BPD Is Problematic
BPD Is a Problematic, Unreliable Estimator of GA or EDD During Routine Ultrasound Exams
It is important to understand that during Laila's routine 18wUSE the problematic, inaccurate BPD was measured and used to estimate a grossly inaccurate BPD-based eSnurra EDD which was then used to calculate a correspondingly grossly inaccurate GA using the equivalent of Naegele's rule, in reverse. The exclusive reliance of NCFM eSnurra Group on BPD for EDD estimation and, therefrom, GA calculation was a critical medical mistake which led to a cascade of subsequent critical medical mistakes and grievous medical harms. If, however, the more robust head circumference (HC) had been used (as in Bergen Group's protocol) instead of, or in conjunction with, BPD, then Laila would not have endured an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications and her baby would not have endured an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head. In short, BPD is known, internationally, as a problematic, unreliable predictor during routine ultrasound exams and should be replaced with the more robust HC, or BPD should only be used in conjunction with HC to keep it in check, to directly estimate GA and, therefrom calculate EDD (i.e., the Campbell Method of GA Estimation) or directly estimate EDD (i.e., the Hutchon Method of PDEE) and, therefrom, calculate GA, during routine ultrasound exams. However, because NCFM eSnurra Group is dependent on BPD as the one and only fetal head metric in their fetal metrics models inventory, when they encounter an abnormal fetal head shape, i.e., provided the fetal head shape is recognized as abnormal, they either "correct" BPD with a mathematical approximation to create an adjusted or expanded virtual BPD to ensure a more accurate estimate of EDD and, therefrom, calculate a more accurate GA, or they switch from BPD to femur length (FL) to directly estimate EDD. If neither of these BPD corrections are made, a grossly inaccurate NCFM eSnurra BPD-based EDD is inevitable.
The Fundamental Problem of BPD is of Basic Geometry & Information Capacity
BPD, the biparietal diameter (or ear-to-ear diameter) is just that, a diameter, which, by definition is a line segment in 1-spacial dimension passing through the radius of a circle. However, the fetal head, not surprisingly, is neither a circle nor sphere. Because BPD is a diameter of 1-spacial dimension, it captures limited information about the size of the fetal head and the shape of the fetal head. On the other hand, had circumference (HC) captures information in 2-spacial dimensions perpendicular to each other while remaining nearly insensitive to head shape. HC is typically measured using 1 of 2 methods: direct or derived:
Unreliable, Problematic BPD: Inconvenient to NCFM eSnurra Group's Agenda
The 2 excerpts below were taken from NCFM Snurra Group's Tunón et al. 2000 in which the data identified, if not screamed, BPD was a problematic, unreliable predictor of GA, with a discrepancy of 14 days between BPD-based GA and IVF-based GA (i.e., actual GA), similar 14 day discrepancies between IVF-based GA and BPD-based GA were confirmed by Wennerholm et al. 1998 and, of course, Tunon et al. 1999. Also, Tunón et al. 2000 reported discrepancies greater than 7 days were either "not present or were very small" in corresponding CRL-based GA estimates of the same fetuses. Ergo, for NCFM eSnurra Group, this data-supported evidence of BPD being problematic and unreliable was somehow switched into a discussion of women's "unreliable" LMP for which Tunón et al. 2000 cited ... wait for it ... Tunón et al. 1998 in which this gleaming gem of a BPD apologist's statement was found, among others, (p. 22):
Interestingly and ironically, Tunón et al. 2000 is the 2nd citation in Wikipedia's entry for Gestational age for IVF-based GA, the 3rd dot point in the "Methods" section as follows:"
Laila and her baby, and other women and their babies, endured increased medical risks, critical medical mistakes and grievous medical harms, which were silently and invisibly written off, unattributed, undocumented and unreported, as acceptable collateral damage of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. Again, BPD is a problematic, unreliable predictor of GA & EDD independent of the prediction method (i.e. Campbell's Method of GA Estimation or Hutchon's Method of PDEE) during routine ultrasound exams, but this fact was (and remains) inconvenient to NCFM eSnurra Group's agenda of promoting the second-trimester ultrasound exams for NCFM eSnurra BPD-based EDD and, therefrom, a calculated GA using the equivalent of Naegele's rule, in reverse; and, replacing any first-trimester EDD & GA values with inherently less accurate second-trimester EDD & GA values for all pregnancies and abortions in Norway. Moreover, this internationally recognized BPD problem is inconvenient to NCFM eSnurra Group's prediction/estimation capabilities, i.e., NCFM eSnurra Group's model inventory does not include the more robust, 2-spacial dimensions HC measurement as a predictor/estimator of EDD. And, similar to used car dealers, NCFM eSnurra Group believes it must sell what is currently in inventory; and, BPD is the entire fetal head metric inventory of NCFM eSnurra Group's "method."
Multiple Studies: BPD Inferior to HC for Establishing GA & EDD
Setting the Standard: The Seminal Altman & Chitty 1997 Study
A seminal Altman & Chitty, 1997 study concluded BPD was problematic and unreliable due to its inability to deal with abnormal fetal head shapes and sizes as stated in the excerpts below.
A 1981 study established that "variations in the shape of the fetal skull...may adversely affect the accuracy of the biparletal diameter (BPD) measurement in estimating fetal age."
A 1988 study, found there were different BPD growth trajectories between males and females leading to the conclusion dating pregnancies by BPD can lead to error.
A 1998 study to assess the accuracy of fetal biometry in mid-trimester of pregnancy in the assignment of fetal age found: "Head circumference was the best predictor of gestational age."
A 2004 study (below) states multiple problems in using BPD and recommends using head circumference (HC) as the "more robust method" for fetal age assessment.
A 2005 study concluded FL/HC is a more robust than FL/BPD for characterizing fetal proportions and that FL is an equally robust method as HC to assess fetal age.
A 2006 study states that HC and BPD predicted spontaneous birth with a mean accuracy of one day, HC being better than BPD.
The following excerpt cites work from 2007 that showed HC outperformed BPD for dolichocephalic fetuses as "a good reason for contemplating using HC rather than BPD."
In a 2008 Correspondence letter regarding the article: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection," presented evidence of "a good reason for contemplating using HC rather than BPD."
In 2010 the ISUOG Prenatal Ultrasound Screening Task Force published their Practice Guidelines for Performance of the Routine Mid-Trimester Fetal Ultrasound Scan which cautioned that BPD "can lead to misleading estimates of fetal age" and that "HC is more reliable."
In 2013 The American Institute of Ultrasound in Medicine (AIUM) published their AIUM Practice Parameter for the Performance of Obstetric Ultrasound Examinations in which they warned about the problems with BPD and explained HC is more robust (excerpts below). Also, AIUM made the argument that LMPD should be used to test the reasonableness of ultrasound-based GA and as evidence of potential fetal pathology when there are "Significant discrepancies between gestational (menstrual) age and fetal measurements" (first excerpt below). Apparently, AIUM advocates for the inclusion of LMPD/OTPD in the practice of evidence-based medicine, not Directorate of Health and NCFM eSnurra Group's protocol of obviating LMPD et al. at the 18wUSE in the practice of evidence-obviated medicine.
In February 2014 the Society of Obstetricians and Gynaecologists of Canada (SOGC) published their "Clinical Practice Guidelines: Determination of Gestational Age by Ultrasound. No. 303" in the Journal of Obstetric and Gynaecology Canada (JOGC) which stated the following.
In 2016 The American College of Obstetrician and Gynecologists (ACOG) & American Institute of Ultrasound in Medicine issued a Practice Bulletin that explicitly stated: "the head circumference is the single most-predictive parameter of gestational age..."
A 2018 UpToDate literature review includes the following.
The 2019 "ISUOG Practice Guidelines: ultrasound assessment of fetal biometry and growth" state the following with respect to accurate estimation of gestational age.
Data Irregularities Not Explained
In 2015 NCFM eSnurra Group were asked to explain BPD data irregularities (excerpts below). Moreover, these identified data irregularities were known to Directorate of Health, but Directorate of Health decided to ignore them.
Model Sensitivity vs. Patient Sensitivity
At Laila's routine 18wUSE, i.e., after all her key pregnancy dates had been discarded by a government-mandated protocol of evidence-obviated medicine implemented in conjunction with NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE), without Laila's prior, informed, voluntary, explicit consent, Laila's baby's BPD was measured to generate NCFM eSnurra BPD-based EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse. However, Laila's assigned NCFM eSnurra BPD-based EDD was grossly inaccurate and resulted in increased medical risks, critical medical mistakes and grievous medical harms; and, given the NCFM eSnurra BPD-based EDD assigned to Laila's pregnancy had been proven to be grossly inaccurate by Laila's combined, fully corroborating, factual LMPT/OTPD/SCID-based EDD by 14-days, there was bound to be a significant prediction error, and there was, a prediction error = (predicted (set to 0) - actual) = -24 days, more than 3 weeks, 3w+3, just 4 days shy of a full menstrual cycle/period, technically classified as a preterm by NCFM eSnurra Group's published criteria (see prediction errors bar-chart frequency distribution below).
It is important to understand that during Laila's routine 18wUSE the problematic, inaccurate BPD was measured and used to estimate a grossly inaccurate BPD-based eSnurra EDD which was then used to calculate a correspondingly grossly inaccurate GA using the equivalent of Naegele's rule, in reverse. The exclusive reliance of NCFM eSnurra Group on BPD for EDD estimation and, therefrom, GA calculation was a critical medical mistake which led to a cascade of subsequent critical medical mistakes and grievous medical harms. If, however, the more robust head circumference (HC) had been used (as in Bergen Group's protocol) instead of, or in conjunction with, BPD, then Laila would not have endured an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications and her baby would not have endured an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head. In short, BPD is known, internationally, as a problematic, unreliable predictor during routine ultrasound exams and should be replaced with the more robust HC, or BPD should only be used in conjunction with HC to keep it in check, to directly estimate GA and, therefrom calculate EDD (i.e., the Campbell Method of GA Estimation) or directly estimate EDD (i.e., the Hutchon Method of PDEE) and, therefrom, calculate GA, during routine ultrasound exams. However, because NCFM eSnurra Group is dependent on BPD as the one and only fetal head metric in their fetal metrics models inventory, when they encounter an abnormal fetal head shape, i.e., provided the fetal head shape is recognized as abnormal, they either "correct" BPD with a mathematical approximation to create an adjusted or expanded virtual BPD to ensure a more accurate estimate of EDD and, therefrom, calculate a more accurate GA, or they switch from BPD to femur length (FL) to directly estimate EDD. If neither of these BPD corrections are made, a grossly inaccurate NCFM eSnurra BPD-based EDD is inevitable.
The Fundamental Problem of BPD is of Basic Geometry & Information Capacity
BPD, the biparietal diameter (or ear-to-ear diameter) is just that, a diameter, which, by definition is a line segment in 1-spacial dimension passing through the radius of a circle. However, the fetal head, not surprisingly, is neither a circle nor sphere. Because BPD is a diameter of 1-spacial dimension, it captures limited information about the size of the fetal head and the shape of the fetal head. On the other hand, had circumference (HC) captures information in 2-spacial dimensions perpendicular to each other while remaining nearly insensitive to head shape. HC is typically measured using 1 of 2 methods: direct or derived:
- Direct: HC is estimated by fitting a digital ellipse function (built into ultrasound machines' software) to the fetal head contour
- Derived: HC is calculated from 2 fetal head diameter measurements perpendicular to each other, BPD (ear-to-ear diameter) and OFD, the ociptio-frontal diameter (back-to-front diameter) via the averaging of the 2 diameters: HC = pi x (BPD + OFD)/2, or by using other similar equations tuned with a model-based constant.
