 2007.
NCFM eSnurra Group's Medico-Marketing Agenda vs. Medical Science
In her 2012 NTNU dr.philos. Thesis (p. 28 & 44), Inger Økland identified what is required for a population-based model to be validated for a specific population, such as Trondheim vs. Bergen. Also, it states the "the methods must be re-calibrated when the examination practice and the population distribution change," such as when "the methods" are used for a different population within a country (e.g., Trondheim vs. Bergen) or within a different country.
Consider what Eric O. Ohuma and the late Douglas G. Altman had to say about multiple populations in their 2019 paper which "discusses the features of study design and methodological considerations for constructing reference centile charts for attained size, growth, and velocity charts with a focus on human growth charts used during pregnancy."
Nevertheless, and strangely, Directorate of Health stated NCFM eSnurra Group's population-based method (i.e. the appropriated, plagiarized, misused Hutchon Method of PDEE) was "installed in over 90 countries" which, given the population-based model requirements stated in Økland's 2012 NTNU dr.philos. Thesis (above, and the excerpt directly above), this would require: 5 prediction/estimation models per country-population x 90 country-populations = 450 country-population-specific models built from country-population-specific "reference material" collected from country-population-specific, quality-assured historical databases of past pregnancies and then validated. (Source: DEBATT OG KRONIKK "Helsedirektoratets rolle – og eSnurra" Skrevet av: Johan Torgersen / Torunn Janbu. Dagens Medisin. Publisert: 2015-04-13 11.49)
Additionally, accessing NCFM eSnurra Group's website and the NCFM eSnurra Group's APP for Android and iOS from another country appears to be what Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, were referring in their request to NOKC (Forslagsnr: 792, 15.11.2013) on behalf of Ministry of Health & Care Services and Directorate of Health, when they stated:
Consider if NCFM eSnurra Group's population-based "method" with models trained/built on the > 95% White Norway-Trondheim population, were to be used in the Philippines and South Africa, where the populations are < 10% White. Then, consider this in the context of the findings from the "Racial/Ethnic Standards for Fetal Growth, the NICHD Fetal Growth Studies" or Buck Louis et al. 2015, are included below.
The other important take-away point is the fact Directorate of Health were promoting NCFM eSnurra Group's "population-based method" had been "installed in over 90 countries" while, simultaneously, and in the very same article "Helsedirektoratets rolle – og eSnurra, (Referanser: 1)", promoting Økland's 2012 NTNU dr.philos. Thesis as independent, academic justification of their knowledge-obviated, medically & ethically flawed 2014 Recommendation without any consideration or apparent comprehension of that which was stated in Økland's 2012 NTNU dr.philos. Thesis regarding the NCFM eSnurra Group's "population-based method." There are 101 occurrences of the compound adjective "population-based" in Økland's 2012 NTNU dr.philos. Thesis. One would think Directorate of Health would have had a modicum of comprehension of the conflict of interest and the science-bending implications of promoting the medico-marketing point of "installed in over 90 countries." This fact serves as additional evidence in support of an important and, hopefully, now, all-too-obvious point made by Bergen Group:
Excessive Claiming Behavior From One Group of Plagiarists to Another
The extent of NCFM eSnurra Group's efforts to promote and protect their "claim" to Dr. Hutchon's original idea and method, the Hutchon Method of PDEE, is evidenced in the excerpts below, emphasis added. The excerpts are from comments made by NCFM eSnurra Group in a "Comment & Reply Correspondence" in The Journal of Maternal-Fetal & Neonatal Medicine regarding Salomon et al. 2010, coauthored by Yves Ville (see Hutchon Timeline 26.07.2007, 17.09.2007, 21.09 2007, 29.02.2008, 13.02.2009, 11.12.2009) to which Salomon et al. Group replied (included below). NCFM eSnurra Group makes the point, incessantly, that the method of Population-based Direct EDD Estimation is "their method." Maybe Dr. Hutchon could take a modicum of solace in the fact NCFM eSnurra Group so valued the Hutchon Method of PDEE, they defended their illegitimate claim, vociferously, from a perceived encroachment by Salomon et al. 2010 who, incredibly, had also appropriated and plagiarized the Hutchon Method of Population-based Direct EDD Estimation. However, it is important to note Salomon et al. 2010 cited NCFM eSnurra Group's Gjessing et al. 2007, extensively, and Salomon et al. 2010 cited Taipale & Hiilesmaa 2001 which was the result of a recognized NCFM eSnurra Group collaboration. Unfortunately, Dr. Hutchon's seminal Hutchon 1998 was neither cited nor acknowledged by Taipale & Hiilesmaa 2001, or by NCFM eSnurra Group's Eik-Nes et al. 2005 or Gjessing et al. 2007 or by the French Group, Salomon et al. 2010 which included Dr. Yves Ville as a coauthor and who was Editor-in-Chief of Ultrasound in Obstetrics & Gynecology at the time of the plagiarism
NCFM eSnurra Group's Comments to Salomon et al. Group: Excessive Claiming Behavior
Included below is an epic and classic display of excessive claiming behavior of plagiarists, courtesy of NCFM eSnurra Group's Håkon K. Gjessing, Per Grøttum, Inger Økland, & Sturla H. Eik-Nes.
Salomon et al. 2010 Also Plagiarized the Hutchon Method of PDEE
Salomon et al. 2010 also appropriated and plagiarized Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE). Again, it is important to note Salomon et al. 2010 cited NCFM eSnurra Group's Gjessing et al. 2007, extensively. Nevertheless, the "Comment & Reply" exchange is decidedly interesting considering:
Plagiarism & Next-Steps
NCFM eSnurra Group's Gjessing et al. 2007 appear to have made 4 changes to the Hutchon Method of PDEE in their appropriated, plagiarized implementation:
NCFM eSnurra: Black Box Techniques
The NCFM eSnurra disclosure of statistical techniques in Gjessing et al. 2007 demonstrate comparability and reproducability by other researchers is not possible due to their use of custom statistical analysis software which is not available in the major statistical packages used by most researchers, thus creating what is commonly termed a black box model or system, a point well made by Salomon et al. in their "Comment & Reply Correspondence " with NCFM eSnurra Group. In the excerpt below, the phrase "which were verified in part against the quantreg implementation of QR models in R" serves to solidify this point. This may very well explain why after 10-years there is still no evidence NCFM eSnurra Group's models and statistical techniques having been reproduced and verified by independent researchers.
NCFM eSnurra Group Conflates Predicted/Estimated GA with Calculated GA
One can predict/estimate y from x (via y regressed on x; i.e. y depends on x) if the dataset observations include both the x and y variables (x = independent variable; y = dependent variable). Not surprisingly, it is impossible to predict/estimate z from x (via y regressed on x) if the dataset only contains observations of x and y. Both Bergen Group and NCFM eSnurra Group regress on the very same independent x variable, i.e., ultrasound-based measurements of fetal metrics (e.g., BPD, FL, HC, CRL, MAD, etc.). However, these two groups use completely different dependent y variables. The Bergen Group's dependent y variable is gestational age (GA) on the ultrasound date, while the NCFM eSnurra Group's dependent y variable is the number of days remaining from the ultrasound date to birth/deliver. The Bergen Group predicts/estimates GA directly from ultrasound fetal metric measurements and NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) directly predicts/estimates days remaining from ultrasound fetal metric measurements to calculate EDD. Consequently, it is impossible for the Bergen Group to directly predict/estimate EDD and it is impossible for NCFM eSnurra Group to directly predict/estimate GA. However, Bergen Group and NCFM eSnurra Group can each calculate (not predict/estimate) their predicted/estimated complement EDD and GA, respectively, by using a fixed gestation time from LMPD (Bergen Group uses 282 days, NCFM eSnurra Group, 283 days). Consequently, the Bergen Group can subtract the predicted/estimated GA on the ultrasound date from the ultrasound date to calculate a virtual LMPD, and then add 282 days to calculate EDD. And, NCFM eSnurra Group can subtract the predicted/estimated days remaining to delivery on the ultrasound date from 283 days to calculate GA on the ultrasound date. Both Bergen Group and NCFM eSnurra Group depend on the use of a virtual LMPD date to calculate EDD and GA, respectively, and then subtract GA on the ultrasound date from the ultrasound date to calculate a virtual LMPD, respectively. And, because these are calculation methods and not direct prediction/estimation methods from ultrasound measurements, these "calculated" methods are sometimes referred to as "indirect" methods.
To get an idea of NCFM eSnurra Group's conflate-to-obfuscate strategy, consider the excerpt below in the context of the preceding paragraph. NCFM eSnurra Group disparaged "traditional models" or, more specifically, Bergen Group, because Bergen Group does not directly predict/estimate EDD from ultrasound fetal metric measurements and, therefore, must calculate EDD from the LMPD established by their directly predicted/estimated GA. Consequently, and by using NCFM eSnurra Group's own reasoning, NCFM eSnurra Group must also believe they "primarily estimate EDD from second-trimester fetal measurements when they calculate GA, thus, gestational age (GA) "is actually an indirect and secondary issue" for NCFM eSnurra Group. Day-0 (or GA = 0w+0) of the median 283-day "gestation period" set by NCFM eSnurra Group is the virtual LMPD. Moreover, all GA values calculated by NCFM eSnurra Group depend on a virtual LMPD.
In the excerpt below, NCFM eSnurra Group conflate estimates of GA with estimates of EDD. NCFM eSnurra Group's method (i.e. the appropriated, plagiarized, misused Hutchon Method of PDEE) estimates EDD and, therefrom, calculates GA using the equivalent of Naegele's rule. In short, it is not "standard procedure to obtain estimates of the gestational age of the fetus and of the expected day of delivery." This is a conflate-to-obfuscate strategy, trying to communicate the terms estimate and calculate with respect to GA & EDD as synonymous; and, this has worked well because it is clear Directorate of Health is confused by direct estimation of GA and calculation of GA from a direct estimation of EDD to the point of incompetence.
Conflate to Obfuscate
Included in the excerpts below is a good example of NCFM eSnurra Group prosecuting their science-bending agenda with a conflate-to-obfuscate strategy. Specifically, in NCFM eSnurra Group's Eik-Nes et al. 2006 they claimed:
Conflate-to-Obfuscate: predict, estimate & calculate
In the following sections it will become obvious NCFM eSnurra Group works to conflate the words "estimate" and "calculate" with respect to GA & EDD as a conflate-to-obfuscate tactic in order to claim NCFM eSnurra Group possesses GA estimation capability when, in reality, it is not possible for NCFM eSnurra to estimate GA; GA must be calculated from NCFM eSnurra EDD using the equivalent of Naegele's rule, in reverse. Again, conflating the words "estimate" and "calculate" to obfuscate the difference is bending science, which is a large part of NCFM eSnurra Group's agenda, which is bending science for ambition, ideology and policy, not research-based science. In fact, NCFM eSnurra Group's agenda of bending policy-relevant science is more akin to a political party gearing up for an election by crafting and repeating a message that is intentionally confusing. Moreover, this very same science-bending, conflate-to-obfuscate strategy was used by NCFM eSnurra Group to obfuscate the differences between a retrospective (looking back) study and a prospective (looking forward) study. These were clearly intentional acts, evidenced by the deliberate actions of 2 of NCFM eSnurra Group's members who were (and remain) "copyright owners" of NCFM eSnurra:
An Apt Analogy
Hakon K. Gjessing's UiB webpage for his genetic association analyses software package includes the following appeal for ethical propriety with respect to acknowledging, citing and referencing his work and, appropriately so, as there are too many who need to be reminded of the ethical etiquette.
Corrupted Process: NCFM eSnurra Group: Mission Creep to Mission Leap
The objective of the NCFM eSnurra Group study, as explicitly stated in their 2007 paper was clearly defined (excerpt below) by the three NCFM eSnurra Group authors, the three "copyright owners" of NCFM eSnurra (© 2007 EikNes, Grøttum og Gjessing).
It boggles the mind Directorate of Health either misses or ignores the important distinction between actually predicting/estimating fetal age and GA from ultrasound fetal metric measurements (Bergen Group) and calculating fetal age and GA from predictions/estimates of the remaining days until EDD using the equivalent of Naegele's rule, in reverse, (NCFM eSnurra Group). Clearly, the basis for determining fetal age and GA is not the end of the pregnancy, but its beginning, and not from calculations based on predictions/estimates of EDD (NCFM eSnurra Group) but from direct predictions/estimates of GA from fetal metric measurements (Bergen Group).
Conflate-to-Obfuscate: Estimate and Calculate
There were 20 occurrences of the word "estimate" or a derivative thereof in the NCFM eSnurra Group's Gjessing et al. 2007, references section excluded. Interestingly, 30% (or 6 of 20) of these word occurrences were used incorrectly, intentionally, and all of the incorrect uses of the word "estimate" pertained to GA (see excerpts below). This was the conflate-to-obfuscate strategy NCFM eSnurra Group used to launch their mission leap claim of GA estimation capability; a capability that did not exist because it was not (and is not) possible. The first excerpt is interesting in that with respect to "traditional approaches" the authors state: "The estimation methods are solely aimed at computing gestational age." Again, even when referring to the "traditional approach" the authors conflate estimation of gestational age with "computing gestational age." Traditional methods predict/estimate gestational age to establish a predicted/estimated number of days from LMPD to the ultrasound date to establish a predicted/estimated LMPD from which GA is established on the date of the ultrasound, just as NCFM eSnurra Group predict/estimate the number of days remaining from the ultrasound exam to delivery date to establish a predicted/estimated EDD. The reason the "the true problem of prediction of term is hardly ever mentioned, let along made explicit" among those using the "traditional approach" is because predicting/estimating EDD is not possible using the "traditional approach," EDD must be calculated when using the "traditional approach," just as predicting/estimating GA is not possible using the NCFM eSnurra Group's approach (i.e., the appropriated Hutchon Method of PDEE) because GA must be calculated when using the NCFM eSnurra Group's Group's approach (i.e., the appropriated Hutchon Method of PDEE). Consequently, the authors must also believe:
Conflate-to-Obfuscate: Retrospective and Prospective
NCFM eSnurra Group appears to believe because the ultrasound-based fetal metric measurements that comprise their 1987–2004 dataset were made before the actual birth/delivery, that this somehow qualified their study as prospective instead of retrospective. Again, this conflate-to-obfuscate strategy requires temporally-challenged thinking, as it implies NCFM eSnurra Group believe all ultrasound studies on pregnancy, in the world, are therefore prospective because birth/delivery occurs after pregnancy. The thing that makes a prospective study prospective is that it is designed (i.e., hypothesis fully formulated, methods established, etc.) before subjects are enrolled and baseline data are collected and before any subjects develope the outcome(s) of interest or the outcomes are known. In general, prospective studies are rated higher among researchers in terms of their reliability and significance of evidence relative to retrospective studies. Also, prospective studies are generally more expensive than retrospective studies. Ergo, by identifying their study as prospective, NCFM eSnurra Group were able to reap the benefits of: 1) a higher rated study by leeching the halo effects of true prospective studies, 2) significantly lower cost per observation of a retrospective database study via the incredibly low cost of collecting historical ultrasound and birth/delivery data from government databases, 3) an incredibly high return of perceived study rating on a small investment (i.e., low cost of collecting historical data from government databases) and 3) the word "prospective" included in their study to ensure inclusion in computer searches seeking matches on the word "prospective." NCFM eSnurra Group had used the conflate-to-obfuscate strategy to "game the system," successfully. What could be next: Possibly, an arbitrage market for existing retrospective ultrasound studies relabeled as prospective studies? Ironically, NCFM eSnurra Group made this very point about prospective vs. retrospective studies in their Gjessing et al. 2007 (except below); the very publication NCFM eSnurra Group claimed was a prospective study.
Interestingly, in the abstract of Gjessing et al. 1999 titled "Errors in Gestational Age: Evidence of Bleeding Early in Pregnancy" authors used gestational age data from the Medical Birth Registry of Norway. Consequently, the authors, including the lead author, NCFM Group's Håkon K. Gjessing, were compelled to include this caution statement regarding "the retrospective nature of the data" (excerpt below, emphasis added).
Also, the fourth excerpt above is a disingenuous attempt by the authors to denigrate legitimate prospective studies that may be resource constrained (most are), but what is even more limiting and more important is that the size of a legitimate, prospective study is set by, and strictly limited to, the size established by the statistical power calculation. This is a fact of which NCFM eSnurra Group authors and NCFM eSnurra "copyright owners" Håkon K. Gjessing, PhD of the Norwegian Institute of Public Health and Per Grøttum, MD, PhD, Professor of medical informatics, Section of Medical Informatics, Faculty of Medicine, UiO are very well aware. Nevertheless, they are committed to the NCFM eSnurra Group's agenda; an agenda that necessitates unethical decision-making, on many levels, including research misconduct via plagiarism and falsification.
NCFM eSnurra Group claimed in their Økland et al. 2011 paper (first excerpt below) that the 1987–2005 historical database data were somehow prospectively registered. Again, NCFM eSnurra Group believed their data were prospectively registered 30-years before their study was designed simply because birth/delivery occurs after pregnancy. And, the same thing again, in their Økland et al. 2012 paper (second excerpt below), using 1988–2009 historical database data. Again, these studies were retrospective database studies. As before, NCFM eSnurra Group believe all ultrasound studies on pregnancy, in the world are therefore prospective because birth/delivery occurs after pregnancy. Again, one can only wonder how these papers made if through referees' reviews and then past editorial review before publication in UOG.
Secular Trends/Drift & Confounding Variables:
Consider the potential of variances due to secular trends (or secular drift) and/or confounding (or missing) variables over the NCFM eSnurra dataset's 18-years calendar interval that could have had an effect on gestation time. If one or more secular trends did have an effect, the dataset would be correspondingly biased, thus any future predictions/estimations made via corresponding models would be biased. Just as an example, NCFM eSnurra Group's Gjessing et al. 2007 included several covariates, but only birth year range had an effect; a very large effect on FL-based predictions in the last 6-year period of the dataset that went completely unexplained in Gjessing et al. 2007. This was stated to be the result of older ultrasound technology of wider beam widths in the lateral direction of measurement on FL. Papers describing these technology-induced measurement errors were published in the 1980s. However, there may be other potential secular trends and confounding variables masked in historical datasets, which is a common problem among retrospective studies using historical databases. The fact that the secular trend induced in FL measurements as a result of constantly improving ultrasound technology throughout the years 1987–2004 enabled less distorted measurements of FL is a good example of why the study reported in Gjessing et al. 2007 and their other publications were retrospective studies, not prospective studies. Note: remember the -2.3 FL adjustment is added to the days remaining estimate to delivery (not to EDD), thus making the fetus or GA 2.3 days older to compensate for the secular trend of improving ultrasound technology.
A Concluding Supposition: An Oxymoron:
There is an agenda-driven supposition (first excerpt below) in the "Conclusions" section of the Abstract of NCFM eSnurra Group's Økland et al. 2010. Additionally, this supposition was not restricted to the Abstract, it also appeared in the body of the paper (second excerpt) where it was stated more as a fact and not as a supposition. A supposition is not a conclusion because a supposition is a belief held without proof or certain knowledge, such as an assumption. In short, a supposition is not a conclusion. The first sentence of the "Conclusion" section of the Abstract contains 17 words (or 31%) of the conclusion, while the second sentence, a supposition contains 38 words (or 69%) of the conclusion. When the "Conclusion" section of a paper's Abstract is filled with 69% supposition it means either: 1) there was little or no resulting evidence to conclude something substantive and/or 2) the authors had a non-science agenda to communicate. Again, one can only wonder how this NCFM eSnurra Group's agenda item made it through referees' reviews and past editorial review before publication in Ultrasound in Obstetrics and Gynecology. It is important to note that NCFM eSnurra Group's Økland et al. 2011 paper did not prove selection was the source of bias. Notice how in the "Conclusion" section the authors state: "These models have important shortcomings, probably because of strict selection criteria..." and 5-pages later the authors state: "The selection criteria of the sample-based models are important in producing these biases." So, which was it? Even though their study did not prove it, the authors were compelled to make their supposition in the "Conclusion" section because they wanted to communicate selection bias, without proof, which was NCFM eSnurra Group's agenda. Ergo, NCFM eSnurra Group's Økland et al. 2010 concluded in a supposition, an oxymoron. Communicating an agenda-driven message in paper published in an academic medical journal speaks to the ethos of scholarship, academic integrity and independence of the authors.
(see Plagiarism > HUTCHON TIMELINE 00.02.2001
- "Population prediction of remaining time has been used previously only to assess prediction quality 22. Our approach extends to constructing a full set of prediction models. Thus, it represents both a new and a complete approach to pregnancy dating using ultrasound examination." [Citation "22" referenced: "22. Taipale P, Hiilesmaa V. Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol 2001; 97: 189–194."] (Source: " A direct method for ultrasound Prediction of day of delivery: a new, population-based approach" H. K. Gjessing, P. Grøttum, S. H. Eik-Nes. Ultrasound in Obstetrics and Gynecology 2007; 30: 19–27, p. 23. Manuscript Accepted:16 April 2007; Version of record online: 8 June 2007; Issue online: 22 June 2007)
- Gjessing et al. 2007 states: "Population prediction of remaining time has been used previously only to assess prediction quality 22." This serves to confirm the term "prediction quality," as defined by NCFM eSnurra Group, was restricted to average prediction error or systematic error (mean, bias) because there was neither identification nor discussion of random error (standard deviation, precision) in NCFM Snurra Group's Taipale & Hiilesmaa 2001. This NCFM eSnurra Group definition of "prediction quality" intentionally excludes the quantification of random error (standard deviation, precision).
- NCFM eSnurra Group's Gjessing et al. 2007 states: "Our approach extends to constructing a full set of prediction models." However, it is a fact the NCFM eSnurra Group's Taipale & Hiilesmaa 2001 resulted in "a full set of prediction models" consisting of CRL, BPD & FL. It is interesting, and telling, to note NCFM Snurra Group did not disclose their supervision of, and contributions to, Taipale & Hiilesmaa 2001, nor did NCFM Snurra Group disclose the fact Pekka Taipale was an NCFM employee within the NCFM Snurra Group.
- NCFM eSnurra Group's Gjessing et al. 2007 states: "it represents both a new and a complete approach to pregnancy dating using ultrasound examination." Neither the method nor the approach were new in NCFM Snurra/eSnurra Group's:
1) Taipale & Hiilesmaa 2001
2) Eik-Nes et al. 2005
3) Gjessing et al. 2007
It is a 20-years old, well-documented fact the original idea and method of Population-based Direct EDD Estimation (PDEE) had been formulated by Dr. David J. R. Hutchon beginning in 1995 at Department of Obstetrics and Gynaecology, Memorial Hospital, Hollyhurst Road, Darlington, Co. Durham DL3 6HX, U.K. and published July 19, 1998 (Hutchon 1998), along with a demonstration of his original idea and method of PDEE, using a dataset of both CRL and BPD in his seminal Hutchon 1998 and website, 7 years and 9 years before NCFM eSnurra Group appropriated and plagiarized Dr. Hutchon's original idea and method of PDEE, and claimed it as their own original idea and method in NCFM eSnurra Group's Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, both of which were published by Ultrasound in Obstetrics & Gynecology (UOG), also known as The White Journal, the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG). This was followed by at least 15 additional NCFM eSnurra Group publications, all of which appropriated and plagiarized Dr. Hutchon's original idea and method, the Hutchon Method of PDEE, most recently in NCFM eSnurra Group's Gjessing et al. 2017, published April 2017 by UOG and Gjessing et al 2017b, published October 2017 in Norsk Epidemiologi. Moreover, Dr. Hutchon's first manuscript of his idea and method of PDEE was published 19.07.1998 in OBGYN.net (Hutchon 1998). Dr. Hutchon's second, more robust manuscript was received 13.07.1999 by UOG, which UOG and coded as "UOG 99/155 Proposed methodology for the preparation of ultrasound charts for estimating the date of delivery." Sturla H. Eik-Nes, NCFM eSnurra Group's founder, leader and 1 of the 3 "claimed copyright owners" of NCFM eSnurra, was President of ISUOG (1998 – 2002).
Whatever the intent or strategy of NCFM Snurra Group, it was and remains a well-documented fact Dr. Hutchon's original idea and method of PDEE had been published 19.07.1998 in Dr. Hutchon's seminal Hutchon 1998 in OBGYN.net, 2.5 years, 7 years and 9 years before NCFM Snurra/eSnurra Group's Taipale & Hiilesmaa 2001, Eik-Nes et al. 2005 and Gjessing et al. 2007, respectively, were published.
Interestingly, the bottom line conclusion of Taipale & Hiilesmaa 2001 was completely consistent with NCFM Snurra Group's agenda of excluding a pregnant woman's key pregnancy dates from medical evidence to ensure unilateral reliance on ultrasound for GA & EDD assignments in the second-trimester, i.e., the routine 18-week ultrasound exam which is widely reported to be less accurate than first-trimester ultrasound and, is completely consistent with NCFM eSnurra Group's current "method' (i.e., an appropriated, plagiarized & misused implementation of Dr. Hutchon's idea and method of PDEE) within a government-mandated protocol of evidence-obviated medicine which obviates all key pregnancy dates, without a pregnant woman's prior, informed, voluntary, explicit consent.