Unreliable, Problematic BPD: Inconvenient to NCFM eSnurra Group's Agenda
The 2 excerpts below were taken from NCFM Snurra Group's Tunón et al. 2000 in which the data identified, if not screamed, BPD was a problematic, unreliable predictor of GA, with a discrepancy of 14 days between BPD-based GA and IVF-based GA (i.e., actual GA), similar 14 day discrepancies between IVF-based GA and BPD-based GA were confirmed by Wennerholm et al. 1998 and, of course, Tunon et al. 1999. Also, Tunón et al. 2000 reported discrepancies greater than 7 days were either "not present or were very small" in corresponding CRL-based GA estimates of the same fetuses. Ergo, for NCFM eSnurra Group, this data-supported evidence of BPD being problematic and unreliable was somehow switched into a discussion of women's "unreliable" LMP for which Tunón et al. 2000 cited ... wait for it ... Tunón et al. 1998 in which this gleaming gem of a BPD apologist's statement was found, among others, (p. 22):
- "Most probably there is an over-representation of genetically small fetuses in the study group that could explain the small shift in the median day of delivery. Such a shift of 3 days may be caused by the BPD being 1–2 mm smaller than the median." (p. 22)
- "There seems to be a difference of approximately 1–2 days between the estimates of gestational age from IVF and from ultrasound. However, in the individual embryo/fetus the difference between the gestational age estimated by IVF and BPD could be as much as 14 days; this has been observed both in the present and a previous study 9. We looked at the cases with a difference of more than 7 days between any two of the three different estimates and in the majority of cases a difference of more than 7 days was found between the IVF and the BPD estimates and were not present or were very small at the time of the CRL measurement." p. 44
- "In pregnancies where gestational age has been calculated from both the last menstrual period and the BPD measurement, differences of more than 14 days between the two estimates have been observed in 6% 5. In 83% of these pregnancies the gestational age was shorter according to the ultrasound method. It is of interest to note that in the present and a previous study 9 on pregnancies conceived by IVF no case with a difference of more than 14 days between the IVF estimate and the BPD estimate was found. A difference of more than 7 days between IVF and CRL estimates was found in only three fetuses. This supports the assumption that large differences between gestational age estimated by the last menstrual period and ultrasound are caused by unreliability in the last menstrual period estimate and not by pathology in the fetus 15." (Source: "Gestational age in pregnancies conceived after in vitrofertilization: a comparison between age assessed from oocyteretrieval, crown-rump length and biparietal diameter" K. TUNON, S.H. EIK-NES, P. GRØTTUM, V. VON DU¨RING and J.A. KAHN. Ultrasound Obstet Gynecol 2000; 15: 41–46,. p 44) [Note 1: Citation "5" above is: "5 Tunon K, Eik-Nes SH, Grøttum P. A comparison between ultrasound and a reliable last menstrual period as predictors of the day of delivery in 15 000 examinations. Ultrasound Obstet Gynecol 1996; 8: 178–85] [Note 2: Citation "9" above is: "9 Wennerholm U-B, Berg C, Hagberg H, Sultan B, Wennergren M. Gestational age in pregnancies after in vitro fertilization: comparison between ultrasound measurements and actual age. Ultrasound Obstet Gynecol 1998; 12: 170–4] [Note: 3: Citation "15" above is: "15 Tunon K, Eik-Nes SH, Grøttum P. Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate. Ultrasound Obstet Gynecol 1999; 14: 17–22"]
- "...the assumption that large differences between gestational age estimated by the last menstrual period and ultrasound are caused by unreliability in the last menstrual period estimate and not by pathology in the fetus 15."
- Abstract Conclusion (p. 41) Tunón et al. 1998
"Assessment of gestational age from the time of IVF, CRL and BPD in pregnancies conceived after IVF shows equally high agreement between the three methods. This supports the use of ultrasound as a reliable method for estimation of gestational age." - Discussion Section Conclusion (p. 45)
"In spite of the fact that IVF pregnancies are achieved through intervention, the high agreement between the gestational age calculated from the time of IVF and from the early CRL measurements in the same pregnancies, the high agreement between gestational age calculated from the time of IVF and BPD supports the use of ultrasound as a reliable method for estimation of day of delivery both in normally conceived pregnancies and IVF pregnancies."
Interestingly and ironically, Tunón et al. 2000 is the 2nd citation in Wikipedia's entry for Gestational age for IVF-based GA, the 3rd dot point in the "Methods" section as follows:"
- "In case of in vitro fertilization, calculating days since oocyte retrieval or co-incubation and adding 14 days.[2]" (Source: Wikipedia: Gestational age) Cited in Wikipedia as: "2 Tunon, K.; Eik-Nes, S. H.; Grøttum, P.; Von Düring, V.; Kahn, J. A. (2000). "Gestational age in pregnancies conceived after in vitro fertilization: A comparison between age assessed from oocyte retrieval, crown-rump length and biparietal diameter". Ultrasound in Obstetrics and Gynecology. 15 (1): 41–46. PMID 10776011. doi:10.1046/j.1469-0705.2000.00004.x."
- "Gestational age can also be estimated by calculating days from ovulation if it was estimated from related signs or ovulation tests, and adding 14 days by convention.[3]"
- "Tunón et al. were able to prove that ultrasound dating should be the method of choice even when LMP-data were reliable (Tunón et al. 1996), and in pregnancies conceived after in vitro fertilization (Tunón et al. 2000)." (Source: Økland 2012 NTNU dr.philos. Thesis, p. 22)
- "In Norway, this study [Tunón et al. 1996] supported the established policy of using the term according to ultrasound, ‘TUL’, independent of the LMP term date." (Source: ibid., p. 30)
Laila and her baby, and other women and their babies, endured increased medical risks, critical medical mistakes and grievous medical harms, which were silently and invisibly written off, unattributed, undocumented and unreported, as acceptable collateral damage of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation. Again, BPD is a problematic, unreliable predictor of GA & EDD independent of the prediction method (i.e. Campbell's Method of GA Estimation or Hutchon's Method of PDEE) during routine ultrasound exams, but this fact was (and remains) inconvenient to NCFM eSnurra Group's agenda of promoting the second-trimester ultrasound exams for NCFM eSnurra BPD-based EDD and, therefrom, a calculated GA using the equivalent of Naegele's rule, in reverse; and, replacing any first-trimester EDD & GA values with inherently less accurate second-trimester EDD & GA values for all pregnancies and abortions in Norway. Moreover, this internationally recognized BPD problem is inconvenient to NCFM eSnurra Group's prediction/estimation capabilities, i.e., NCFM eSnurra Group's model inventory does not include the more robust, 2-spacial dimensions HC measurement as a predictor/estimator of EDD. And, similar to used car dealers, NCFM eSnurra Group believes it must sell what is currently in inventory; and, BPD is the entire fetal head metric inventory of NCFM eSnurra Group's "method."
Multiple Studies: BPD Inferior to HC for Establishing GA & EDD
Setting the Standard: The Seminal Altman & Chitty 1997 Study
A seminal Altman & Chitty, 1997 study concluded BPD was problematic and unreliable due to its inability to deal with abnormal fetal head shapes and sizes as stated in the excerpts below.
- "As we have shown (Table 10), the most precise estimates of gestational age in our study are derived from the directly measured head circumference. Other measurements which gave almost as good predictions up to 30 weeks were the head area and the head circumference derived from two diameters." (Source: "New charts for ultrasound dating of pregnancy" D.G. Altman and L.S. Chitty. Ultrasound in Obstetrics & Gynecology 10 (1997) 174-191, p. 189)
- "As the prediction of gestational age is most accurate when based on the measurement of head circumference or head area, we believe that these measures should be used in preference to BPD for estimation of gestational age." (Source: ibid. p. 190)
A 1981 study established that "variations in the shape of the fetal skull...may adversely affect the accuracy of the biparletal diameter (BPD) measurement in estimating fetal age."
- "Several recent obstetrical sonographic examinations in this department demonstrated that variations in the shape of the fetal skull (e.g., dolichocephaly, brachycephaly) may adversely affect the accuracy of the biparietal diameter (BPD) measurement in estimating fetal age. In each case the cephalic index of the fetal skull (short axis/long axis x 100) was in either the dolichocephalic or brachycephalic range based on established postnatal criteria. Consequently, normal values were determined (mean, 78.3) for the cephalic index in utero based on 316 obstetrical sonographic studies performed at 14--40 weeks. Preliminary experience indicates that a cephalic index greater than 1 SD from the mean (less than 74, greater than 83) may be associated with a significant alteration in the BPD measurement expected for a given gestational age, and that the head circumference can be used effectively as an alternative means of establishing gestational age." (Source: "Estimating fetal age: effect of head shape on BPD." Hadlock FP, Deter RL, Carpenter RJ, Park SK. AJR Am J Roentgenol 1981; 137: 83-5.)
A 1988 study, found there were different BPD growth trajectories between males and females leading to the conclusion dating pregnancies by BPD can lead to error.
- "Summary. Growth of the fetal biparietal diameter (BPD) throughout the second and third trimesters was measured in a prospective longitudinal study. Linear-cubic equations were fitted to the data of individual fetuses and from these equations mean growth curves were produced for males and females. The head growth trajectories of males and females were significantly different. The study illustrates why the practice of dating pregnancies by ultrasonic fetal BPD measurement at about 16 weeks gestation can lead to error." (Source: "Sex difference in fetal head growth" W. M. O. MOORE, B. S. WARD, V. P. JONES, F. N. BAMFORD. BJOG Volume 95, Issue 3, March 1988 Pages 238–242 First published: March 1988. DOI: 10.1111/j.1471-0528.1988.tb06863.x)
A 1998 study to assess the accuracy of fetal biometry in mid-trimester of pregnancy in the assignment of fetal age found: "Head circumference was the best predictor of gestational age."
- "RESULTS Head circumference was the best predictor of gestational age (random error [SD] 3.77 days). Addition of abdominal circumference and femur length to head circumference improved the accuracy of the dating equation (random error 3.35 days). Most dating formulas had systematic errors of <1 week. The systematic error was -0.32 day for averaging the singleton-based predictions for twins and -1.26 days for triplets.
CONCLUSIONS Gestational age assessment with the use of fetal biometry from 14 to 22 weeks is accurate for singleton, twin, and triplet gestations." (Source: "How accurate is fetal biometry in the assessment of fetal age?" Chervenak FA, Skupski DW, Romero R, Myers MK, Smith-Levitin M, Rosenwaks Z, Thaler HT. Am J Obstet Gynecol. 1998 Apr;178(4):678-87.)
A 2004 study (below) states multiple problems in using BPD and recommends using head circumference (HC) as the "more robust method" for fetal age assessment.