- "We do not see any reason to use LMP for dating when adequate ultrasonic data are available by midpregnancy." (Source: "Predicting Delivery Date by Ultrasound and Last Menstrual Period in Early Gestation" TAIPALE, PEKKA MD, PhD; HIILESMAA, VILHO MD, PhD. Obstetrics & Gynecology: February 2001 - Volume 97 - Issue 2 - p 189–194. Received May 30, 2000. Received in revised form September 25, 2000. Accepted October 12, 2000)
- "The smaller prediction error in our study suggests that dating pregnancies by ultrasound is more accurate at 8–16 weeks than at 12–22 weeks. The prediction error in our series was lowest at 12–14 weeks' gestation."
- "Assessment of gestational age from the time of IVF, CRL and BPD in pregnancies conceived after in vitro fertilization shows equally high agreement between the three methods, this supports the use of ultrasound as a reliable method for estimation of gestational age."
- "Although our main indication for screening at 13–14 weeks was to identify fetuses with increased nuchal translucency, 7 the opportunity to obtain fetal ultrasonic dimensions emerged as a useful adjunct. However, it might not be worth switching from midtrimester screening to 13-week screening for slightly better precision in dating."
Consider the "Conclusion" presented in the abstract of Taipale & Hiilesmaa 2001 in the excerpt below:
- "Conclusion: Ultrasound was more accurate than LMP in dating, and when it was used the number of postterm pregnancies decreased. Crown-rump length of 15–60 mm was superior to BPD, but then BPD (at least 21 mm) was more precise. Combining more than one ultrasonic measurements did not improve dating accuracy."
- CRL = 15–60 mm corresponds to GA = 8w+0 to 12w+3 (50th centile; Daya, 1993)
- BPD = 21 mm corresponds to GA = 12w+2 (50th centile; Johnsen et al. 2004)
While the statement below speaks for itself with respect to evidence-obviated medicine it is literally the last sentence, the bottom line of the NCFM Snurra Group's recognized, documented collaboration on Taipale & Hiilesmaa 2001, which deserves a modicum of consideration.
- "We do not see any reason to use LMP for dating when adequate ultrasonic data are available by midpregnancy."
NCFM eSnurra Group Claimed the Hutchon Method of PDEE as Their Own Idea & Method
The first sentence of the first page of both the English and Norwegian versions of NCFM eSnurra Group's websites state: "eSnurra is a new method for calculating Estimated Date of Delivery (EDD)"
- "eSnurra is a new method for calculating Estimated Date of Delivery(EDD), gestational age and fetal growth." (Source: http://www.esnurra.com/)
- eSnurra er en ny metode for beregning av termin, gestasjonsalder og fostervekst." (Source: http://www.esnurra.no/)
Interestingly and strangely, in the very first sentence of both their English and Norwegian websites for 'eSnurra', NCFM eSnurra Group state "eSnurra is a new method for calculating (beregning) EDD, GA and fetal growth." What happened to predicting/estimating EDD or GA?
- "eSnurra is a new method for calculating Estimated Date of Delivery(EDD), gestational age and fetal growth." (Source: http://www.esnurra.com/)
- "eSnurra er en ny metode for beregning av termin, gestasjonsalder og fostervekst." (Source: http://www.esnurra.no/)
The NCFM eSnurra Group made several patently false statements (emphasis added) in: 1) their Økland et al. 2007, an 08.10.2007 Poster Abstract at the 17th World Congress on Ultrasound in Obstetrics and Gynecology and 2) in NCFM eSnurra Group'S Gjessing et al. 2007.
- "Objectives To introduce a direct population-based method for prediction of term based on ultrasound measurements of the biparietal diameter and femur length in the second trimester of pregnancy" (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p.23)
- "This study assesses the predictive capacity of FL and BPD when a newly developed direct population-based method, eSnurra, is used." (Source: OP08: FETAL BIOMETRY: OP08.01: A new population-based term prediction method – evaluation of the BPD-based predictions, I. Økland, H. K. Gjessing, P. Grøttum, T. M. Eggebø, S. H. Eik-Nes, Ultrasound in Obstetrics & Gynecology 2007; 30: 456–546, p. 478)
- "Population prediction of remaining time has been used previously only to assess prediction quality 22. Our approach extends to constructing a full set of prediction models. Thus, it represents both a new and a complete approach to pregnancy dating using ultrasound examination." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p.23) Note: Reference 22: (Source: "Predicting Delivery Date by Ultrasound and Last Menstrual Period in Early Gestation" TAIPALE, PEKKA, HIILESMAA, VILHO, Obstetrics & Gynecology: February 2001 - Volume 97 - Issue 2 - p 189–194) [Note: Taipale & Hiilesmaa 2001 was a recognized, documented collaboration with NCFM Snurra Group.]
- "The great benefit of our design is precisely the fact that we do not base our analyses on the LMP, which is fraught with error due to factors such as recall bias and irregular menstrual cycles." (Source: Correspondence: Reply to "Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection" H. K. Gjessing*, P. Grøttum and S. H. Eik-Nes. Ultrasound Obstet Gynecol 2008; 31: 225–228., p. 226)
- "Interestingly, among these mothers, as many as 34.5% were uncertain of their LMP, illustrating the usefulness of our approach." (Source: ibid.)
- "To demonstrate the utility of our method in an independent Norwegian population, we applied our predictions to 9046 ultrasound scans collected over the period 2001–2006 at the Stavanger University Hospital." (Source: ibid.)
- "eSnurra is developed at the National Center for Fetal Medicine (NSFM) in Trondheim in Collaboration with the Department of Medical Informatics at UiO and National Public Health Institute in Oslo. It is a further development of Snurra that was introduced in 1984 and which until 2005 was in national use. Validation with approximately 16,000 pregnant women had shown that there was a systematic error (bias) in the lower area of the measurements made with Snurra. The development of eSnurra was intended to make a better method for predicting fetal age and term for use throughout the Norwegian the population of pregnant women. eSnurra is developed on the basis of approx. 120 000 ultrasound measurements of 41 343 pregnant women at NSFM and thus the method is population-based.
- "eSnurra er utviklet ved Nasjonalt senter for fostermedisin (NSFM) i Trondheim i samarbeid med Seksjon for medisinsk informatikk ved UiO og Nasjonalt Folkehelseinstitutt i Oslo. Det er en videreutvikling av Snurra som ble introdusert i 1984 og som fram til 2005 var i nasjonalt bruk. Validering med ca 16 000 gravide kvinner hadde vist at det forelå en systematisk feil (bias) i det nedre området av målingene gjort med Snurra. Utviklingen av eSnurra hadde som formål å lage en bedre metode for prediksjon av fosteralder og termin til bruk på hele den norske populasjonen av gravide. eSnurra er utviklet på bakgrunn av ca. 120 000 ultralydmålinger på 41 343 gravide ved NSFM og metoden er dermed populasjonsbasert."
(Source: Letter: Helsedirektoratet to Helse- og omsorgsdepartementet, 13.10.2014 Vår ref.: 12/6746-19, Saksbehandler: Cecilie Sommerstad. "Helsedirektoratets anbefalinger til Helse- og omsorgsdepartementet etter oppfølging av rapport fra «Uavhengig ekspertgruppe for vurdering av svangerskapsavbrudd»"; Local English & Norwegian HTML Version: 13.10.2014 Hdir Letter to HOD); Original Norwegian PDF Version: Health Directorate's 13.10.2014 Recommendations Letter to Ministry of Health and Care Services)
NCFM eSnurra Group's Medico-Marketing Agenda vs. Medical Science
In her 2012 NTNU dr.philos. Thesis (p. 28 & 44), Inger Økland identified what is required for a population-based model to be validated for a specific population, such as Trondheim vs. Bergen. Also, it states the "the methods must be re-calibrated when the examination practice and the population distribution change," such as when "the methods" are used for a different population within a country (e.g., Trondheim vs. Bergen) or within a different country.
- "With a population-based model, the performance of the method is evaluated directly from the reference material. However, if the aim is to get a measure of how the model's predictions suit other populations with possibly different examination routines, a validation on the actual population has to be carried out." (p. 28) (Source: Inger Økland 2012 NTNU dr.philos. Thesis: "Biases in second-trimester ultrasound dating related to prediction models and fetal measurements" NTNU, 13 January 2012. Principal Supervisor: Sturla H. Eik-Nes, MD, PhD , Co-supervisors: Håkon K. Gjessing, PhD & Per Grøttum, MD, PhD)
- "A correct’ EDD should of course concur with the actual median date of delivery in the population." (Source: ibid., p. 42)
- "Thus, taking advantage of huge databases, into which data of adequate quality from unselected and representative populations have been continuously collected, is an indisputable opportunity." (Source: ibid., p. 42)
- "The population data will reflect the local referral practice and the distribution of the scheduled examinations; with a routine second-trimester examination practice, the majority of the included examinations will be measurements from pregnancy week 17–19, as shown in Figure 16." (Source: ibid. p. 43-44)
- "Being ‘trained’ on a population distribution, the models will operate in this fashion and produce predictions that are optimal for the population." (Source: ibid., p. 44)
- "In other words, the prediction bias for the sample-based models tends to vary with the fetal size at examination (Figure 11 and 12) (Tunón et al. 1998, Backe and Nakling 2006), while the population-based models are aimed at the actual population and avoid these biases (Figure 14)." (Source: ibid., p. 44)
- "To ensure lasting optimal predictions, the methods must be re-calibrated when the examination practice and the population distribution change, and future models are not likely to survive unadjusted for 20 years, as did the Trondheim–1984-model." (Source: ibid., p. 44)
- "In fact, the optimal and essential calibration is to use population data in an overall calibration, in order to remove the biases over the whole range of measurement values, i.e., to apply a population-based approach to prediction of EDD (Figure 26 c)." (Source: ibid., p. 80)
Consider what Eric O. Ohuma and the late Douglas G. Altman had to say about multiple populations in their 2019 paper which "discusses the features of study design and methodological considerations for constructing reference centile charts for attained size, growth, and velocity charts with a focus on human growth charts used during pregnancy."
- "In contrast, the descriptive approach is commonly used to produce a reference chart that describes the anthropometry of a given population at a particular time and place, such as a hospital, region, or country. Descriptive reference charts are usually based on an unselected population with minimal exclusion criteria, for example, known risk factors for optimal health. Although they are used more widely, descriptive charts are only relevant to the source population. Different populations will differ in many aspects, such as rates of smoking during pregnancy, malaria, gestational diabetes, and maternal obesity, which can all affect newborn outcomes. In principle, following the descriptive approach requires separate reference charts for each subpopulation of interest." (p. 3529) (Source: "Design and other methodological considerations for the construction of human fetal and neonatal size and growth charts" Eric O. Ohuma, Douglas G. Altman. Statistics in Medicine 2019 Aug 30; 38(19): 3527–3539. Published online 2018 Oct 23. doi: 10.1002/sim.8000. URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6767035/ PDF: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6767035/pdf/SIM-38-3527.pdf)
Nevertheless, and strangely, Directorate of Health stated NCFM eSnurra Group's population-based method (i.e. the appropriated, plagiarized, misused Hutchon Method of PDEE) was "installed in over 90 countries" which, given the population-based model requirements stated in Økland's 2012 NTNU dr.philos. Thesis (above, and the excerpt directly above), this would require: 5 prediction/estimation models per country-population x 90 country-populations = 450 country-population-specific models built from country-population-specific "reference material" collected from country-population-specific, quality-assured historical databases of past pregnancies and then validated. (Source: DEBATT OG KRONIKK "Helsedirektoratets rolle – og eSnurra" Skrevet av: Johan Torgersen / Torunn Janbu. Dagens Medisin. Publisert: 2015-04-13 11.49)
Additionally, accessing NCFM eSnurra Group's website and the NCFM eSnurra Group's APP for Android and iOS from another country appears to be what Jens Grøgaard and Cecilie Sommerstad, both Senior Advisers, Directorate of Health, were referring in their request to NOKC (Forslagsnr: 792, 15.11.2013) on behalf of Ministry of Health & Care Services and Directorate of Health, when they stated:
- "Both methods are research-based and developed respectively at UiB and NTNU. Internationally, both methods well recognized and used in several countries." (Source: Knowledge Centre for Health Services in Public Health, Assessment of the most accurate and research-based tools of gestation and term, Jens Grøgaard, Cecilie Sommerstad, Forslagsnr: 792, 15.11.2013.)
Consider if NCFM eSnurra Group's population-based "method" with models trained/built on the > 95% White Norway-Trondheim population, were to be used in the Philippines and South Africa, where the populations are < 10% White. Then, consider this in the context of the findings from the "Racial/Ethnic Standards for Fetal Growth, the NICHD Fetal Growth Studies" or Buck Louis et al. 2015, are included below.