- "We found that maternal age, multiparity, fetal gender, breech position, and shape of fetal head significantly affected GA assessment using BPD. However, when using HC, maternal age and fetal gender where the only factors affecting the estimation, and the impact of these two factors was less marked than for BPD." (Source: Fetal age assessment based on ultrasound head biometry and the effect of maternal and fetal factors., Johnsen SL1, Rasmussen S, Sollien R, Kiserud T., Acta, Obstet Gynecol Scand. 2004 Aug;83(8):716-23, p. 720)
- "The BPD chart presently used in the Norwegian population (10) was established in 1983 and was based on a longitudinal study of 90 fetuses, but statistical details are not available." (Source: ibid., p. 720)
- "Our study confirmed that the shape of the fetal head significantly affects age assessment in the second trimester, especially when using BPD (1.6 days for each SD of cephalic index from the mean)." (Source: ibid., p. 721)
- "A separate analysis including the observation of the excluded participant due to >14 days discrepancy between GA determined by LMP and by ultrasound measurement. We found no change in the regression curve. Comparison with the chart currently in use for the Norwegian population (10) showed that there was a difference of 8, 3 and 7 days for BPDs of 30, 40 and 60mm (corresponding to 13, 18 and 24 weeks of gestation, respectively). However, compared to a recent British chart (6) the difference was 1 day or less. Compared to the German BPD chart (9) the difference was 4 and 5 days at 18 and 24 weeks, respectively (30 and 40 mm)." (Source: ibid., p. 718)
- "RESULTS
BPD and HC were successfully measured in 642 participants. Using BPD and HC before 20 weeks, the new charts gave 3-8 days higher GA assessment than the charts presently in use, and <1 day difference compared to other recently established charts. Maternal age, multiparity, fetal gender, breech position and shape of fetal head affect GA estimation by 1-2 days when using BPD (p = 0.0001-0.02). Only maternal age and fetal gender affected GA estimation when using HC (</= 1 day, p = 0.001). (Source: ibid.)
CONCLUSIONS
Our new charts for assessing gestational age based on fetal head biometry are notably different from charts presently in use. Maternal and especially fetal factors affect gestational age assessment when using BPD, but less so for the HC method, which is suggested as the more robust method. (Source: ibid.)
A 2005 study concluded FL/HC is a more robust than FL/BPD for characterizing fetal proportions and that FL is an equally robust method as HC to assess fetal age.
- RESULTS
The new chart for age assessment by means of FL was based on 636 measurements. The 95% CI of the mean corresponded to <1 day. The variation between the mean and the 90th percentile was 5, 6, and 7 days at 13, 18, and 23 weeks, respectively, similar to the results when using BPD or HC. Maternal age modestly influenced gestational age assessment (1.3 days/10 years, P = 0.005), whereas smoking, height, body mass index, multiparity, fetal sex, cephalic index, and breech presentation had no impact. Reference charts for FL to head ratios have been presented. Maternal age, fetal sex, and cephalic index influenced the FL/BPD ratio, whereas only fetal sex influenced FL/HC. - "CONCLUSIONS
Fetal age assessment based on FL is an equally robust method as using HC. FL/HC is a more robust ratio to characterize fetal proportions than is FL/BPD." (Source: Fetal age assessment based on femur length at 10–25 weeks of gestation, and reference ranges for femur length to head circumference ratios, Synnøve Lian Johnsen, Svein Rasmussen, Rita Sollien, Torvid Kiserud, Acta Obstet Gynecol Scand. 2005 Aug;84(8):725-33.)
A 2006 study states that HC and BPD predicted spontaneous birth with a mean accuracy of one day, HC being better than BPD.
- RESULTS
For the entire group, the median differences between actual and predicted delivery with HC and BPD were 0.9 and 1.2 days, respectively. For deliveries with a spontaneous onset of labor (n=3336) the corresponding differences were 0.9 and 1.4 days. The difference between the HC and BPD methods was significant (P<0.0001). In the group of spontaneous onset of labor, there were 05.6% post-term pregnancies (>or=296 days) according to HC and 5.7% according to BPD.
CONCLUSION
Provided that the expected pregnancy duration was 282 days, both HC and BPD predicted spontaneous birth with a mean accuracy of one day, HC being significantly better than BPD. (Source: Accuracy of second trimester fetal head circumference and biparietal diameter for predicting the time of spontaneous birth. Johnsen SL1, Rasmussen S, Sollien R, Kiserud T., J Perinat Med. 2006;34(5):367-70.)
- "RESULTS
A total of 111 ultrasonographic biometries were performed between the 31(st) 38(th) week of gestation. Fetuses in the breech position had a significantly lower BPD compared to HC and FL. The difference between BPD and HC was 16.2 days (95%Cl 14.318.1; p = 0.001). Maternal age at delivery was 20-36 years (average 28.1; median 28.0)."
"CONCLUSIONS
According to our results, fetuses in the breech position have a significantly lower BPD compared to HC or FL. HC and FL parameters correlate with gestational age. In cases of ultrasonographic biometric discrepancy between BPD and FL, the fetal position should be taken into account. Breech presented fetuses have an elongated head shape and ultrasound biometrics should evaluate its circumference (HC). It is important to responsibly interpret the results so as not to stress the expecting mother with suspicions of fetal pathology." (Source: "DISCREPANCY IN ULTRASOUND BIOMETRIC PARAMETERS OF THE HEAD (HC – HEAD CIRCUMFERENCE, BPD – BIPARIETAL DIAMETER) IN BREECH PRESENTED FETUSES" M. Lubusky, M. Prochazka, M. Langova, K. Vomackova, L. Cizek; Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2007, 151(2):323–326.)
The following excerpt cites work from 2007 that showed HC outperformed BPD for dolichocephalic fetuses as "a good reason for contemplating using HC rather than BPD."
- "In a recent prospective study 2,3 we were able to show that for the 10% of fetuses that were most dolichocephalic, the biparietal diameter (BPD) method missed the day of spontaneous birth by −3.0 days (95% CI, −4.5 to −1.4) compared with the head circumference (HC) method’s 0.9 days (95% CI, −0.6to 2.4): a good reason for contemplating using HC rather than BPD." (Source: Correspondence, Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, Ultrasound Obstet Gynecol 2008; 31: 225–228) (Cited Sources: 2, Johnsen SL, Rasmussen S, Sollien R, Kiserud T. Accuracy of second trimester fetal head circumference and biparietal diameter for predicting the time of spontaneous birth. JPerinat Med 2006;34: 367–370. AND 3, Johnsen SL, Rasmussen S, Sollien R, Kiserud T. Reply. JPerinat Med 2007; 35: 352.)
In a 2008 Correspondence letter regarding the article: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection," presented evidence of "a good reason for contemplating using HC rather than BPD."
- In a recent prospective study 2,3 we were able to show that for the 10% of fetuses that were most dolichocephalic, the biparietal diameter (BPD) method missed the day of spontaneous birth by −3.0 days (95% CI, −4.5 to −1.4) compared with the head circumference (HC) method’s 0.9 days (95% CI, −0.6 to 2.4): a good reason for contemplating using HC rather than BPD. (Source: Correspondence: Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, T. Kiserud, S. L. Johnsen and S. Rasmussen, Ultrasound Obstet Gynecol 2008; 31: 225–228)
In 2010 the ISUOG Prenatal Ultrasound Screening Task Force published their Practice Guidelines for Performance of the Routine Mid-Trimester Fetal Ultrasound Scan which cautioned that BPD "can lead to misleading estimates of fetal age" and that "HC is more reliable."
- "Abnormalities in head shape (e.g. dolichocephaly and brachycephaly) can lead to misleading estimates of fetal age when the BPD is used under these circumstances, in which case the HC is more reliable (20)." (Source: ISUOG Practice Guidelines for Performance of the Routine Mid-Trimester Fetal Ultrasound Scan, ISUOG Prenatal Ultrasound Screening Task Force June 2010, p.7) (Citation: 20. Hadlock FP, Deter RL, Carpenter RJ, Park SK. Estimating fetal age: effect of head shape on BPD. AJR Am J Roentgenol 1981; 137: 83-5.)
In 2013 The American Institute of Ultrasound in Medicine (AIUM) published their AIUM Practice Parameter for the Performance of Obstetric Ultrasound Examinations in which they warned about the problems with BPD and explained HC is more robust (excerpts below). Also, AIUM made the argument that LMPD should be used to test the reasonableness of ultrasound-based GA and as evidence of potential fetal pathology when there are "Significant discrepancies between gestational (menstrual) age and fetal measurements" (first excerpt below). Apparently, AIUM advocates for the inclusion of LMPD/OTPD in the practice of evidence-based medicine, not Directorate of Health and NCFM eSnurra Group's protocol of obviating LMPD et al. at the 18wUSE in the practice of evidence-obviated medicine.
- "Significant discrepancies between gestational (menstrual) age and fetal measurements may suggest the possibility of a fetal growth abnormality, intrauterine growth restriction, or macrosomia. 34" p. 8
- "The head circumference is measured at the same level as the biparietal diameter, around the outer perimeter of the calvarium. This measurement is not affected by head shape." p.8
- "The head shape may be flattened (dolichocephaly) or rounded (brachycephaly) as a normal variant. Under these circumstances, certain variants of normal fetal head development may make measurement of the head circumference more reliable than biparietal diameter for estimating gestational (menstrual) age." p. 8 (Source: The American Institute of Ultrasound in Medicine (AIUM): AIUM Practice Parameter for the Performance of Obstetric Ultrasound Examinations, © 2013 by AIUM; Parameter developed in conjunction with the American College of Radiology (ACR), the American College of Obstetricians and Gynecologists (ACOG), and the Society of Radiologists in Ultrasound (SRU))
In February 2014 the Society of Obstetricians and Gynaecologists of Canada (SOGC) published their "Clinical Practice Guidelines: Determination of Gestational Age by Ultrasound. No. 303" in the Journal of Obstetric and Gynaecology Canada (JOGC) which stated the following.
- "The BPD is less reliable in determining gestational age when there are variations in skull shape, such as dolichocephaly or brachycephaly; hence some authors feel that BPD is less reliable than HC. 9, 53–57 As a single parameter, HC correlates better to gestational age than the other 3 standard parameters in the second trimester, and as with all others, it becomes less accurate with increasing gestational age.58–61" (Source: SOGC Clinical Practice Guidelines: Determination of Gestational Age by Ultrasound. No. 303, PRINCIPAL AUTHORS: Kimberly Butt, MD, Fredericton NB, Ken Lim, MD, Vancouver BC. JOGC February 2014, p. 176.)
- "It is prudent to evaluate the etiology of an aberrant measurement to determine its clinical significance." (Source: ibid., p. 176.)
- "Potential harms include the possible reassignment of dates when significant fetal pathology (such as fetal growth restriction or macrosomia) result in a discrepancy between ultrasound biometric and clinical gestational age. Such reassignment may lead to the omission of appropriate—or the performance of inappropriate—fetal interventions." (Source: ibid., p. 171.)