- "The findings from the NICHD Fetal Growth Studies suggest significant differences in fetal growth among different racial/ethnic groups as exemplified by individual biometrics and EFW." (Source: "Racial/Ethnic Standards for Fetal Growth, the NICHD Fetal Growth Studies" Germaine M. BUCK LOUIS, PhD, MS, Jagteshwar GREWAL, PhD, MPH, Paul S. ALBERT,PhD, Anthony SCISCIONE, DO, Deborah A. WING, MD, William A. GROBMAN, MD, MBA, Roger B. NEWMAN, MD, Ronald WAPNER, MD, Mary E. D’ALTON, MD, Daniel SKUPSKI, MD, Michael P. NAGEOTTE, MD, Angela C. RANZINI, MD, John OWEN, MD, MSPH, Edward K. CHIEN, MD, Sabrina CRAIGO, MD, Mary L. HEDIGER, PhD, Sungduk KIM, PhD, Cuilin ZHANG, MD, MPH, PhD, and Katherine L. GRANTZ, MD, MS. Am J Obstet Gynecol. 2015 October ; 213(4): 449.e1–449.e41. doi:10.1016/j.ajog.2015.08.032.)
- "Our finding that the White standard overestimates the percentage of non-White fetuses <5th percentile agrees with recent findings from a prospective study of fetal growth for three racial groups in Papua New Guinea. 28 Despite the low-risk status of the pregnant women followed with serial ultrasonology for EFW and birthweight, use of the Hadlock formula (Caucasian) or Congolese standard 14 overestimated the percentage of Papua New Guinea fetuses considered <10th percentile." (Source: ibid., p 7)
- "Instead of presupposing no racial/ethnic differences, we considered that fetal dimensions could vary even in early pregnancy, as we found for FL and AC, consistent with adult racial/ethnic differences in size and proportion. While we observed little variation by race/ethnicity for BPD early in pregnancy, highly significant differences are detectable in HC by about 21 weeks’ gestation and remained until delivery even in adjusted analyses. The ratio of HC/AC generally declines over gestation as expected, but the differences in trajectories demonstrate that there are significant differences in proportions by racial/ethnic group that should be considered in the evaluation of growth restriction." Source: ibid., p. 8)
- "In summary, we found highly significant differences in fetal growth by self-identified maternal race/ethnicity for BPD, HC, AC, HL, FL, HC/AC, and EFW among low-risk women randomized to longitudinal ultrasonology examinations. These findings should help inform clinical management consistent with precision medicine initiatives. 38" (Source: ibid., p. 8-9)
- "Current standards for ultrasound evaluation of fetal growth may lead to misclassification of up to 15 percent of fetuses of minority mothers as being too small, according to a study by researchers at the National Institutes of Health (NIH) and other institutions." (Source: "NIH study finds racial, ethnic differences in fetal growth" NEWS RELEASE U.S. Department of Health & Human Services, National Institutes of Health. Tuesday, September 29, 2015)
- In conclusion, we have shown that fetal femur length is less than expected in Asian women and greater than expected in black women compared with fetal femur length in white women. These differences are small, yet they may influence the success of screening for chromosomal abnormalities using the genetic sonogram (with standard biometric tables)." (Source: "Variation in Fetal Femur Length With Respect to Maternal Race" Thomas D. Shipp, MD, Bryann Bromley, MD, Maria Mascola, MD, Beryl Benacerraf, MD. Journal of Ultrasound in Medicine Volume 20, Issue 2, p. 143. Version of Record online: 1 FEB 2001)
- research misconduct,
- medical malpractice,
- breach of medical ethics,
- false advertising,
- poor manners,
- all of the above?
- "The study that is the basis for the new population-based term prediction model, eSnurra (Figure 13), was published in 2007 (Gjessing et al. 2007). This was a new cooperation project between Eik-Nes and Grøttum, now in alliance with the mathematician Håkon K. Gjessing. To base a term prediction model on fetal ultrasound measurements from a non-selected population of 36 982 pregnancies (41 343 ultrasound examinations), was a new approach that seemed obvious to statisticians and mathematicians, but not equally obvious to obstetricians." (p. 26) (Source: Inger Økland's 2012 NTNU dr.philos. Thesis: "Biases in second-trimester ultrasound dating related to prediction models and fetal measurements" NTNU, 13 January 2012. Principal Supervisor: Sturla H. Eik-Nes, MD, PhD , Co-supervisors: Håkon K. Gjessing, PhD & Per Grøttum, MD, PhD)
- "To rectify this problem, a population-based model was developed (Gjessing et al. 2007), predicting date of delivery directly." (Source: ibid., p. 43)
The other important take-away point is the fact Directorate of Health were promoting NCFM eSnurra Group's "population-based method" had been "installed in over 90 countries" while, simultaneously, and in the very same article "Helsedirektoratets rolle – og eSnurra, (Referanser: 1)", promoting Økland's 2012 NTNU dr.philos. Thesis as independent, academic justification of their knowledge-obviated, medically & ethically flawed 2014 Recommendation without any consideration or apparent comprehension of that which was stated in Økland's 2012 NTNU dr.philos. Thesis regarding the NCFM eSnurra Group's "population-based method." There are 101 occurrences of the compound adjective "population-based" in Økland's 2012 NTNU dr.philos. Thesis. One would think Directorate of Health would have had a modicum of comprehension of the conflict of interest and the science-bending implications of promoting the medico-marketing point of "installed in over 90 countries." This fact serves as additional evidence in support of an important and, hopefully, now, all-too-obvious point made by Bergen Group:
- "In this instance we feel that the Directorate of Health has acted beyond their competence and that they have simplified the issues beyond all understanding." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
Excessive Claiming Behavior From One Group of Plagiarists to Another
The extent of NCFM eSnurra Group's efforts to promote and protect their "claim" to Dr. Hutchon's original idea and method, the Hutchon Method of PDEE, is evidenced in the excerpts below, emphasis added. The excerpts are from comments made by NCFM eSnurra Group in a "Comment & Reply Correspondence" in The Journal of Maternal-Fetal & Neonatal Medicine regarding Salomon et al. 2010, coauthored by Yves Ville (see Hutchon Timeline 26.07.2007, 17.09.2007, 21.09 2007, 29.02.2008, 13.02.2009, 11.12.2009) to which Salomon et al. Group replied (included below). NCFM eSnurra Group makes the point, incessantly, that the method of Population-based Direct EDD Estimation is "their method." Maybe Dr. Hutchon could take a modicum of solace in the fact NCFM eSnurra Group so valued the Hutchon Method of PDEE, they defended their illegitimate claim, vociferously, from a perceived encroachment by Salomon et al. 2010 who, incredibly, had also appropriated and plagiarized the Hutchon Method of Population-based Direct EDD Estimation. However, it is important to note Salomon et al. 2010 cited NCFM eSnurra Group's Gjessing et al. 2007, extensively, and Salomon et al. 2010 cited Taipale & Hiilesmaa 2001 which was the result of a recognized NCFM eSnurra Group collaboration. Unfortunately, Dr. Hutchon's seminal Hutchon 1998 was neither cited nor acknowledged by Taipale & Hiilesmaa 2001, or by NCFM eSnurra Group's Eik-Nes et al. 2005 or Gjessing et al. 2007 or by the French Group, Salomon et al. 2010 which included Dr. Yves Ville as a coauthor and who was Editor-in-Chief of Ultrasound in Obstetrics & Gynecology at the time of the plagiarism
NCFM eSnurra Group's Comments to Salomon et al. Group: Excessive Claiming Behavior
Included below is an epic and classic display of excessive claiming behavior of plagiarists, courtesy of NCFM eSnurra Group's Håkon K. Gjessing, Per Grøttum, Inger Økland, & Sturla H. Eik-Nes.
- It is very interesting to see the median-based direct prediction method that we developed for second trimester measurements [,] being applied to first trimester data.
- "Although the size of their study is much smaller than ours, it illustrates the strength of our population-based method; when high-quality registry data are available, the direct method provides a prediction model adapted to the clinical setting that the data were collected under, whether it is first- or second trimester routine scans."
- "To avoid obscuring the central concept, it should be stressed that the essence of the authors' approach is precisely the one developed in our paper, namely a direct estimation of median (and other centiles) of remaining time of pregnancy."
- "However, we believe that such technical differences are of secondary importance to the overarching principle of direct median prediction."
- "In fact, this is precisely one of the important empirical questions that can be addressed with our direct prediction method."
- "This is precisely what the direct prediction method can provide. It may well be the case that first trimester scans provide higher precision than second trimester scans, but it would be very useful to see this verified scientifically, which could be done with our direct prediction method."
- "In conclusion, we welcome the authors' application of our direct prediction approach to first trimester measurements."
- "We believe our approach opens for the development of population-based prediction curves over a large range of measurements and populations."
- "While we fail to see any particular advantages of the alternative quantile smoothing approach suggested by the authors, the advantages of our direct prediction method are still obvious: it obtains fully ultrasound-based estimates of median birth term, and allows the precision of these estimates to be assessed and quantified directly."
- (Sources)
Comment & Reply Correspondence: Comment and reply on: Prediction of the date of delivery based on first trimester ultrasound measurements: an independent method from estimated date of conception, Håkon K. Gjessing, Per Grøttum, Inger Økland & Sturla H. Eik-Nes (2010), The Journal of Maternal-Fetal & Neonatal Medicine, 23:8, 944-947, DOI: 10.3109/14767050903420309)
Salomon et. al. Group's Salomon et al. 2010: (Source: Prediction of the date of delivery based on first trimester ultrasound measurements: An independent method from estimated date of conception, Laurent J. Salomon, Costanza Pizzi, Antonio Gasparrini, Jean-Pierre Bernard & Yves Ville, The Journal of Maternal-Fetal & Neonatal Medicine Volume 23, 2010 - Issue 1)
NCFM eSnurra Group's Gjessing et al. 2007: (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, DOI: 10.1002/uog.4053) Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 21)
- A serious lack of comparability and reproducibility by other researchers
- The local linear quantile regression routine used in Gjessing et al. 2007 "...is not available to other researchers," amounting to the use of a black box with respect to other researchers
- "Before addressing the specific comments, we are pleased to explain why we disagree with Gjessing et al. when they argue that they ‘fail to see any particular advantage of the alternative quantile smoothing approach’ we developed. These advantages are called comparability and reproducibility. Given that no method could be considered perfect to answer a scientific question, the availability of different analytic strategies offers a way to compare the benefits and weaknesses of each approach, strengthening the plausibility of the findings if the results are consistent between different choices. This issue is closely related to the second advantage: our spline-based approach [3] is performed through functions currently implemented in the major statistical packages, for example Stata (StataCorp, LP, TX) with rc_spline or mkspline, R (R Development Core Team) with ns, and SAS (SAS Institute) with proc transreg. The availability of these functions gives the opportunity to replicate our method in other populations, and to compare it against potential alternative solutions. To our knowledge, the local linear quantile regression (LLQR) [4] proposed by Gjessing et al. is not directly implemented in any major statistical software, and they needed to develop their own routine which is not available to other researchers."
(Sources)
Comment & Reply Correspondence: (Source: "Comment and reply on: Prediction of the date of delivery based on first trimester ultrasound measurements: an independent method from estimated date of conception" Håkon K. Gjessing, Per Grøttum, Inger Økland & Sturla H. Eik-Nes (2010), The Journal of Maternal-Fetal & Neonatal Medicine, 23:8, 944-947, DOI: 10.3109/14767050903420309)
Salomon et. al. Group's Salomon et al. 2010: (Source: Prediction of the date of delivery based on first trimester ultrasound measurements: An independent method from estimated date of conception, Laurent J. Salomon, Costanza Pizzi, Antonio Gasparrini, Jean-Pierre Bernard & Yves Ville, The Journal of Maternal-Fetal & Neonatal Medicine Volume 23, 2010 - Issue 1)
NCFM eSnurra Group's Gjessing et al. 2007: (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, DOI: 10.1002/uog.4053) Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 21)
Taipale & Hiilesmaa 2001 (Collaboration with NCFM eSnurra Group): (Source: "Predicting delivery date by ultrasound and last menstrual period in early gestation" Taipale P, Hiilesmaa V. Obstet Gynecol 2001; 97: 189–194.)
Salomon et al. 2010 Also Plagiarized the Hutchon Method of PDEE
Salomon et al. 2010 also appropriated and plagiarized Dr. Hutchon's original idea and method, the Hutchon Method of Population-based Direct EDD Estimation (PDEE). Again, it is important to note Salomon et al. 2010 cited NCFM eSnurra Group's Gjessing et al. 2007, extensively. Nevertheless, the "Comment & Reply" exchange is decidedly interesting considering:
- 2 separate research groups comprising 2 separate groups of authors
- 2 separate publications, Gjessing et al. 2007 and Salomon et al. 2010
- 2 separate publishers, Ultrasound in Obstetrics and Gynecology (UOG) also known as The White Journal, the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG), published by John Wiley & Sons, Inc. and The Journal of Maternal-Fetal & Neonatal Medicine, the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, and the International Society of Perinatal Obstetricians, published by Informa plc,
- both plagiarizing author groups trading criticisms of the other group's appropriated, plagiarized implementation of the same original idea and method, the Hutchon Method of PDEE, in a "Comment & Reply" article published in The Journal of Maternal-Fetal & Neonatal Medicine
- both publications citing the Taipale & Hiilesmaa 2001, a collaboration with NCFM eSnurra Group, the first known appropriation and plagiarism of Dr. Hutchon's original idea and method, the Hutchon Method of PDEE,
- both groups of authors presenting poster abstracts of their respective, appropriated, plagiarized implementations of Dr. Hutchon's original idea and method, the Hutchon Method of PDEE, on 08.10.2007 at the 17th World Congress on Ultrasound in Obstetrics and Gynecology
- both groups' poster abstracts (3 by NCFM eSnurra Group, 1 by Salomon et al. Group) of their respective appropriated, plagiarized implementations of Dr. Hutchon's original idea and method, the Hutchon Method of PDEE, published side-by-side on the same page (p. 478), literally, literally in Ultrasound in Obstetrics & Gynecology's "Special Issue: 17th World Congress on Ultrasound in Obstetrics and Gynecology October 2007" while, simultaneously, Salomon et al. Group coauthor Yves Ville was Editor-in-Chief of Ultrasound in Obstetrics & Gynecology. The 3 poster abstracts published on the same page include: Eik-Nes et al, 2007 , Økland et al. 2007b and Salomon et al. 2007, with both author groups including a member who has served as President of ISUOG:
- NCFM eSnurra Group member Sturla H. Eik-Nes, President of ISUOG (1998-2004), prior to publication of NCFM eSnurra Group's Gjessing et al. 2007 and during the time Dr. Hutchon's first and second manuscripts of his original idea and method, the Hutchon Method of PDEE, were submitted to Ultrasound in Obstetrics & Gynecology;
- Salomon et al. Group member Yves Ville, President of ISUOG (2012-2014), after publication of Salomon et al. 2010; and, Yves Ville was Editor-in Chief of Ultrasound in Obstetrics & Gynecology before, during & after publication of Salomon et al. 2010 and to whom Dr. Hutchon sent his first registered letter dated 26.07.2007 seeking a by-the-book investigation and redress for the appropriation and plagiarism of his original idea and method, the Hutchon Method of PDEE in NCFM eSnurra Group's Gjessing et al. 2007, published 08.06.2007 by Ultrasound in Obstetrics and Gynecology
Plagiarism & Next-Steps
NCFM eSnurra Group's Gjessing et al. 2007 appear to have made 4 changes to the Hutchon Method of PDEE in their appropriated, plagiarized implementation:
- replaced mean days renaming with median days remaining
- replaced the gestation period of 280 days with 282 days and, later, 283 days
- replaced least-squares & polynomial regressions with local linear quantile regression (LLQR)
- ignored Dr. Hutchon's 3 key, cautionary statements made in his seminal Hutchon 1998 [This is the "misused" part.]
- "The chart is only for estimating the date of delivery."
- "Just as Boerhaave was not actually measuring the length of pregnancy, and the word "gestation" is used to describe the measurement of time from the last menstrual period to reflect this, so also there is no pretence that this method is determining fetal age."
- "The approach mimics, in modern terms, the method originally formulated by Boerhaave. By adopting this approach we do not need to concern ourselves about the length of the cycle nor the certainty of the dates. Provided the fetus can be assessed as normal using other criteria, this chart can be used to provide the best estimate of the date of delivery (EDD)." (Source: "'Back to the Future' for Hermanni Boerhaave' or 'A rational way to generate ultrasound scan charts for estimating the date of delivery'" Hutchon DJR, ObGyn Ultrasound, Obgyn.net 1998: http://www.obgyn.net/obgyn-ultrasound/back-future-hermanni-boerhaave-or-rational-way-generate-ultrasound-scan-charts-estimating-date [Note: URL updated from published original by ObGyn.net])
- "The traditional ultrasound dating chart does not provide an expected date of delivery but does provide a virtual last menstrual period from which the expected date of delivery can be calculated using Naegele's rule."
NCFM eSnurra: Black Box Techniques
The NCFM eSnurra disclosure of statistical techniques in Gjessing et al. 2007 demonstrate comparability and reproducability by other researchers is not possible due to their use of custom statistical analysis software which is not available in the major statistical packages used by most researchers, thus creating what is commonly termed a black box model or system, a point well made by Salomon et al. in their "Comment & Reply Correspondence " with NCFM eSnurra Group. In the excerpt below, the phrase "which were verified in part against the quantreg implementation of QR models in R" serves to solidify this point. This may very well explain why after 10-years there is still no evidence NCFM eSnurra Group's models and statistical techniques having been reproduced and verified by independent researchers.
- "All statistical analyses, including the LLQR, were performed using our own implementations in R version 2.2.1 for Windows 19, which were verified in part against the quantreg implementation of QR models in R 20." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 21. DOI: 10.1002/uog.4053) References: 19 R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing: Vienna, 2005; http://www.r-project.org [Accessed 14 December 2006]. 20 Koenker R. quantreg: Quantile Regression. R package version 3.90. R Foundation for Statistical Computing: Vienna, 2006; http://www.r-project.org [Accessed 14 December 2006].
- "Wang et al. (2007a) pointed out that the GCV approach tends to produce overfitted models even as the sample size goes to infinity." (Source: Quantile regression for single-index-coefficient regression models, p. 308-309. Rong Jianga, Wei-Min Qianb, Statistics & Probability Letters Volume 110, March 2016, Pages 305–317. http://doi.org/10.1016/j.spl.2015.09.022) Reference: Wang et al. (2007a) (Source: "Robust regression shrinkage and consistent variable selection via the LAD-LASSO" H. Wang, G. Li, G. Jiang, J. Bus. Econom. Statist., 20 (2007), pp. 347–355)
- "Even at the lower end of our sampling distribution (from 37 mm BPD and below), a cross-validation 24 verified that the sample size was large enough to cancel possible effects of random bias (results not shown)." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 21. DOI: 10.1002/uog.4053)
NCFM eSnurra Group Conflates Predicted/Estimated GA with Calculated GA
One can predict/estimate y from x (via y regressed on x; i.e. y depends on x) if the dataset observations include both the x and y variables (x = independent variable; y = dependent variable). Not surprisingly, it is impossible to predict/estimate z from x (via y regressed on x) if the dataset only contains observations of x and y. Both Bergen Group and NCFM eSnurra Group regress on the very same independent x variable, i.e., ultrasound-based measurements of fetal metrics (e.g., BPD, FL, HC, CRL, MAD, etc.). However, these two groups use completely different dependent y variables. The Bergen Group's dependent y variable is gestational age (GA) on the ultrasound date, while the NCFM eSnurra Group's dependent y variable is the number of days remaining from the ultrasound date to birth/deliver. The Bergen Group predicts/estimates GA directly from ultrasound fetal metric measurements and NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) directly predicts/estimates days remaining from ultrasound fetal metric measurements to calculate EDD. Consequently, it is impossible for the Bergen Group to directly predict/estimate EDD and it is impossible for NCFM eSnurra Group to directly predict/estimate GA. However, Bergen Group and NCFM eSnurra Group can each calculate (not predict/estimate) their predicted/estimated complement EDD and GA, respectively, by using a fixed gestation time from LMPD (Bergen Group uses 282 days, NCFM eSnurra Group, 283 days). Consequently, the Bergen Group can subtract the predicted/estimated GA on the ultrasound date from the ultrasound date to calculate a virtual LMPD, and then add 282 days to calculate EDD. And, NCFM eSnurra Group can subtract the predicted/estimated days remaining to delivery on the ultrasound date from 283 days to calculate GA on the ultrasound date. Both Bergen Group and NCFM eSnurra Group depend on the use of a virtual LMPD date to calculate EDD and GA, respectively, and then subtract GA on the ultrasound date from the ultrasound date to calculate a virtual LMPD, respectively. And, because these are calculation methods and not direct prediction/estimation methods from ultrasound measurements, these "calculated" methods are sometimes referred to as "indirect" methods.
To get an idea of NCFM eSnurra Group's conflate-to-obfuscate strategy, consider the excerpt below in the context of the preceding paragraph. NCFM eSnurra Group disparaged "traditional models" or, more specifically, Bergen Group, because Bergen Group does not directly predict/estimate EDD from ultrasound fetal metric measurements and, therefore, must calculate EDD from the LMPD established by their directly predicted/estimated GA. Consequently, and by using NCFM eSnurra Group's own reasoning, NCFM eSnurra Group must also believe they "primarily estimate EDD from second-trimester fetal measurements when they calculate GA, thus, gestational age (GA) "is actually an indirect and secondary issue" for NCFM eSnurra Group. Day-0 (or GA = 0w+0) of the median 283-day "gestation period" set by NCFM eSnurra Group is the virtual LMPD. Moreover, all GA values calculated by NCFM eSnurra Group depend on a virtual LMPD.
- "Traditional models primarily estimate a last menstrual period (LMP) from second-trimester fetal measurements, thus, the estimated date of delivery (EDD) is actually an indirect and secondary issue 3, 5, 6." (Source: Advantages of the population-based approach to pregnancy dating: results from 23 020 ultrasound examinations, I. ØKLAND, J. NAKLING, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2012; 39: 563–568, p. 563 DOI: 10.1002/uog.10081)
In the excerpt below, NCFM eSnurra Group conflate estimates of GA with estimates of EDD. NCFM eSnurra Group's method (i.e. the appropriated, plagiarized, misused Hutchon Method of PDEE) estimates EDD and, therefrom, calculates GA using the equivalent of Naegele's rule. In short, it is not "standard procedure to obtain estimates of the gestational age of the fetus and of the expected day of delivery." This is a conflate-to-obfuscate strategy, trying to communicate the terms estimate and calculate with respect to GA & EDD as synonymous; and, this has worked well because it is clear Directorate of Health is confused by direct estimation of GA and calculation of GA from a direct estimation of EDD to the point of incompetence.
- "In modern pregnancy care it is standard procedure to obtain estimates of the gestational age of the fetus and of the expected day of delivery 1–3." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 19. DOI: 10.1002/uog.4053)
- Regarding the Bergen Group
"The estimation methods are solely aimed at computing gestational age at the time of the ultrasound examination; the true problem of prediction of term is hardly ever mentioned, let alone made explicit, except for an ‘understanding’ that a certain number of days should be added to the estimated start of pregnancy." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIKNES; Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 20. DOI: 10.1002/uog.4053) - Regarding NCFM eSnurra Group
The estimation methods are solely aimed at computing days remaining at the time of the ultrasound examination, the true problem of prediction of gestational age is hardly ever mentioned, let along made explicit, except for an 'understanding' that a certain number of days should be subtracted from the estimated end of pregnancy.
- is not trying to conflate-to-obfuscate to try to claim a prediction/estimation capability they do not have.
- regressed on ultrasound fetal metric measurements with GA as their dependent variable, not days remaining to date of delivery, in order to directly predict/estimate GA.
Conflate to Obfuscate
Included in the excerpts below is a good example of NCFM eSnurra Group prosecuting their science-bending agenda with a conflate-to-obfuscate strategy. Specifically, in NCFM eSnurra Group's Eik-Nes et al. 2006 they claimed:
- "polynomial regressions...are becoming obsolete" (Source: LETTER TO THE EDITOR: Regarding ‘‘Term prediction with ultrasound: evaluation of a new dating curve for biparietal diameter’’ STURLA H. EIK-NES, PER GRØTTUM, HÅKON GJESSING. Acta Obstetricia et Gynecologica Scandinavica Volume 85, Issue 10, October 2006, Pages 1276–1278 First published: October 2006 DOI: 10.1080/00016340600839668)
- to have developed "new methods using large population-based data" (i.e., the appropriated, plagiarized Hutchon Method of PDEE) (Source: ibid.)
- "to predict gestational age and expected day of delivery." (Source: ibid.)