- "There is disagreement in the literature as to whether a significant discordance between menstrual and US estimates of gestational age is associated with an increased risk of obstetrical complications. 107–114" (Source: ibid., p. 177.) [Note: US = ultrasound]
- "Although there may be a risk in using US dating exclusively, some of this risk would remain whenever there is discordance between menstrual and US estimates, regardless of which method of gestational age assignment is used." (Source: ibid., p. 177.)
In 2016 The American College of Obstetrician and Gynecologists (ACOG) & American Institute of Ultrasound in Medicine issued a Practice Bulletin that explicitly stated: "the head circumference is the single most-predictive parameter of gestational age..."
- "Ultrasound dating in the second trimester typically is based on calculations that incorporate the biparietal diameter, head circumference, femur length, and abdominal circumference. Of the different measurements, the head circumference is the single most-predictive parameter of gestational age between 14-22 weeks of gestation, although combining various parameters improves the precision of gestational age over the use of head circumference measurement alone (16, 36)." (Source: The American College of Obstetrician and Gynecologists (ACOG) & American Institute of Ultrasound in Medicine (AIUM), Practice Bulletin, Clinical Management Guidelines for Obstetrician-Gynecologists, Number 175, December 2016. p. 7)
- DISCUSSION [Note: Citation/reference hypertext links added for convenience]
(...)
"Other studies (22, 23) have compared the EDD prediction bias for a population-based model estimating the remaining time of pregnancy (24) with charts based on carefully selected low-risk women with regular menstrual cycle (12, 25). These comparative studies found a clinically relevant gestational age dependent EDD prediction bias of more than four days for our dating charts. Unfortunately, the comparison was made based on biparietal diameter and FL measurements, neither of those representing the recommended method HC for second trimester dating (12). Such a systematically skewed bias (22, 23) could not be shown in the current study of second trimester HC dating. Furthermore the EDD predictions based on our charts (biparietal diameter, FL) were in those studies (22, 23) retrospectively applied on a population. The pregnant women had been assigned and informed about an EDD based on a different term prediction model. This approach ignores the complexity of the initiation of labor in human (26), far from well understood. Psychological stress during pregnancy is associated with preterm delivery and was estimated to account for 2 3 –27% of the variance in gestational age at birth (27). Several hormonal axes are thought to be involved in the initiation of parturition on one side (26), and on the other side are targets for psycho -neuro - immunological modulation during pregnancy (28) . Thus, maternal expectations of the given due date may affect the initiation of parturition." (Source: "Estimated date of delivery based on second trimester fetal head circumference; a population based validation of 21451 deliveries" Jörg Kessler, Synnøve Lian Johnsen, Cathrine Ebbing, Henriette Odland Karlsen, Svein Rasmussen & Torvid Kiserud. Acta Obstetrica et Gynecologica Scandinavica (AOGS), https://doi.org/10.1111/aogs.13454 First published: 31 August 2018, Publication history: Accepted manuscript online: 31 August 2018)
"Abstract
Introduction
Fetal biometry is used for determining gestational age and estimated day of delivery (EDD). However, the accuracy of the EDD depends on the assumed pregnancy length included in the calculation. This study aimed at assessing actual pregnancy length and accuracy of EDD prediction based on fetal head circumference measured at second trimester.
Material and methods
Population based observational study with inclusion criteria: singleton pregnancy, head circumference dating in the second trimester, spontaneous onset or induction of delivery ≥294 days of gestation, live birth. The EDD was set anticipating a pregnancy length of 282 days. Bias in the prediction of EDD was defined as the difference between the actual date of birth and EDD.
Results
Head circumference measurements were available for 21 451 pregnancies. Ultrasound‐dated pregnancies had a median pregnancy length of 283.03 days corresponding to a method bias of 1.03 days (95% CI; 0.89 to 1.16). This bias was dependent on head circumference at dating ranging from ‐1.58 days (95% CI; ‐3.54 to 1.12) to 3.42 days (95% CI; 1.98 to 4.31). The median pregnancy length based on the last menstrual period of women with regular menstrual cycle (n=12985) was 283.15 days (95% CI; 282.91 to 283.31). A total of 5685 (22.9%, 95%CI; 22.4 to 23.4%) and 886 (3.6%, 95% CI; 3.3 to 3.8%) were still pregnant 7 and 14 days after EDD, respectively.
Conclusions
Second trimester head circumference measurements can be safely used to predict EDD. A revision of the pregnancy length to 283 days will reduce the bias of EDD prediction to a level comparable with other methods."
(Source: "Estimated date of delivery based on second trimester fetal head circumference; a population based validation of 21451 deliveries" Jörg Kessler, Synnøve Lian Johnsen, Cathrine Ebbing, Henriette Odland Karlsen, Svein Rasmussen & Torvid Kiserud. Acta Obstetrica et Gynecologica Scandinavica (AOGS), https://doi.org/10.1111/aogs.13454 First published: 31 August 2018, Publication history: Accepted manuscript online: 31 August 2018)
A 2018 UpToDate literature review includes the following.
- "A single late [ultrasound] examination cannot reliably distinguish between a pregnancy that is misdated and younger than expected and a pregnancy that is complicated by fetal symmetric growth restriction."
- "In some cases, very early fetal growth restriction rather than inaccurate menstrual dating may be the reason for a discrepancy between an early ultrasound and menstrual dating (or dating based on conception using assisted reproductive technologies) [72], although this is uncommon [124-126]. When an EDD is revised because of smaller than expected size of the fetus on an ultrasound examination before 22 weeks, we suggest a follow-up ultrasound to evaluate fetal growth over time and make sure this finding was not due to early growth restriction."
- "Ultrasound estimates of gestational age are based on the assumption that size correlate with age. When there is a reason that a biometric parameter might not correlate with age, then that value is excluded from gestational age estimates. Various fetal body ratio indexes (eg, HC/AC, BPD/FL,FL/AC) have been established across preg nancy to define how these measurements correlate in an average fetus and to determine if a parameter is potentially abnormal. Measurements of additional biometric parameters may be useful when there are biometric discrepancies. (See 'Sonographic assessment of gestational age' above and 'Approach to discordant biometry markers' above.)" (Source: "Prenatal assessment of gestational age, date of delivery, and fetal weight" Andrew P MacKenzie, MDCourtney D Stephenson, DOEdmund F Funai, MD. Section Editor:Deborah Levine, MD; Deputy Editor:Vanessa A Barss, MD, FACOG. UpToDate. Literature review current through: Apr 2019. | This topic last updated: Jul 12, 2018. Topic 5391 Version 41.0)
The 2019 "ISUOG Practice Guidelines: ultrasound assessment of fetal biometry and growth" state the following with respect to accurate estimation of gestational age.
- "Accurate estimation of gestational age is a prerequisite for determining whether fetal size is appropriate-for-gestational age (AGA). Except for pregnancies arising from assisted reproductive technology, the date of conception cannot be determined precisely. Clinically, most pregnancies are dated by the last menstrual period, though this may sometimes be uncertain or unreliable. Therefore, dating pregnancies by early ultrasound examination at 8–14 weeks, based on measurement of the fetal crown–rump length (CRL), appears to be the most reliable method to establish gestational age. Once the CRL exceeds 84 mm, HC should be used for pregnancy dating 2–4. HC, with or without FL, can be used for estimation of gestational age from the mid-trimester if a first-trimester scan is not available and the menstrual history is unreliable. When the expected delivery date has been established by an accurate early scan, subsequent scans should not be used to recalculate the gestational age 1. Serial scans can be used to determine if interval growth has been normal." (Source: "ISUOG Practice Guidelines: ultrasound assessment of fetal biometry and growth" Salomon LJ, Alfirevic Z, da Silva Costa F, Deter RL, Figueras F, Ghi T, Glanc P, Khalil A, Lee W, Napolitano R, Papageorghiou AT, Sotiriadis A, Stirnemann J, Toi A, Yeo G. Ultrasound Obstet Gynecol 2019; 53: 715–723. URL: ttps://obgyn.onlinelibrary.wiley.com/doi/full/10.1002/uog.20272; PDF: https://www.isuog.org/uploads/assets/uploaded/74ebbe42-863b-4d8f-a6b0e06a416c5f2e.pdf)
Data Irregularities Not Explained
In 2015 NCFM eSnurra Group were asked to explain BPD data irregularities (excerpts below). Moreover, these identified data irregularities were known to Directorate of Health, but Directorate of Health decided to ignore them.
- "The Directorate of Health also ignores published criticism of the Trondheim study (4): selection bias before and after weeks 18 – 20 of gestation; unclear exclusion criteria for fetuses with potentially hampered growth; and failing to account for the inclusion of fetuses with an elongated head whose biparietal diameter was adjusted based on the longitudinal axis of the skull." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age", Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093) Reference (4): (Source: Re: A direct method for ultrasound prediction of day of delivery:a new, population-based approach. Problems of accounting for a retrospective selection. Kiserud T, Johnsen SL, Rasmussen S., Ultrasound Obstet Gynecol 2008; 31: 22)
- "The midwives trained at the center in Trondheim have been recommended to measure the fronto-occipital diameter in fetuses considered to be dolichocephalic, and to use this information in order to assign an expanded virtual BPD for the calculation of gestational age and day of confinement. We cannot see that the authors have given any account of these fetuses or how this procedure influenced the statistics." (Source: Correspondence, Re: A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Problems of accounting for a retrospective selection, Ultrasound Obstet Gynecol 2008; 31: 225–228:)
Model Sensitivity vs. Patient Sensitivity
At Laila's routine 18wUSE, i.e., after all her key pregnancy dates had been discarded by a government-mandated protocol of evidence-obviated medicine implemented in conjunction with NCFM eSnurra Group's "method" (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE), without Laila's prior, informed, voluntary, explicit consent, Laila's baby's BPD was measured to generate NCFM eSnurra BPD-based EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse. However, Laila's assigned NCFM eSnurra BPD-based EDD was grossly inaccurate and resulted in increased medical risks, critical medical mistakes and grievous medical harms; and, given the NCFM eSnurra BPD-based EDD assigned to Laila's pregnancy had been proven to be grossly inaccurate by Laila's combined, fully corroborating, factual LMPT/OTPD/SCID-based EDD by 14-days, there was bound to be a significant prediction error, and there was, a prediction error = (predicted (set to 0) - actual) = -24 days, more than 3 weeks, 3w+3, just 4 days shy of a full menstrual cycle/period, technically classified as a preterm by NCFM eSnurra Group's published criteria (see prediction errors bar-chart frequency distribution below).
- "However, the mean value has the well known drawback of being overly sensitive to outliers in the data, such as those caused by gross errors 25. The further away a measurement is from the center of the distribution, the larger its influence on the mean. As the length of gestation has a heavily left-skewed distribution, this makes inclusion and exclusion criteria for the reference data much more precarious; different criteria may lead to substantial differences in the mean value. Figure 7 shows how only a few percent of the data in the lower tail of the distribution may influence the mean value by up to 2 days. This is untenable in a situation where there may be disagreement about details of the data selection." (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," p. 24-25. H. K. GJESSING, P. GRØTTUM and S. H. EIKNES. Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 23. DOI: 10.1002/uog.4053)
- To paraphrase the bold text above: This is untenable in a situation were there may be disagreement about details of the data obviated from all medical evidence (i.e. factual, key pregnancy dates) and, consequently, obviated from any and all consideration in medical thinking, medical decision-making and medical actions.