- "The traditional polynomial regressions used in ‘‘Snurra’’ and ‘‘Terminhjulet’’ are becoming obsolete in constructing models in obstetrics. New methods using the large population-based data now available must form the future tools to predict gestational age and expected day of delivery. Such methods have recently been developed (10)." (Source: LETTER TO THE EDITOR: Regarding ‘‘Term prediction with ultrasound: evaluation of a new dating curve for biparietal diameter’’ Acta Obstetricia et Gynecologica. 2006; 85: 1276"1279, p. 1277) Citation 10 (Source: Eik-Nes SH, Blaas HG, Grøttum P, Gjessing H. Predicting remaining time of pregnancy: a new approach to the prediction of day of delivery. 15th World Congress on Ultrasound in Obstetrics and Gynecology. Book of Abstracts. Ultrasound Obstet Gynecol 2005; 26: 341 [Google Scholar])
Conflate-to-Obfuscate: predict, estimate & calculate
In the following sections it will become obvious NCFM eSnurra Group works to conflate the words "estimate" and "calculate" with respect to GA & EDD as a conflate-to-obfuscate tactic in order to claim NCFM eSnurra Group possesses GA estimation capability when, in reality, it is not possible for NCFM eSnurra to estimate GA; GA must be calculated from NCFM eSnurra EDD using the equivalent of Naegele's rule, in reverse. Again, conflating the words "estimate" and "calculate" to obfuscate the difference is bending science, which is a large part of NCFM eSnurra Group's agenda, which is bending science for ambition, ideology and policy, not research-based science. In fact, NCFM eSnurra Group's agenda of bending policy-relevant science is more akin to a political party gearing up for an election by crafting and repeating a message that is intentionally confusing. Moreover, this very same science-bending, conflate-to-obfuscate strategy was used by NCFM eSnurra Group to obfuscate the differences between a retrospective (looking back) study and a prospective (looking forward) study. These were clearly intentional acts, evidenced by the deliberate actions of 2 of NCFM eSnurra Group's members who were (and remain) "copyright owners" of NCFM eSnurra:
- Håkon K. Gjessing, PhD of the Norwegian Institute of Public Health, who coauthored a book for Springer's Statistics for Biology and Health Series and who developed a genetic association analysis package for the open-source R-project.org.
- Per Grøttum, MD, PhD, Professor of medical informatics, Section of Medical Informatics, Faculty of Medicine, UiO.
An Apt Analogy
Hakon K. Gjessing's UiB webpage for his genetic association analyses software package includes the following appeal for ethical propriety with respect to acknowledging, citing and referencing his work and, appropriately so, as there are too many who need to be reminded of the ethical etiquette.
- "Please: If you use Haplin in your analyses, it will be much appreciated if you refer to Haplin (this web page), or better, to the Annals of Human Genetics paper above." (Source: https://folk.uib.no/gjessing/genetics/software/haplin/111annet/Haplin_3.5/)
- "Please: If you use my original idea and method (PDEE) as your country's official national healthcare method to estimate EDD, it will be much appreciated if you refer to Hutchon.net (this website), or better, to my 1998 OBGYN.net paper above."
- "Just as Boerhaave was not actually measuring the length of pregnancy, and the word "gestation" is used to describe the measurement of time from the last menstrual period to reflect this, so also there is no pretence that this method [PDEE] is determining fetal age." (Source: Hutchon 1998)
Corrupted Process: NCFM eSnurra Group: Mission Creep to Mission Leap
The objective of the NCFM eSnurra Group study, as explicitly stated in their 2007 paper was clearly defined (excerpt below) by the three NCFM eSnurra Group authors, the three "copyright owners" of NCFM eSnurra (© 2007 EikNes, Grøttum og Gjessing).
- "Objectives To introduce a direct population-based method for prediction of term based on ultrasound measurements of the biparietal diameter and femur length in the second trimester of pregnancy" (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p.23) .
- "... the aim of this study was to develop a method for estimating expected day of delivery and gestational age based on a large population" (Source: same as above, p. 20)
- "Our primary focus in this paper has been on prediction of term. It is interesting to note that the approach also provides estimates for gestational age at the time of the ultrasound examination. (Source: p. 26, same as above)
It boggles the mind Directorate of Health either misses or ignores the important distinction between actually predicting/estimating fetal age and GA from ultrasound fetal metric measurements (Bergen Group) and calculating fetal age and GA from predictions/estimates of the remaining days until EDD using the equivalent of Naegele's rule, in reverse, (NCFM eSnurra Group). Clearly, the basis for determining fetal age and GA is not the end of the pregnancy, but its beginning, and not from calculations based on predictions/estimates of EDD (NCFM eSnurra Group) but from direct predictions/estimates of GA from fetal metric measurements (Bergen Group).
Conflate-to-Obfuscate: Estimate and Calculate
There were 20 occurrences of the word "estimate" or a derivative thereof in the NCFM eSnurra Group's Gjessing et al. 2007, references section excluded. Interestingly, 30% (or 6 of 20) of these word occurrences were used incorrectly, intentionally, and all of the incorrect uses of the word "estimate" pertained to GA (see excerpts below). This was the conflate-to-obfuscate strategy NCFM eSnurra Group used to launch their mission leap claim of GA estimation capability; a capability that did not exist because it was not (and is not) possible. The first excerpt is interesting in that with respect to "traditional approaches" the authors state: "The estimation methods are solely aimed at computing gestational age." Again, even when referring to the "traditional approach" the authors conflate estimation of gestational age with "computing gestational age." Traditional methods predict/estimate gestational age to establish a predicted/estimated number of days from LMPD to the ultrasound date to establish a predicted/estimated LMPD from which GA is established on the date of the ultrasound, just as NCFM eSnurra Group predict/estimate the number of days remaining from the ultrasound exam to delivery date to establish a predicted/estimated EDD. The reason the "the true problem of prediction of term is hardly ever mentioned, let along made explicit" among those using the "traditional approach" is because predicting/estimating EDD is not possible using the "traditional approach," EDD must be calculated when using the "traditional approach," just as predicting/estimating GA is not possible using the NCFM eSnurra Group's approach (i.e., the appropriated Hutchon Method of PDEE) because GA must be calculated when using the NCFM eSnurra Group's Group's approach (i.e., the appropriated Hutchon Method of PDEE). Consequently, the authors must also believe:
- The estimation methods are solely aimed at computing EDD at the time of the ultrasound examination; the true problem of prediction of GA is hardly ever mentioned, let alone made explicit, except for an ‘understanding’ that a certain number of days should be subtracted from the estimated date of delivery of pregnancy. Ergo: The NCFM eSnurra Group's approach of constructing reference charts has a number of weaknesses.
- "The traditional approach of constructing reference charts has a number of weaknesses. The reference material needs to be based on a highly selected group of women with LMP dates as precise as possible. This has led many researchers to avoid population-based materials, which they see as less reliable than prospective studies. The estimation methods are solely aimed at computing gestational age at the time of the ultrasound examination; the true problem of prediction of term is hardly ever mentioned, let alone made explicit, except for an ‘understanding’ that a certain number of days should be added to the estimated start of pregnancy." (Source: p. 20, same as above)
- "Our primary focus in this paper has been on prediction of term. It is interesting to note that the approach also provides estimates for gestational age at the time of the ultrasound examination." (Source: same as above, p. 26)
- "It is interesting to note that the approach also provides estimates for gestational age at the time of the ultrasound examination. This can be done by assuming a typical length of pregnancy of, for instance, 282 days 12, 33. For a given BPD or FL value, one can then subtract the predicted remaining time from the total length of 282 days and thus obtain an estimate of gestational age. The strength of this approach is that it is almost entirerly independent of LMP, and fully population based." (Source: p. 27, same as above)
Conflate-to-Obfuscate: Retrospective and Prospective
NCFM eSnurra Group appears to believe because the ultrasound-based fetal metric measurements that comprise their 1987–2004 dataset were made before the actual birth/delivery, that this somehow qualified their study as prospective instead of retrospective. Again, this conflate-to-obfuscate strategy requires temporally-challenged thinking, as it implies NCFM eSnurra Group believe all ultrasound studies on pregnancy, in the world, are therefore prospective because birth/delivery occurs after pregnancy. The thing that makes a prospective study prospective is that it is designed (i.e., hypothesis fully formulated, methods established, etc.) before subjects are enrolled and baseline data are collected and before any subjects develope the outcome(s) of interest or the outcomes are known. In general, prospective studies are rated higher among researchers in terms of their reliability and significance of evidence relative to retrospective studies. Also, prospective studies are generally more expensive than retrospective studies. Ergo, by identifying their study as prospective, NCFM eSnurra Group were able to reap the benefits of: 1) a higher rated study by leeching the halo effects of true prospective studies, 2) significantly lower cost per observation of a retrospective database study via the incredibly low cost of collecting historical ultrasound and birth/delivery data from government databases, 3) an incredibly high return of perceived study rating on a small investment (i.e., low cost of collecting historical data from government databases) and 3) the word "prospective" included in their study to ensure inclusion in computer searches seeking matches on the word "prospective." NCFM eSnurra Group had used the conflate-to-obfuscate strategy to "game the system," successfully. What could be next: Possibly, an arbitrage market for existing retrospective ultrasound studies relabeled as prospective studies? Ironically, NCFM eSnurra Group made this very point about prospective vs. retrospective studies in their Gjessing et al. 2007 (except below); the very publication NCFM eSnurra Group claimed was a prospective study.
- "This has led many researchers to avoid population-based materials, which they see as less reliable than prospective studies." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p.20)
Interestingly, in the abstract of Gjessing et al. 1999 titled "Errors in Gestational Age: Evidence of Bleeding Early in Pregnancy" authors used gestational age data from the Medical Birth Registry of Norway. Consequently, the authors, including the lead author, NCFM Group's Håkon K. Gjessing, were compelled to include this caution statement regarding "the retrospective nature of the data" (excerpt below, emphasis added).
- "Furthermore, there is evidence for a strong relationship between bleeding at the time of the next menstrual period after conception and low birthweight. This conclusion should be approached with caution because of the retrospective nature of the data. (Am J Public Health. 1999;89:213-218)" (Source: "Errors in Gestational Age: Evidence of Bleeding Early in Pregnancy" Håkon K. Gjessing, PhD, Rolv Skjcerven, PhD, and Allen J. Wilcox, MD, PhD, American Journal of Public Health, February 1999, Vol. 89, No. 2 , p. 213)
- "A retrospective database study of CRL in first-trimester embryos was conducted in a fetal medicine referral center with a predominantly Caucasian population." (Source: "New crown–rump length curve based on over 3500 pregnancies" A. Pexsters, A. Daemen, C. Bottomley, D. Van Schoubroeck, L. De Catte, B. De Moor, T. D'Hooghe, C. Lees, D. Timmerman, T. Bourne, Ultrasound in Obstetrics & Gynacology, 28 May 2010, DOI: 10.1002/uog.7654)
- "Although validated internally, our own reference curve needs to be validated externally by testing it prospectively on a different study population to assess its reproducibility." (Source: same as above)
- "Large databases represent advantages when conducting statistical analysis, but carry inherent weaknesses when it comes to controlling the quality of the material. We therefore believe that the authors' new method of calculating the remaining days of pregnancy should be tested in a prospective study." (Source: "Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection" T. Kiserud, S. L. Johnsen, S. Rasmussen. Ultrasound in Obstetrics & Gynecology Volume 31, Issue 2, February 2008, Page 225. DOI: 10.1002/uog.5204)
- "The authors state in the Abstract that their study was based on data collected prospectively. We cannot see that this classification is justified since there is no information that the measurements were taken with the object of developing a new method according to a protocol established before the data collection started. Rather, this study is a retrospective analysis of a population that attended the ultrasound unit either for a routine second-trimester scan or based on a clinical indication." (Source: ibid.)
- Methods Our data consisted of 41 343 ultrasound scans from a non-selected population, prospectively collected during the years 1987–2004. (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p. 19)
- Conclusions This direct ultrasound-based prediction of term using population-based data avoids selection biases possibly present in smaller prospective samples. (Source: ibid., p. 19)
- This has led many researchers to avoid population-based materials, which they see as less reliable than prospective studies. (Source: ibid., p. 20)
- In addition, owing to limited resources, the sample size of such prospective studies is usually limited to around 500 pregnancies and a few ultrasound operators. (Source: ibid., p. 20)
- A population-based prediction model has several advantages over traditional small prospective studies. (Source: ibid., p. 23)
- The traditional prospective approach is often based on the work of a few or even only two ultrasound operators 23, whereas our population data include a range of operators, from those with experience of more than 5000 scans to operators with a more modest contribution. (Source: ibid., p. 23-24)
- Traditional small prospective studies enroll equally many pregnant women at all BPD and FL values to obtain sufficient data over the entire prediction range. (Source: ibid., p. 26)
- This obviates the need for new prospective studies every time the prediction model needs updating. (Source: ibid., p. 26)
Also, the fourth excerpt above is a disingenuous attempt by the authors to denigrate legitimate prospective studies that may be resource constrained (most are), but what is even more limiting and more important is that the size of a legitimate, prospective study is set by, and strictly limited to, the size established by the statistical power calculation. This is a fact of which NCFM eSnurra Group authors and NCFM eSnurra "copyright owners" Håkon K. Gjessing, PhD of the Norwegian Institute of Public Health and Per Grøttum, MD, PhD, Professor of medical informatics, Section of Medical Informatics, Faculty of Medicine, UiO are very well aware. Nevertheless, they are committed to the NCFM eSnurra Group's agenda; an agenda that necessitates unethical decision-making, on many levels, including research misconduct via plagiarism and falsification.
NCFM eSnurra Group claimed in their Økland et al. 2011 paper (first excerpt below) that the 1987–2005 historical database data were somehow prospectively registered. Again, NCFM eSnurra Group believed their data were prospectively registered 30-years before their study was designed simply because birth/delivery occurs after pregnancy. And, the same thing again, in their Økland et al. 2012 paper (second excerpt below), using 1988–2009 historical database data. Again, these studies were retrospective database studies. As before, NCFM eSnurra Group believe all ultrasound studies on pregnancy, in the world are therefore prospective because birth/delivery occurs after pregnancy. Again, one can only wonder how these papers made if through referees' reviews and then past editorial review before publication in UOG.
- "The clinical measurements in this study originated from the second-trimester routine fetal ultrasound examinations at the National Center for Fetal Medicine at St Olavs University Hospital in Trondheim, Norway, and the data were prospectively registered in an electronic database over the period 1987–2005." (Source: "Narrowed beam width in newer uonlinelibrary.wiley.com/doi/10.1002/uog.8954/pdfltrasound machines shortens measurements in the lateral direction: fetal measurement charts may be obsolete" I. ØKLAND, T. G. BJASTAD, T. F. JOHANSEN, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2011; 38: 82–87 DOI: 10.1002/uog.8954)
- "In a study population of 23 020 second-trimester ultrasound examinations, data were prospectively collected and registered over the period 1988–2009" p. 563 (Source: Advantages of the population-based approach to pregnancy dating: results from 23 020 ultrasound examinations, I. ØKLAND, J. NAKLING, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2012; 39: 563–568, p. 563 DOI: 10.1002/uog.10081)
Secular Trends/Drift & Confounding Variables:
Consider the potential of variances due to secular trends (or secular drift) and/or confounding (or missing) variables over the NCFM eSnurra dataset's 18-years calendar interval that could have had an effect on gestation time. If one or more secular trends did have an effect, the dataset would be correspondingly biased, thus any future predictions/estimations made via corresponding models would be biased. Just as an example, NCFM eSnurra Group's Gjessing et al. 2007 included several covariates, but only birth year range had an effect; a very large effect on FL-based predictions in the last 6-year period of the dataset that went completely unexplained in Gjessing et al. 2007. This was stated to be the result of older ultrasound technology of wider beam widths in the lateral direction of measurement on FL. Papers describing these technology-induced measurement errors were published in the 1980s. However, there may be other potential secular trends and confounding variables masked in historical datasets, which is a common problem among retrospective studies using historical databases. The fact that the secular trend induced in FL measurements as a result of constantly improving ultrasound technology throughout the years 1987–2004 enabled less distorted measurements of FL is a good example of why the study reported in Gjessing et al. 2007 and their other publications were retrospective studies, not prospective studies. Note: remember the -2.3 FL adjustment is added to the days remaining estimate to delivery (not to EDD), thus making the fetus or GA 2.3 days older to compensate for the secular trend of improving ultrasound technology.
- "The only notable effect of the covariates is that of birth year on FL predictions; when applying predictions to future data this covariate should thus be included, using the last time period." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES; Ultrasound Obstet Gynecol 2007: 30: 19–27, p.22)
FL (mm) 1–16 17–21 22–26 27–31 32–36 37–42
Birth year
1987–1992 0.2 0.5 0.7 0.8 0.8 0.7
1993–1998 0.4 0.4 0.5 0.5 0.6 0.7
1999–2004 0.0 −0.5 − 0.9 −1.4 −1.8 −2.3
A Concluding Supposition: An Oxymoron:
There is an agenda-driven supposition (first excerpt below) in the "Conclusions" section of the Abstract of NCFM eSnurra Group's Økland et al. 2010. Additionally, this supposition was not restricted to the Abstract, it also appeared in the body of the paper (second excerpt) where it was stated more as a fact and not as a supposition. A supposition is not a conclusion because a supposition is a belief held without proof or certain knowledge, such as an assumption. In short, a supposition is not a conclusion. The first sentence of the "Conclusion" section of the Abstract contains 17 words (or 31%) of the conclusion, while the second sentence, a supposition contains 38 words (or 69%) of the conclusion. When the "Conclusion" section of a paper's Abstract is filled with 69% supposition it means either: 1) there was little or no resulting evidence to conclude something substantive and/or 2) the authors had a non-science agenda to communicate. Again, one can only wonder how this NCFM eSnurra Group's agenda item made it through referees' reviews and past editorial review before publication in Ultrasound in Obstetrics and Gynecology. It is important to note that NCFM eSnurra Group's Økland et al. 2011 paper did not prove selection was the source of bias. Notice how in the "Conclusion" section the authors state: "These models have important shortcomings, probably because of strict selection criteria..." and 5-pages later the authors state: "The selection criteria of the sample-based models are important in producing these biases." So, which was it? Even though their study did not prove it, the authors were compelled to make their supposition in the "Conclusion" section because they wanted to communicate selection bias, without proof, which was NCFM eSnurra Group's agenda. Ergo, NCFM eSnurra Group's Økland et al. 2010 concluded in a supposition, an oxymoron. Communicating an agenda-driven message in paper published in an academic medical journal speaks to the ethos of scholarship, academic integrity and independence of the authors.
- "Conclusion Term predictions made with traditional sample-based models had significant biases that varied over each method’s measurement range. These models have important shortcomings, probably because of strict selection criteria in the process of constructing the models, and because the methods primarily aim at estimating the last menstrual period-based day of conception, not the day of birth." p. 728. (Source: "Biases of traditional term prediction models: results from different sample-based models evaluated on 41 343 ultrasound examinations" I. ØKLAND, H. K. GJESSING, P. GRØTTUM and S. H. EIK-NES, Ultrasound Obstet Gynecol 2010; 36: 728–734, p. 728. DOI: 10.1002/uog.7707)
- "The selection criteria of the sample-based models are important in producing these biases. Therefore, the more robust population-based approach to all categories of fetal biometry charts 21, 25, 27, 28 should probably supersede the traditional models." (Source: ibid.p. p. 733)
Information Rights & Medical Rights
Despite the obvious effects of increased risks, critical mistakes, grievous harms and negative medical outcomes, this systemic, institutionalized problem of evidence-obviated medicine is an information rights issue as much as it is a problem of intentional recklessness and willful negligence. Not surprisingly, this problem is not limited to Norway. A large part of what makes this problem systemic is articulated by NCFM themselves in the following excerpt from their website.
Smaller Norwegian Towns
In smaller Norwegian towns midwives and doctors conform to what they are told, taught and trained by NCFM and NCFM eSnurra Group. They were told, taught and trained to practice evidence-obviated medicine with respect to obviating a pregnant woman's key pregnancy dates (e.g., LMPD/OTPD/SCID) at the scheduling of a pregnant woman's "routine" 18wUSE, without her prior, informed, voluntary, explicit consent. Consequently, after the ultrasound exam, and during a pregnant woman's next appointment with her midwife or doctor she may learn her gestational calendar has been rest to conform with her assigned ultrasound-based NCFM eSnurra BPD-based EDD & GA, again, without her prior, informed, voluntary, explicit consent. Laila's midwife did not tell her that her GA & EDD calendar had been "corrected" by the ultrasound exam. Laila discovered it by looking at her pregnancy log which her midwife would update for Laila at each appointment. Laila's "corrected" EDD & GA meant Laila was supposed to accept that she and Edward had somehow been mistaken, by 12 days, regarding all of Laila's key pregnancy dates; dates Laila & Edward meticulously recorded in Laila's pregnancy spreadsheet when each presented. In short, Laila's medical professionals expected Laila & Edward to believe 2 + 2 = 5 in the special NCFM eSnurra Group's version of alternative mathematics, but Laila and Edward refused to recognize alternative mathematics and alternative facts i.e., the "official" NCFM eSnurra BPD-based EDD & GA assigned to Laila's pregnancy, again, without Laila's prior, informed, voluntary, explicit consent. Also, Laila was forced to accept a quantified (Gjessing et al. 2007), undisclosed 12.8% risk that her pregnancy would be assigned a grossly inaccurate (i.e., < -14 days or > 14 days) NCFM eSnurra BPD-based EDD and, therefrom, a calculated GA using the equivalent of Naegele's rule, in reverse, that was also grossly inaccurate. No rational pregnant woman would knowingly accept an unnecessary 12.8% risk for herself and her fetus/baby while in ownership possession of a combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD given the only method that could be more accurate is if the woman were to have had an in vitro fertilization date (IVFD) to establish the beginning of her pregnancy, which would only be more accurate in terms of hours, not weeks and days. Moreover, there is no arguing this point with either logic, basic human biology or basic gestational mathematics because all discussions and arguments with Laila's medical professionals ended with "this is how we do it in Norway" or "this is The Rule" or "these are the Norwegian guidelines" (i.e., mandate). So, Laila and Edward were told to get on board with NCFM eSnurra Group's alternative mathematics and alternative facts and believe 2 + 2 = 5, just as all of Laila's medical professionals had been told, taught and trained to believe, no matter what contradictory medical evidence was available.
In summary, at the scheduling of Laila's "routine" 18wUSE, Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD, and all of Laila's other key pregnancy dates, were obviated, without Laila's prior, informed, voluntary, explicit consent. These key pregnancy dates, especially the combined, fully corroborating, factual LMPD/OTPD/SCID were medical evidence that would neither be be seen nor used again by any of Laila's medical professionals. Unfortunately, it was apparent Laila's medical professionals were doing exactly as they had been told, taught and trained, and with a decidedly pride-filled attitude. Consequently, Norway's medical professionals' medical thinking had been compromised by Norwegian Directorate of Health's medically & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine. In the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
NCFM: eSnurra: Institutionalized Systemic Problem
It is the training from NCFM and NCFM eSnurra Group that conditions Norway's doctors and midwives into the cognitive behaviors of institutionalized confirmation bias and doublethink which result in critical medical mistakes; critical medical mistakes such as assigning a grossly inaccurate NCFM eSnurra BPD-based EDD & GA to a pregnancy while masking an FGR/malformation or other fetal pathology by assigning a grossly inaccurate, younger, GA to the fetus/baby (i.e., grossly smaller than accurately average BPD head measurement = grossly smaller age = grossly big mistake) and preventing the routine turning of a fetus/baby from breech to vertex, in time, before the onset of labor; critical medical mistakes that increase medical risks and cause grievous medical harms to some of Norway's women and their fetuses/babies. And, insidiously, there is absolutely nothing in place to stop this, yet. Moreover, these critical medical mistakes are silently and invisibly written off, unattributed, undocumented & unreported, as acceptable collateral damage of Directorate of Health's medically & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation. Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Included below is the morning session agenda of the first day of the NCFM 25 Years Anniversary Symposium (Jubileumssymposium, Nasjonalt senter for fostermedisin – 25 år) which reads as if it were an NCFM eSnurra Group medico-marketing event to spread evidence-obviated medicine. Also, it is interesting to note that all of the prime-time morning session speakers are authors of the four papers included in Inger Økland's 2012 NTNU dr.philos. Thesis; the academically compromised thesis used by Directorate of Health to justify their medically & ethically flawed 2014 Recommendation within a government-mandated protocol of evidence-obviated medicine at the scheduling of the routine 18wUSE.
Despite the obvious effects of increased risks, critical mistakes, grievous harms and negative medical outcomes, this systemic, institutionalized problem of evidence-obviated medicine is an information rights issue as much as it is a problem of intentional recklessness and willful negligence. Not surprisingly, this problem is not limited to Norway. A large part of what makes this problem systemic is articulated by NCFM themselves in the following excerpt from their website.
- "NSFM teaches and trains midwives and doctors in ultrasound diagnostics both in Norway and abroad. In cooperation with the Norwegian University in Technology (NTNU), the center develops new procedures and technologies in fetal medicine. The center is a WHO collaborating center for diagnostic ultrasound in obstetrics and gynecology." (Source: NCFM website
Directorate of Health's Johan Torgersen and Torunn Janbu did no small amount of marketing & promotion for NCFM eSnurra Group in their article "Directorate of Health - and eSnurra" ("Helsedirektoratets rolle – og eSnurra") published in Dagens Medisin, 2015-04-13. However, the last sentence is a bit confusing in English and Norwegian. - "EASILY ACCESSIBLE. eSnurra has been developed at the National Center for Fetal Medicine (NSFM) in Trondheim, in collaboration with the Department of Medical Informatics at the University of Oslo and the National Public Health Institute. eSnurra as a national tool is readily available as a plastic wheel and there is an open available online version (www.esnurra.no). It is also available as an app for Android, iPhone, iPad-installed in over 90 countries as well as Norway. After performing traditional ultrasound measurements of the head and thigh, the data can be used in all modern ultrasound machines."