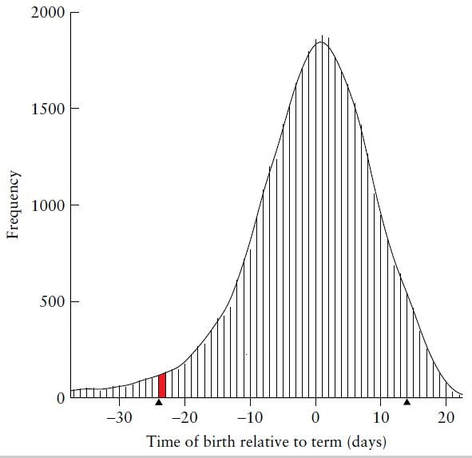
"Figure 3 Bar chart of residual frequencies for biparietal diameter in the range 25–60 mm. Residuals are computed as actual remaining time of pregnancy minus remaining time predicted with the local linear quantile regression model. Negative residuals indicate that the birth actually occurred before term; positive residuals denote birth after term. A curve of smoothed frequencies is superimposed on the bar charts to enhance readability. Bias, computed as the median of the residual distribution, is −0.09 days. 87.2% of the births fall within ±14 days of predicted delivery. 3.5% of births are classified as preterm (24 days or more before term, indicated by a black triangle) and 4.3% are classified as post-term (14 days or more after term, indicated by a black triangle). The residual distribution is based on 40 248 births. (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," p. 19, H. K. GJESSING, P. GRØTTUM and S. H. EIKNES. Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 23. DOI: 10.1002/uog.4053) [Note: the term "residual frequencies" = "prediction errors"; the term "gross errors" was used 3 times in Gjessing et al. 2007, but other than these 3 occurrences, the words "error" and "errors" were never used.]
Mere Statistics, not People: "outliers (gross errors) and/or pathologies"
Finally, NCFM eSnurra Group's Gjessing et al. 2007 (i.e., the paper which appropriated, plagiarized and enabled the misuse of the Hutchon Method of PDEE) discussed how "outliers (gross errors) and/or pathologies" do not affect the median as much as the mean of term predictions (excerpt below), indicating NCFM eSnurra Group is well aware of the inherent gross errors in NCFM eSnurra BPD-based EDD values assigned to pregnancies. However, NCFM eSnurra Group's Gjessing et al. 2007 does not discuss the unnecessary, preventable medical mistakes endured by some of these inherent "outliers (gross errors) and/or pathologies" i.e., (3.5% + 4.3% + 5%) = 12.8% of pregnant women and their babies, nor is there any discussion on how to screen for these inherent "outliers (gross errors) and/or pathologies" before they present as gross prediction errors; such as screening for "outliers (gross errors) and/or pathologies" by testing NCFM eSnurra BPD-based EDD values for reasonableness, errors or efficacy against Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD. Consequently, when NCFM eSnurra Group is more focused on protecting their models' sensitivities to "outliers (gross errors) and/or pathologies" than on their sensitivities regarding unnecessary increased medical risks, critical medical mistakes and grievous medical harms that present after the fact as inconvenient data points labeled as "outliers (gross errors) and/or pathologies," is, in itself a critical medical mistake; a mistake which induces a cascade of other critical medical mistakes proven to cause grievous medical harms to some of Norway's women and their fetuses/babies, Laila and her baby among them.
Finally, NCFM eSnurra Group's Gjessing et al. 2007 (i.e., the paper which appropriated, plagiarized and enabled the misuse of the Hutchon Method of PDEE) discussed how "outliers (gross errors) and/or pathologies" do not affect the median as much as the mean of term predictions (excerpt below), indicating NCFM eSnurra Group is well aware of the inherent gross errors in NCFM eSnurra BPD-based EDD values assigned to pregnancies. However, NCFM eSnurra Group's Gjessing et al. 2007 does not discuss the unnecessary, preventable medical mistakes endured by some of these inherent "outliers (gross errors) and/or pathologies" i.e., (3.5% + 4.3% + 5%) = 12.8% of pregnant women and their babies, nor is there any discussion on how to screen for these inherent "outliers (gross errors) and/or pathologies" before they present as gross prediction errors; such as screening for "outliers (gross errors) and/or pathologies" by testing NCFM eSnurra BPD-based EDD values for reasonableness, errors or efficacy against Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD. Consequently, when NCFM eSnurra Group is more focused on protecting their models' sensitivities to "outliers (gross errors) and/or pathologies" than on their sensitivities regarding unnecessary increased medical risks, critical medical mistakes and grievous medical harms that present after the fact as inconvenient data points labeled as "outliers (gross errors) and/or pathologies," is, in itself a critical medical mistake; a mistake which induces a cascade of other critical medical mistakes proven to cause grievous medical harms to some of Norway's women and their fetuses/babies, Laila and her baby among them.
- "The distribution of the duration of the pregnancy for the human fetus is highly skewed with a long left tail of preterm births, mainly caused by pathology. When evaluating a system that is designed to predict term in normal pregnancies, as these two methods are, one would prefer to exclude the pathological cases. However, because there are no good, independent measures of such pathology, the cases cannot easily be identified and excluded from the evaluation. One must consequently choose measures of performance that are reasonably insensitive to abnormal cases or outliers (gross errors in data). The mean is highly sensitive to observations in the tails of the distribution, and particularly so for skewed distributions. The pathological, early births will draw the ‘‘true’’ mean residual in a negative direction, yet their presence has no relevance for the predictive capacity of the method evaluated. Analyses we have done on a dataset of approximately 50,000 ultrasound scans from Trondheim, Norway, show that the leftmost 6% of the residual distribution account for a change in the mean of 2 days. In addition, residuals are also shifted in a negative direction by the inductions for post-term, which artificially shortens the duration of the pregnancy." (Source: LETTER TO THE EDITOR: Regarding ‘‘Term prediction with ultrasound: evaluation of a new dating curve for biparietal diameter’’ STURLA H. EIK-NES, PER GRØTTUM, HÅKON GJESSING. Acta Obstetricia et Gynecologica Scandinavica Volume 85, Issue 10, October 2006, Pages 1276–1278 First published: October 2006 DOI: 10.1080/00016340600839668)
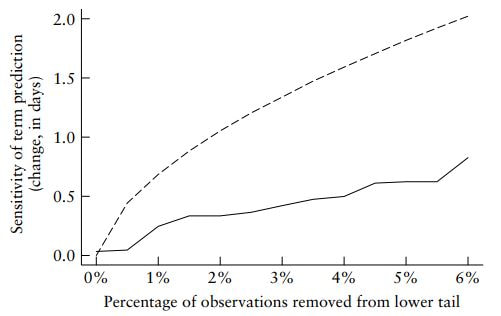
- "Figure 7 Approximate sensitivity of mean (dashed line) and median (solid line) term prediction when outliers (gross errors) and/or pathologies are removed from the lower (early) part of the birth distribution. The y-axis shows, as more observations are excluded, by how many days the corresponding term prediction will increase, relative to a prediction without exclusions. For example, excluding 4% of the data in the lower left tail increases the median by about 0.5 days, but the mean by more than 1.5 days." [Note: "observations removed from the lower tail" are the "outliers (gross errors) and/or pathologies" discussed above, which wold include Laila and her baby's -24 day NCFM eSnurra BPD-based EDD prediction error.] (Source: "A direct method for ultrasound prediction of day of delivery: a new, population-based approach," p. 19, H. K. GJESSING, P. GRØTTUM and S. H. EIKNES. Ultrasound Obstet Gynecol 2007; 30: 19–27, p. 26. DOI: 10.1002/uog.4053)
A Rough, Back-of-the-envelope Calculation
Question: How many pregnancies were at risk of critical mistakes due to grossly inaccurate NCFM Snurra/eSnurra BPD-based GA or EDD estimations used to assign GA & EDD to pregnancies in Norway within a government-mandated policy of evidence-obviated medicine with respect to obviating a woman's key pregnancy dates from medical evidence and from any and all consideration in medical thinking, medical decision-making and medical actions with respect to women's pregnancies, as happened to Laila and her baby, and other women and their babies, but not restricted to the same consequences as Laila's pregnancy? For convenience, let's define this to be the cumulative number of BPD-dated pregnancies at risk since "TUL" policy and label it: BPD@Risk.
Calculation Assumptions
Directorate of Health's knowledge-obviated, medially & ethically flawed, willfully reckless, grossly negligent 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine is the equivalent of a government-mandate for blindfolds and earmuffs to be worn by Norway's pregnant women (and their doctors and midwives) to cross the street. Mathematically, this sharply increases the opportunities to cause harms or adverse events, including lethal adverse events. This has been happening for 30 years, and this will continue to happen, unnecessarily. Moreover, the evidence of this is within multiple international studies published in international, academic medical journals; including Norwegian studies, such as the seminal Morken et al. 2014. Morken et al. 2014 used datasets unique to the Medical Birth Registry of Norway (MBRN) to conclude, for example:
The BPD Bottom Line
If head circumference (HC) had been included in NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) to predict/estimate EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse, instead of using the problematic, unreliable BPD, critical medical mistakes would have been prevented, and Laila and her baby would not have endured increased medical risks, critical medical mistakes and grievous medical harms, and the same would be true for other women and their fetuses/babies.
Alternatively
Since NCFM eSnurra does not include HC as an independent variable (i.e., predictor variable) in their model inventory, NCFM eSnurra Group's ultrasonographers could have been trained and/or instructed to take a full complement of fetal head metric measurements or just 1 more measurement, the robust HC measurement. And, since the HC measurement could have been looked up, easily, on the Internet from a source of proven efficacy, which would be in accordance with NCFM eSnurra Group's practice of making their method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) available to the public via NCFM eSnurra Group's website, iOS and Android apps. Another possibility is to secure fetal biometry reference charts from an ultrasound machine's advanced user manual (a searchable pdf file) which, not surprisingly, includes all the fetal biometry reference charts/tables included in the ultrasound machine's software. For example, the 12 reference charts/tables for HC identified below were found via a quick Google Search of the GE Voluson® E8 ultrasound machine; any one of these 12 charts/tables could be used to test BPD against HC for reasonableness, errors or efficacy i.e., provided the HC measurement had been made and recorded at the same time as the BPD measurement. The charts/tables for items 3 & 4 below are included as examples, emphasis added.
Question: How many pregnancies were at risk of critical mistakes due to grossly inaccurate NCFM Snurra/eSnurra BPD-based GA or EDD estimations used to assign GA & EDD to pregnancies in Norway within a government-mandated policy of evidence-obviated medicine with respect to obviating a woman's key pregnancy dates from medical evidence and from any and all consideration in medical thinking, medical decision-making and medical actions with respect to women's pregnancies, as happened to Laila and her baby, and other women and their babies, but not restricted to the same consequences as Laila's pregnancy? For convenience, let's define this to be the cumulative number of BPD-dated pregnancies at risk since "TUL" policy and label it: BPD@Risk.