("LETT TILGJENGELIG. eSnurra er utviklet ved Nasjonalt senter for fostermedisin (NSFM) i Trondheim i samarbeid med Seksjon for medisinsk informatikk ved Universitetet i Oslo og Nasjonalt Folkehelseinstitutt. eSnurra som nasjonalt verktøy er lett tilgjengelig som et plasthjul og det finnes en åpen tilgjengelig nettversjon (www.esnurra.no). Den finnes også som app for Android, iPhone, iPad –installert i over 90 land i tillegg til Norge. Etter å ha foretatt tradisjonelle ultralydmålinger av hode og lårbein, kan dataene brukes i alle moderne ultralydmaskiner.")
(Source: DEBATT OG KRONIKK "Helsedirektoratets rolle – og eSnurra" Skrevet av: Johan Torgersen / Torunn Janbu. Dagens Medisin. Publisert: 2015-04-13 11.49)
Smaller Norwegian Towns
In smaller Norwegian towns midwives and doctors conform to what they are told, taught and trained by NCFM and NCFM eSnurra Group. They were told, taught and trained to practice evidence-obviated medicine with respect to obviating a pregnant woman's key pregnancy dates (e.g., LMPD/OTPD/SCID) at the scheduling of a pregnant woman's "routine" 18wUSE, without her prior, informed, voluntary, explicit consent. Consequently, after the ultrasound exam, and during a pregnant woman's next appointment with her midwife or doctor she may learn her gestational calendar has been rest to conform with her assigned ultrasound-based NCFM eSnurra BPD-based EDD & GA, again, without her prior, informed, voluntary, explicit consent. Laila's midwife did not tell her that her GA & EDD calendar had been "corrected" by the ultrasound exam. Laila discovered it by looking at her pregnancy log which her midwife would update for Laila at each appointment. Laila's "corrected" EDD & GA meant Laila was supposed to accept that she and Edward had somehow been mistaken, by 12 days, regarding all of Laila's key pregnancy dates; dates Laila & Edward meticulously recorded in Laila's pregnancy spreadsheet when each presented. In short, Laila's medical professionals expected Laila & Edward to believe 2 + 2 = 5 in the special NCFM eSnurra Group's version of alternative mathematics, but Laila and Edward refused to recognize alternative mathematics and alternative facts i.e., the "official" NCFM eSnurra BPD-based EDD & GA assigned to Laila's pregnancy, again, without Laila's prior, informed, voluntary, explicit consent. Also, Laila was forced to accept a quantified (Gjessing et al. 2007), undisclosed 12.8% risk that her pregnancy would be assigned a grossly inaccurate (i.e., < -14 days or > 14 days) NCFM eSnurra BPD-based EDD and, therefrom, a calculated GA using the equivalent of Naegele's rule, in reverse, that was also grossly inaccurate. No rational pregnant woman would knowingly accept an unnecessary 12.8% risk for herself and her fetus/baby while in ownership possession of a combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD given the only method that could be more accurate is if the woman were to have had an in vitro fertilization date (IVFD) to establish the beginning of her pregnancy, which would only be more accurate in terms of hours, not weeks and days. Moreover, there is no arguing this point with either logic, basic human biology or basic gestational mathematics because all discussions and arguments with Laila's medical professionals ended with "this is how we do it in Norway" or "this is The Rule" or "these are the Norwegian guidelines" (i.e., mandate). So, Laila and Edward were told to get on board with NCFM eSnurra Group's alternative mathematics and alternative facts and believe 2 + 2 = 5, just as all of Laila's medical professionals had been told, taught and trained to believe, no matter what contradictory medical evidence was available.
In summary, at the scheduling of Laila's "routine" 18wUSE, Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA & EDD, and all of Laila's other key pregnancy dates, were obviated, without Laila's prior, informed, voluntary, explicit consent. These key pregnancy dates, especially the combined, fully corroborating, factual LMPD/OTPD/SCID were medical evidence that would neither be be seen nor used again by any of Laila's medical professionals. Unfortunately, it was apparent Laila's medical professionals were doing exactly as they had been told, taught and trained, and with a decidedly pride-filled attitude. Consequently, Norway's medical professionals' medical thinking had been compromised by Norwegian Directorate of Health's medically & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation with their exclusive implementation of NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) within a government-mandated protocol of evidence-obviated medicine. In the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
NCFM: eSnurra: Institutionalized Systemic Problem
It is the training from NCFM and NCFM eSnurra Group that conditions Norway's doctors and midwives into the cognitive behaviors of institutionalized confirmation bias and doublethink which result in critical medical mistakes; critical medical mistakes such as assigning a grossly inaccurate NCFM eSnurra BPD-based EDD & GA to a pregnancy while masking an FGR/malformation or other fetal pathology by assigning a grossly inaccurate, younger, GA to the fetus/baby (i.e., grossly smaller than accurately average BPD head measurement = grossly smaller age = grossly big mistake) and preventing the routine turning of a fetus/baby from breech to vertex, in time, before the onset of labor; critical medical mistakes that increase medical risks and cause grievous medical harms to some of Norway's women and their fetuses/babies. And, insidiously, there is absolutely nothing in place to stop this, yet. Moreover, these critical medical mistakes are silently and invisibly written off, unattributed, undocumented & unreported, as acceptable collateral damage of Directorate of Health's medically & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation. Again, in the sage economy of words of Bergen Group and NGF, this is "medically flawed" and "can be directly dangerous," respectively.
Included below is the morning session agenda of the first day of the NCFM 25 Years Anniversary Symposium (Jubileumssymposium, Nasjonalt senter for fostermedisin – 25 år) which reads as if it were an NCFM eSnurra Group medico-marketing event to spread evidence-obviated medicine. Also, it is interesting to note that all of the prime-time morning session speakers are authors of the four papers included in Inger Økland's 2012 NTNU dr.philos. Thesis; the academically compromised thesis used by Directorate of Health to justify their medically & ethically flawed 2014 Recommendation within a government-mandated protocol of evidence-obviated medicine at the scheduling of the routine 18wUSE.
- Anniversary Symposium National Center for Fetal Medicine - 25 years
Program
Wednesday June 1
Start June 1, 2016, kl. 10.00, End kl. 17.30.
Part 1 - Symposium on eSnurra, age, term, growth
10:00 Sturla H. Eik-Nes Introduction
10:15 Håkon Gjessing Principle for eSnurra as population-based predictive tools
10:40 Sturla H. Eik-Nes Clinical results for the prediction of term, the use of electronic versions
11.00 Break
11:20 Inger Økland National validation of predictive tools for term
11:40 Sturla H. Eik-Nes Complex term and age
5.12 Håkon Gjessing Population based estimation of growth and growth abnormalities, actual weight for age curves and estimated weight for age curves
12:40 Torbjørn Moe Eggebø Weight estimation at week 41-consultation
(Source: Jubileumssymposium; also see St Olavs Communications Department report: "A quarter of a century as a fetal advocate" "Et kvart århundre som fosterets advokat" Av Frode Nikolaisen, Publisert 02.06.2016, Sist oppdatert 23.08.2018)
NCFM eSnurra Group's Calculation of Gestational Age (GA) is Flawed & Cavalier
The gestational age (GA) calculated by NCFM eSnurra Group from the estimated end of pregnancy (i.e., the wrong end) using the equivalent of Naegele's rule, in reverse, provides different results depending on which NCFM eSnurra Group platform is used (i.e., NCFM eSnurra pregnancy wheel, website, iOS app or Android app). To say this is a flawed and cavalier approach to establishing consistent "official" medical GA for all pregnancies and abortions in Norway would be an understatement and serves as additional confirmation of the explicit warnings issued by NGF and Bergen Group.
The gestational age (GA) calculated by NCFM eSnurra Group from the estimated end of pregnancy (i.e., the wrong end) using the equivalent of Naegele's rule, in reverse, provides different results depending on which NCFM eSnurra Group platform is used (i.e., NCFM eSnurra pregnancy wheel, website, iOS app or Android app). To say this is a flawed and cavalier approach to establishing consistent "official" medical GA for all pregnancies and abortions in Norway would be an understatement and serves as additional confirmation of the explicit warnings issued by NGF and Bergen Group.
- "We hold the opinion that this recommendation is medically flawed and that the Directorate has conducted a muddled investigation process." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "...the basis for determining gestational age is not the end of the pregnancy, but its beginning." (Source: ibid.)
- "eSnurra
The new EDD method.
eSnurra is a population based method for determining the gestational age, the estimated date of delivery and the weight of a fetus."
- "eSnurra is an evolution of the old “Snurra” that has been in use in Norway from 1984 until eSnurra came in the first edition in 2007."
|
NCFM eSnurra Group's Android app
© Eik-Nes, Grøttum and Gjessing Version 2.0.3 Updated on Sep 21, 2015 Test date: 25.09.2017 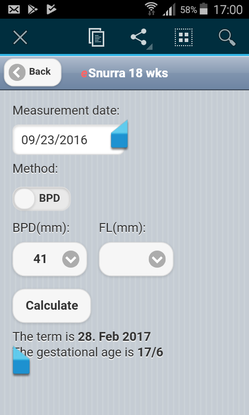
|
NCFM eSnurra Group's Website
© 2007 Eik-Nes, Grøttum og Gjessing Version [not identified] Test date: 25.09.2017 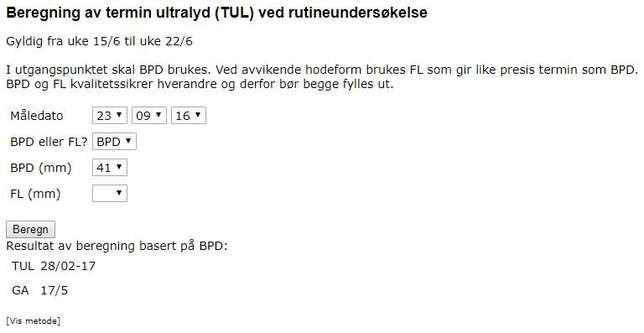
|
|
Test date: 25.09.2017 Using NCFM eSnurra Group's Android app:
|
Test date: 25.09.2017 Using the NCFM eSnurra Group's Website:
|
- The FL & BPD measurements used in the test were identical, 29 mm and 41 mm, respectively, for both NCFM eSnurra Group's Android APP and their Website; and, the ultrasound date was also identical, all of which can be confirmed by comparing the values in the 2 screen images above. Moreover, the, NCFM eSnurra Group's Android APP had been downloaded on the same date as the test, 25.09.2017. Consequently, the Android APP version was current.
- Therefore, not only is BPD recognized, internationally, as a problematic, unreliable predictor/estimator during routine ultrasound exams, NCFM eSnurra Group's calculation of NCFM eSnurra BPD-based GA, using the equivalent of Naegele's rule, in reverse, is also problematic in that it is not consistent across NCFM eSnurra Group's platforms. [Note: NCFM eSnurra Group's iOS app was not tested.]
- The EDD provided by NCFM eSnurra Group's Android APP and Website for BPD = 41 mm were identical, 28.02.2017 (grossly inaccurate); however, the GAs (also grossly inaccurate) were not identical, but should have been. If NCFM eSnurra Group's current Website version, using a 282-day gestation period instead of NCFM eSnurra Group's 283-day gestation period were to have been used for Laila's pregnancy to establish Laila's NCFM eSnurra BPD-based EDD and, therefrom, calculated Laila's GA, using the equivalent of Naegele's rule, in reverse, then Laila's GA would have been 1-day younger, and her baby would have been delivered (via an unwanted, unnecessary Cesarean section surgery) as preterm at NCFM eSnurra BPD-based GA = 36w+6. (Note: GA < 37w+0 at birth/delivery is the definition of preterm.) Again, Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA = 38w+5 at delivery on 04.02.2017.
- Sometime after Laila's pregnancy NCFM eSnurra Group created a veritable 1-day GA arbitrage opportunity. When one wants or needs a pregnancy or fetus to have an "official" medical GA which is 1-day younger than the GA calculated from the estimated end of pregnancy (i.e., the wrong end) using the equivalent of Naegele's rule, in reverse, via NCFM eSnurra Group's Android APP, one can simply use their Website platform for an "official" medical GA which is 1-day younger.
- "...[NCFM eSnurra Group's "method"] provides women seeking abortion with equality before the law." (Source: "One Norwegian national tool for estimating date of delivery and fetal age" or in Norwegian ("Nasjonalt verktøy for bestemmelseav termin og fosteralder") Torunn Janbu, Tidsskr Nor Legeforen nr. 9, 2016; 136: 790 – 1)
- "The outcome of an application for abortion may depend on which model is used." (Source: ibid.)