Calculation Assumptions
- "TUL" or Term according to Ultralyd (utlrasoud) and only ultrasound policy & protocol has been in effect in Norway for 30 years, since 1987. ("...Eik-Nes et al. to introduce the phrase ‘TUL‘ — Term according to ULtrasound — which for 25 years has been a fixed Norwegian term..." (Source: Økland's 2012 NTNU dr.philos. Thesis)) [Note: 2012 - 25 years = 1987; 1987 through 2017 = 31 years]
- Over-the-counter, home-use ovulation tests were introduced to the mass market in 1989, 2-years after the "TUL" national medical policy & protocol of evidence-obviated medicine; the ovulation test adoption rate in Norway was not found/available; ergo, it is not included.
- Approximately 60,000 births in Norway/year "Of 58 100 births in 2016, there were 918 sets of twins and 4 sets of triplets, which corresponds to 15.9 multiple births per 1 000 births. This is the lowest share in 20 years. In 2016, the number of late foetal deaths was 183. This corresponds to 3.1 late foetal deaths per 1 000 births. This is an increase of 21 foetal deaths compared to 2015, but fewer than in 2014."(Source: https://www.ssb.no/en/fodte/)
- BPD measurements used to estimate GA and EDD via Campbell's method of GA Estimation and the Hutchon Method of Direct EDD Estimation (PDEE), respectively.
- 3.5% of BPD prediction errors "classified" as preterm, per NCFM eSnurra Group's Gjessing et al. 2007, Figure 7, "derived from a population-based registry with approximately 40 000 measurements." (p.22, 23)
- 4.3% of BPD prediction errors "classified" as post-term, per NCFM eSnurra Group's Gjessing et al. 2007, Figure 7 "derived from a population-based registry with approximately 40 000 measurements." (p.22, 23)
- 1,803,966 total births in Norway from 1987 through 2017 (31 years). (Source: Table 2, Single and multiple births, https://www.ssb.no/en/befolkning/statistikker/fodte)
- Equation: BPD@Risk = 1,803,966 total births x (0.035 preterm + 0.043 post-term) = 140,709 births
BPD@Risk = 140,709. Consequently since each pregnancy delivered at least 1 baby, the 140,400 must be doubled (conservatively, assume 1 child/pregnancy); ergo, the cumulative number of people at risk from BPD since 1987 has been 140,400 x 2 = 280, 800, of which 75% were women and baby girls.
20% of total people at risk = 56,160
10% of total people at risk = 28,800
5% of total people at risk = 14,400
1% of total people at risk = 2,808
- Equation: BPD@Risk = 1,803,966 total births x (0.035 preterm + 0.043 post-term) = 140,709 births
- Again, 280, 800 people at risk from BPD and the TUL policy since 1987; a rough approximation; reduce it by half and the message remains unchanged; reduce it by half again, same message.
Directorate of Health's knowledge-obviated, medially & ethically flawed, willfully reckless, grossly negligent 2014 Recommendation with their government-mandated protocol of evidence-obviated medicine is the equivalent of a government-mandate for blindfolds and earmuffs to be worn by Norway's pregnant women (and their doctors and midwives) to cross the street. Mathematically, this sharply increases the opportunities to cause harms or adverse events, including lethal adverse events. This has been happening for 30 years, and this will continue to happen, unnecessarily. Moreover, the evidence of this is within multiple international studies published in international, academic medical journals; including Norwegian studies, such as the seminal Morken et al. 2014. Morken et al. 2014 used datasets unique to the Medical Birth Registry of Norway (MBRN) to conclude, for example:
- "However, one of the most important clinical implications of our study is that these growth restricted infants should probably not have their gestational age determined solely by ultrasound."
- "This analysis of data from Norway, Sweden, Finland, and the United States demonstrates that both groups with discordant gestational age estimates had consistently higher risks of adverse perinatal outcomes than those classified as term by both methods. These results show that discrepancy between methods to estimate gestational age may be a predictor for infant mortality and other adverse pregnancy outcomes in all four study countries."
The BPD Bottom Line
If head circumference (HC) had been included in NCFM eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) to predict/estimate EDD and, therefrom, calculate GA, using the equivalent of Naegele's rule, in reverse, instead of using the problematic, unreliable BPD, critical medical mistakes would have been prevented, and Laila and her baby would not have endured increased medical risks, critical medical mistakes and grievous medical harms, and the same would be true for other women and their fetuses/babies.
Alternatively
Since NCFM eSnurra does not include HC as an independent variable (i.e., predictor variable) in their model inventory, NCFM eSnurra Group's ultrasonographers could have been trained and/or instructed to take a full complement of fetal head metric measurements or just 1 more measurement, the robust HC measurement. And, since the HC measurement could have been looked up, easily, on the Internet from a source of proven efficacy, which would be in accordance with NCFM eSnurra Group's practice of making their method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) available to the public via NCFM eSnurra Group's website, iOS and Android apps. Another possibility is to secure fetal biometry reference charts from an ultrasound machine's advanced user manual (a searchable pdf file) which, not surprisingly, includes all the fetal biometry reference charts/tables included in the ultrasound machine's software. For example, the 12 reference charts/tables for HC identified below were found via a quick Google Search of the GE Voluson® E8 ultrasound machine; any one of these 12 charts/tables could be used to test BPD against HC for reasonableness, errors or efficacy i.e., provided the HC measurement had been made and recorded at the same time as the BPD measurement. The charts/tables for items 3 & 4 below are included as examples, emphasis added.
- Head Circumference (HC) ASUM, 1-85
- Head Circumference (HC) CFEF, 1-86
- Head Circumference (HC) Chitty, 1-87 (included below as an example, only)
- Head Circumference (HC) Chitty(derived), 1-88 (included below an example, only)
- Head Circumference (HC) Hadlock_82, 1-89
- Head Circumference (HC) Hadlock_84, 1-90
- Head Circumference (HC) Hansmann, 1-91
- Head Circumference (HC) Jeanty, 1-92
- Head Circumference (HC) Johnsen, 1-93
- Head Circumference (HC) Kurmanavicius, 1-95
- Head Circumference (HC) Merz, 1-96
- Head Circumference (HC) Nicolaides, 1-97
|
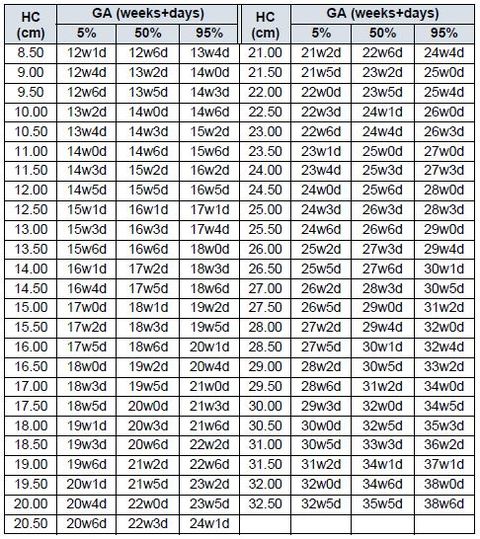
1-1-87 Head Circumference (HC) CHITTY Reference: Altman D.G.; Chitty L.S. “New charts for ultrasound dating of pregnancy.” Ultrasound in Obstetrics and Gynecology Vol. 10: 174-191, 1997 NOTE: HC measured (not derived from diameters) |
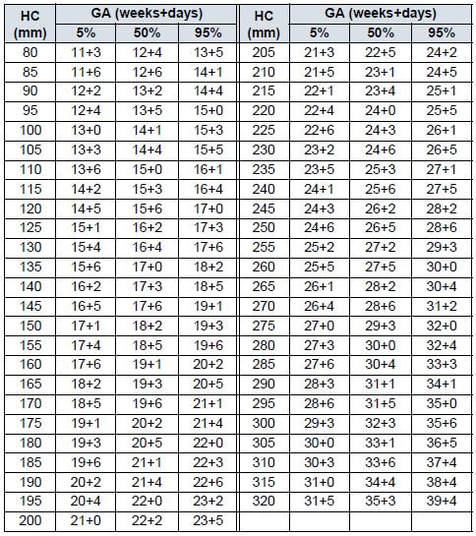
1-1-88 Head Circumference (HC) CHITTY (derived)
Reference: Altman D.G.; Chitty L.S. “New charts for ultrasound dating of pregnancy” Ultrasound in Obstetrics and Gynecology Vol. 10: 174-191, 1997 NOTE: HC derived from BPD/OFD Input Unit: mm Output Unit: weeks+/- days Min Range: 80 mm Max Range: 320 mm |
|
|
(Source: GE Medical Systems Kretz Ultrasound, VOLUSON® E8- ADVANCED REFERENCE MANUAL 1-87 DIRECTION KTD100278-100, REVISION 2, Operating Documentation 0123, Copyright© 2009 by GE Medical Systems - Kretztechnik) Note: GE Medical Systems acquired Kretztechnik AG in 2001.
The Altman & Chitty 1997 charts included above are both HC reference charts; however, the chart on the left is for "HC measured (not derived from diameters)" while the chart on the right is for "HC derived from BPD/OFD." The reason for the 2 HC charts is because there is a difference of 1-4 days, increasing with GA, with the "measured" lagging the "derived" which needed to be recognized. Also, Altman & Chitty believed HC "should be used in preference to BPD for estimation of gestational age." The excerpt below is literally the last words, the actual bottom line of Altman & Chitty 1997.
- "As the prediction of gestational age is most accurate when based on the measurement of head circumference or head area, we believe that these measures should be used in preference to BPD for estimation of gestational age." (Source: "New charts for ultrasound dating of pregnancy" D.G. Altman and L.S. Chitty. Ultrasound in Obstetrics & Gynecology 10 (1997) 174-191, p. 190)
- New Charts for ultrasound dating of pregnancy, 1997
D. G. Altman & L. S. Chitty - Charts of fetal size: 4. Femur length, 1994
Lyn S. Chitty, Douglas G. Altman, Annabel Henderson, Stuart Campbell - Charts of fetal size: 3. Abdominal measurements, 1994
Lyn S. Chitty, Douglas G. Altman, Annabel Henderson, Sruart Campbell - Charts of fetal size: 2. Head measurements, 1994
Lyn S. Chitty, Douglas G. Altman, Annabel Henderson, Stuart Campbell - Charts of fetal size: 1. Methodology, 1994
Douglas G. Altman, Lyn S. Chitty
- research design to ensure clinically relevant results
- study methodology
- principles of data analysis
- methods comparisons
- statistical modeling techniques
- sample selection criteria
- inclusion & exclusion criteria with associated consequences
- disciplined comparison of results among other publications
- "The relationship between BPD and cephalic index suggests that we might get a better estimate of fetal age by using a measurement that was not affected by head shape. Put another way, we ought to consider OFD as well, either explicitly (as in derived head circumference and head area) or implicitly (as for measured head circumference). The correlation coefficients between these three measures and the cephalic index were all below 0.08, showing that they are essentially independent of head shape." (Source: "New charts for ultrasound dating of pregnancy" D.G. Altman and L.S. Chitty. Ultrasound in Obstetrics & Gynecology 10 (1997) 174-191, p. 182)
- "It can be seen that the directly measured head circumference offers the tightest prediction intervals up to 18 weeks, with estimated gestational age likely to be within +/- 7 days (in 90% of cases). All the other measurements had uncertainty of arround +/- 8 days. Head circumference (either directly measured or derived) and head area gave predicted gestational ages that were mostly within about +/- 10 days in the period 18-24 weeks and about +/- 14 days at 24-30 weeks. Predictions based on the BPD were good up to about 18 weeks of gestation, but at later gestations were noticeably worse than those based on head circumference and head area. This effect is likey to reflect the relationship between BPD and head shape [Figure 9]. Head circumference and head area were much less storngly related to head shape. Note that 95% prediction intervals are 20% wider than the 90% ranges shown in Table 10." (Source: ibid. p. 185)
- "When ultrasound is used to date pregnancy, the date should be determined at the time of the firsts scan with acceptable measurements. That date should then be used throughout pregnancy, and should not be adjusted on the basis of subsequent ultrasound measurements." (Source: ibid. p. 188)
- "A particular problem concerns measurement of the fetal head. The most commonly used measurement is the BPD, but this single dimension does not adequately capture information about the size of the fetal head. Hadlock and colleagues 14 noted that dating pregnancies using the BPD would be misleading for fetuses with an atypical cephalic index. They did not take this effect into account, however, when they produced their formula for predicting gestational age from BPD 15. As we have shown, fetuses in the breech position are on average 2 days older than cephalic fetuses with the same BPD (Table 9). This difference is likely to relate to the difference in head shape, with fetuses in the breech position rending to be dolichocephalic, i.e., with a smaller cephalic index. This effect of fetal position is likely to be one reason why the estimation of gestational age using BPD is less accurate than dating based on head circumference or head area (Table 10)." (Source: ibid. p. 189)
- "As we have shown (Table 10), the most precise estimates of gestational age in our study are derived from the directly measured head circumference. Other measurements which gave almost as good predictions up to 30 weeks were the head area and the head circumference derived from two diameters." (Source: ibid. p. 189)
- "As the prediction of gestational age is most accurate when based on the measurement of head circumference or head area, we believe that these measures should be used in preference to BPD for estimation of gestational age." (Source: ibid. p. 190)
- "Doug Altman, Director, Centre for Statistics in Medicine, Oxford, UK opens the first EQUATOR symposium and talks about "Improving the quality and value of research publications -- how can we speed up progress?(Source: EQUATORNetwork, Published on Jan 7, 2013, https://www.youtube.com/watch?v=jJBjN8sYots)
NCFM eSnurra Group: Growth Method Description
Included below is a section entitled "BPD and FL versus HC" from the NCFM eSnurra Group publication "eSnurra Growth - Method Description," an 8-page pamphlet which appears to be a marketing pamphlet to increase awareness and purchase of the the eSnurra circular slide rule or pregnancy wheel to which Growth/weight prediction/estimation at delivery has been added to CRL, BPD, FL & MAD predictions/estimations of EDD. Moreover, this publication would appear to be based on the results of NCFM eSnurra Groups Gjessing et al. 2017 (above) entitled: "Fetal size monitoring and birth-weight prediction: a new population-based approach" which is the most current NCFM eSnurra Group publication to appropriate, plagiarize and misuse the Hutchon Method of Population-based Direct EDD Estimation. However, while the pamphlet cites and references 11 NCFM eSnurra Group publications, it does not reference Gjessing et al. 2017, indicating it was likely published before Gjessing et al. 2017. The date for this pamphlet is not know, as there is no identifiable calendar date within the 8-page pamphlet . However, the NCFM eSnurra Group website states:
- "Håkon K. Gjessing, Per Grøttum, Inger Økland, J. Morten Dreier and Sturla H. Eik-Nes are the authors of the booklet on the growth calculation method in eSnurra. The booklet is available as PDF , interactive iBook for iPad and soon also as ePub eBook for other eReader platforms." ("Håkon K. Gjessing, Per Grøttum, Inger Økland, J. Morten Dreier og Sturla H. Eik-Nes er forfatterene av hefte om vekstberegningsmetoden i eSnurra. Heftet er tilgjengelig som PDF, interaktiv iBook for iPad og snart også som ePub eBok for andre lesebrett-plattformer.") (Source: NCFM eSnurra Group's website: http://www.esnurra.no/publikasjoner/esnurra-vekst-metodebeskrivelse/)
- Pregnancy Calendar eSnurra
Pregnancy Calendar Snurra has become even better! Based on data from 40,000 pregnancies, this wheel answers when a pregnant woman can expect her term.
eSnurra is an updated version of Snurra, which was the nationwide standard for 20 years. The method, developed jointly by the National Center for Fetal Medicine, the Norwegian Institute of Public Health and the University of Oslo, is used in much of the country. eSnurra was launched in 2007.
eSnurra calculates the term date directly from the fetus size based on statistics. You can also enter additional parameters. - Graviditetskalenderen eSnurra
Graviditetskalenderen Snurra er blitt enda bedre! Basert på data fra 40.000 svangerskap gir dette hjulet deg svar på når den gravide kan vente at hun har termin.
eSnurra er en oppdatert versjon av Snurra, som var den landsdekkende standarden i 20 år. Metoden, som er utviklet i fellesskap av Nasjonalt senter for fostermedisin, Folkehelseinstituttet og Universitetet i Oslo, brukes i store deler av landet. eSnurra ble lansert i 2007.
eSnurra beregner termindatoen direkte fra fosterets størrelse basert på statistikk. Du kan også legge inn flere andre parametre.
NCFM eSnurra Group's 'Spin' (snurre) on HC vs. BPD
Compare NCFM eSnurra Group's spin (snurre) on HC reliability and accuracy relative to BPD with the data-driven analyses, evidence-supported findings, discussions and conclusions regarding HC reliability and accuracy in Altman & Chitty 1997 directly above. Also, compare the story NCFM eSnurra Group spin (snurre) about HC relative to BPD with all the study results presented earlier in this section. NCFM eSnurra Group are selling the problematic, unreliable BPD because BPD is the only fetal head metric they have in their data and model inventories; just as a used car dealer can only sell what is on the lot, in inventory, so it is for NCFM eSnurra Group and BPD.
BPD and FL versus HC
"BPD is a proven and robust parameter, introduced internationally in 1964 and well established in Norwegian practice. In case of deviating head shape, FL may be used instead of BPD. Predictions based on the FL measurement have precision close to BPD [8], and FL is therefore a good replacement for BPD, for example, dolichocephalic fetuses. As explained later, the FL measurement can also replace BPD in use for growth follow-up.
"Head circumference" (HC) is not the actual head circumference, but is calculated by the operator placing an ellipse over the head contour. The ellipse is determined by longitudinal and transverse axes. In practice, these axes will correspond to OFD and BPD. Then the formula used is
HC = π x (BPD + OFD)/2 (1)
for calculation [10]. HC is thus calculated as an average of BPD and OFD (multiplied by π).
This calculation method results in the following problems with the HC measurement :
- The head shape is of course not really elliptical. Therefore, the circumference of the ellipse will not match the actual head circumference. (Interestingly, the formula (1) is not the correct formula for the perimeter of an ellipse, just one approximation. The approximation is worse, the flatter the skull is).
- OFD is measured in a lateral direction and will therefore have greater uncertainty than BPD [11]. It is therefore not apparent the HC measurement when calculated as an average of BPD and OFD will have better precision than BPD alone. There is also no evidence that this would be the case [12]. The measurement in two axes also makes HC more difficult to standardize than BPD.
- It is clear that the HC measurement will also be affected if the skull is flattened. The assumption that HC will not be affected presupposes that the OFD expands as much as BPD decreases. This is unlikely since the skull will also expand in the height direction.
References cited in NCFM eSnurra Group's "BPD and FL versus HC" include:
- [1] Eik-Nes SH, Grøttum P, Persson P, Marsal K. Prediction of fetal growth deviation by ultrasonic biometry: I. Methodology. Acta Obstetricia et Gynecologica Scandinavica. 1982;61(1):53–58.
- [8] Gjessing HK, Grøttum P, Eik-Nes SH. A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Ultrasound in Obstetrics and Gynecology. 2007 Jul;30(1):19–27.
- [10] Loughna P, Chitty L, Evans T, Chudleigh T. Fetal size and dating: charts recommended for clinical obstetric practice. Ultrasound. 2009;17(3):160–166.
- Reference Source/Type Reference numbers total references
NCFM eSnurra Group: 1-9, 11-12 11 (58%)
R Statistical Environment: 13-15 3 (16%)
WHO Child Growth Standards: 17-18 2 (10.5%)
Fetal weight estimation: 18-19 2 (10.5%)
HC formula using BPD & OFD: 10 1 (5%)
Total: 19 (100%)
- "In view of the inaccuracies that may result from using the BPD measurement, the BMUS Fetal Measurements Working Party was of the opinion that the BPD should not be used in routine clinical practice for the estimation of gestational age or the appropriateness of fetal size in later pregnancy. Charts and tables for BPD measurements are therefore not presented in this document." (Source: ULTRASOUND, August 2009, Volume 17, Number 3, "Fetal size and dating: charts recommended for clinical obstetric practice" Pam Loughna1 , Lyn Chitty2 , Tony Evans3 & Trish Chudleigh4, 1 Academic Division of Obstetrics and Gynaecology, Nottingham University Hospitals NHS Trust, 2 Genetics and Fetal Medicine, Institute of Child Health and University College London Hospitals NHS foundation Trust, London, 3 Medical Physics, University of Leeds, Leeds and 4 The Rosie Hospital, Cambridge, UK)
- "BMUS accepted the need to review the old guidance, in order to ensure that the statistical validity of the original recommendations remained intact. That review, performed by Dr Lynn Chitty, Dr Trish Chudleigh and Dr Tony Evans, did bring some changes to recommendations, most particularly that dating after 13 weeks be based on head circumference measurement rather than bi-parietal diameter. The revised guidance was published in February 2007, and was widely welcomed." (Source: "The British Medical Ultrasound Society (BMUS), Policies, Statements & Guidelines: Fetal Measurements, https://www.bmus.org/policies-statements-guidelines/fetal-measurements/)
- "The authors prove only that their own BPD-based prediction has a larger overall bias than their HC prediction. This only has relevance for the authors’ own prediction models, not as an assessment of the prediction quality of HC versus BPD in general." (Source: Letters to the editor: "Accuracy of second trimester fetal head circumference and biparietal diameter for predicting the time of spontaneous birth" Håkon K. Gjessing and Per Grøttum. J. Perinat. Med. 35 (2007) 350–351 Received February 14, 2007. Accepted May 10, 2007. Published online on June 1, 2007. DOI: https://doi.org/10.1515/JPM.2007.080)
- "In summary, we cannot see that the authors have provided evidence that HC measurements give more precise predictions than do BPD measurements. Thus, the deduction that the well-tested BPD should be replaced by HC for term prediction cannot be made from this study." (Source: ibid.)
Cephalic Index Estimate: LMPD/OTPD/SCID-based GA vs. NCFM eSnurra BPD-based GA
Laila & Edward knew for a fact NCMF eSnurra BPD-based EDD & GA were grossly inaccurate; consequently, they decided to compare the cephalic index from Laila's LMPD/OTPD/SCID-based GA with the NCFM eSnurra BPD-based GA on the date of the 18wUSE. Cephalic index (CI) = (BPD/OFD x 100) or (i.e., (ear-to-ear diameter)/(back-to-front diameter) x 100); a CI < 75 is dolichocephaly (i.e., more commonly "long head" or "breech head").
Laila & Edward knew for a fact NCMF eSnurra BPD-based EDD & GA were grossly inaccurate; consequently, they decided to compare the cephalic index from Laila's LMPD/OTPD/SCID-based GA with the NCFM eSnurra BPD-based GA on the date of the 18wUSE. Cephalic index (CI) = (BPD/OFD x 100) or (i.e., (ear-to-ear diameter)/(back-to-front diameter) x 100); a CI < 75 is dolichocephaly (i.e., more commonly "long head" or "breech head").
- "CI refers to the ratio of the BPD and the occipitofrontal diameter (OFD) multiplied by 100 [25]. The standard CI range for normal-shaped craniums approximates one standard deviation from the mean (>74 or <83) [72]. Therefore, if the CI measurement approaches the outer limits of the normal range, the use of the BPD for estimation of gestational age is not accurate [72,73]. In these cases, HC (discussed below) is recommended for cranial assessment because it provides a good estimate of gestational age despite the fetus' irregular cranial structure [72]." (Source: "Prenatal assessment of gestational age and estimated date of delivery" Andrew P MacKenzie, MD, Courtney D Stephenson, DO, Edmund F Funai, MD, Deborah Levine, MD, Vanessa A Barss, MD, FACOG. UpToDate: Literature review current through: Sep 2017. | This topic last updated: Jun 26, 2017. https://www.uptodate.com/contents/prenatal-assessment-of-gestational-age-and-estimated-date-of-delivery)
- HC = π x (BPD + OFD)/2 or HC = 1.57 x (BPD + OFD)
CI = BPD/OCD x 100
Look up GA in 50th centile column of HC table in Johnsen et al. 2004, get HC
Plug HC into HC equation above
Plug BPD = 41 mm into HC equation above
Solve HC equation for: OFD = HC/1.57 - BPD
Plug OFD into CI equation above
Plug BPD = 41 mm into CI equation above
Solve CI equation for: CI = BPD/OFD x 100 - Results:
Laila's LMPD/OTPD/SCID-based GA = 19w+4, HC = 168 mm, BPD = 41 mm; CI = 62; extreme dolichocephaly
NCFM eSnurra BPD-based GA = 17w+6, HC = 146 mm, BPD = 41 mm; CI = 79; normal, not dolichocephaly (erroneous)
Tabel V. Gestational age assessed by head circumference (HC) from Johnsen et al. 2004
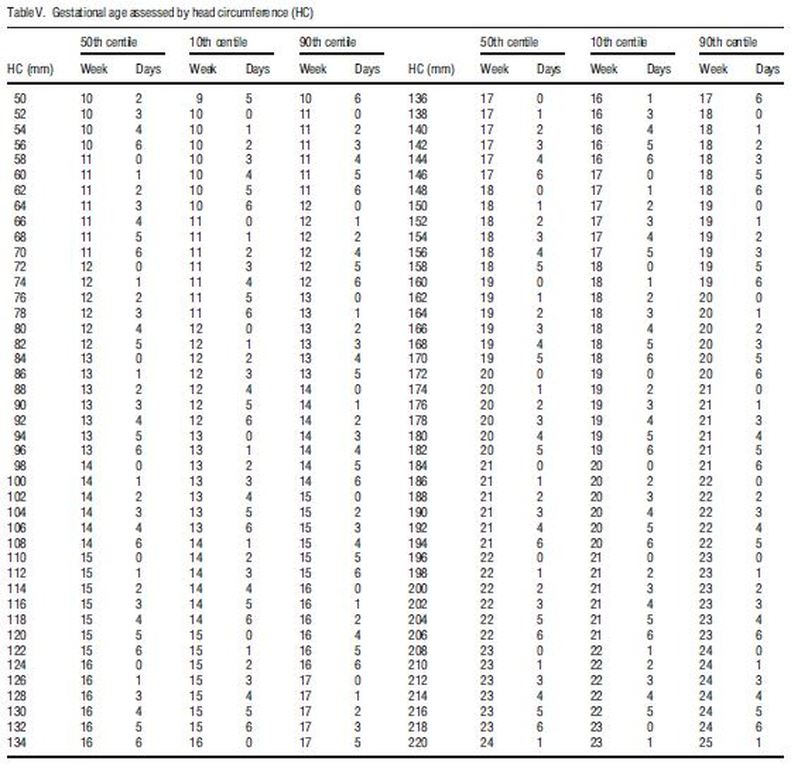
(Source: "Fetal age assessment based on ultrasound head biometry and the effect of maternal and fetal factors" Johnsen SL, Rasmussen S, Sollien R, Kiserud T., Acta, Obstet Gynecol Scand. 2004 Aug;83(8):716-23, p. 721)
Consider Laila's baby's reasonably estimated Cephalic Index = 62 = extreme dolichocephaly in the context of what NCFM eSnurra Group's Tunon et al. 2000 stated about fetal pathology in this context.
Bergen Group Recognized For Methodological Excellence
TheBergen Group's Terminhjulet or Term wheel is based on 2 prospective cross-sectional studies, Johnsen et al. 2004 & Johnsen et al 2005. However, there is a third, separate study, Johnsen et al. 2006, a prospective longitudinal study of growth of fetal biometric measurements which embeds Johnsen et al. 2004 & Johnsen et al 2005. This third study, Johnsen et al. 2006, with its 2 embedded studies was thoroughly examined and recognized for methodological excellence in all categories among 83 study publications from 32 countries. The resulting publication from this systematic review of methodology was featured in: "Systematic review of methodology used in ultrasound studies aimed at creating charts of fetal size" C Ioannou, K Talbot, E Ohuma, I Sarris, J Villar, A Conde-Agudelo, AT Papageorghioua. BJOG: An International Journal of Obstetrics & Gynaecology Volume 119, Issue 12. Version of Record online: 13 AUG 2012.
Methodological Excellence is Similar to Music (i.e., good music)
When it was learned the BJOG "Systematic Review of Methodology..." article had identified Bergen Group for excellence in all methodology categories, it begged the obvious question: Were Bergen Group Led Zeppelin fans? Okay, sure, Bergen Group are likely Bach: Concerto for 4 Harpsichords in A minor fans, but Bergen Group are most decidedly Altman & Chitty et al. and Royston & Wright fans. Included above are key references cited by Bergen Group which make it clear Bergen Group were/are true fans and, themselves, recognized as next-level masters of of the music that is methodological excellence; excellence enabled from the privilege of standing on the shoulders of Altman & Chitty et al. and Royston & Wright, and others, all for the every-day-low-price of full, proper attribution. Consequently, Bergen Group's methodology is music; and, to get the most from this music metaphor, Bergen Group released their double-album, Johnsen et al. Live at Bergen (2004-2006), with sides 1 & 2 featuring "Fetal Head Biometry" and "Femur Length with Ratios," respectively, back to back on disc 1 and, sides 3 & 4 featuring "Fetal Metrics' Growth" and "Fetal Weight," respectively, back to back on disc 2, as numbered above, in manual sequence, of course; after all, Johnsen et al. Live at Bergen is a classic (available on vinyl). Bergen Group published a booklet (link below) which consolidates the techniques and methods of Johnsen et al. Live at Bergen, the liner notes, if you will.
- "This supports the assumption that large differences between gestational age estimated by the last menstrual period and ultrasound are caused by unreliability in the last menstrual period estimate and not by pathology in the fetus 15." (Source: "Gestational age in pregnancies conceived after in vitro ertilization: a comparison between age assessed from oocyteretrieval, crown-rump length and biparietal diameter" K. TUNON, S.H. EIK-NES, P. GRØTTUM, V. VON DU¨RING and J.A. KAHN. Ultrasound Obstet Gynecol 2000; 15: 41–46,. p 44)
- "However, at 18 weeks an early growth restriction that results in changing the estimated day of delivery to a date 2-3 weeks later in accordance with the ultrasound estimate means that the BPD is at least 6 mm smaller than it should be, i.e. the width of the BPD is already 14% less than expected for the age. This indicates an extensive restriction that is probably outside the physiological range, and cannot be considered compatible with continuous normal development. Such a severe and highly pathological growth restriction will be most likely to continue and make itself manifest later in pregnancy even if it is (mistakenly) corrected for at 18 weeks." (Source: "Fetal outcome when the ultrasound estimate of the day of delivery is more than 14 days later than the last menstrual period estimate" K. Tunon, S. H. Eik-Nes and P. Grattum, Ultrasound Obstet Gynecol 1999;14:17-22, p. 21)
Bergen Group Recognized For Methodological Excellence
TheBergen Group's Terminhjulet or Term wheel is based on 2 prospective cross-sectional studies, Johnsen et al. 2004 & Johnsen et al 2005. However, there is a third, separate study, Johnsen et al. 2006, a prospective longitudinal study of growth of fetal biometric measurements which embeds Johnsen et al. 2004 & Johnsen et al 2005. This third study, Johnsen et al. 2006, with its 2 embedded studies was thoroughly examined and recognized for methodological excellence in all categories among 83 study publications from 32 countries. The resulting publication from this systematic review of methodology was featured in: "Systematic review of methodology used in ultrasound studies aimed at creating charts of fetal size" C Ioannou, K Talbot, E Ohuma, I Sarris, J Villar, A Conde-Agudelo, AT Papageorghioua. BJOG: An International Journal of Obstetrics & Gynaecology Volume 119, Issue 12. Version of Record online: 13 AUG 2012.
- Johnsen et al. 2004: Fetal age assessment based on ultrasound head biometry and the effect of maternal and fetal factors. Johnsen SL1, Rasmussen S, Sollien R, Kiserud T., Acta, Obstet Gynecol Scand. 2004 Aug;83(8):716-23.
"The principles of data analysis described by Altman and Chitty (15) and Royston and Wright (16) were applied."
15. Altman DG, Chitty LS. Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994; 101: 29–34.
16. Royston P, Wright EM. How to construct ‘normal ranges’ for fetal variables. Ultrasound Obstet Gynecol 1998; 11: 30–8.
17. Bland JM, Altman DG. Measurement error. Br Med J 1996; 312: 1654.
6. Altman DG, Chitty LS. New charts for ultrasound dating of pregnancy. Ultrasound Obstet Gynecol 1997; 10: 174–91. - Johnsen et al 2005: Fetal age assessment based on femur length at 10–25 weeks of gestation, and reference ranges for femur length to head circumference ratios, Synnøve Lian Johnsen, Svein Rasmussen, Rita Sollien, Torvid Kiserud, Acta Obstet Gynecol Scand. 2005 Aug;84(8):725-33.
"The principles of data analysis described by Altman and Chitty (23) and Royston and Wright (24) were applied."
2. Altman DG, Chitty LS. New charts for ultrasound dating of pregnancy. Ultrasound Obstet Gynecol 1997; 10: 174–91.
23. Altman DG, Chitty LS. Charts of fetal size: 1. Methodology. Br J Obstet Gynaecol 1994; 01: 9–34.
24. Royston P, Wright EM. How to construct ‘normal ranges’ for fetal variables. Ultrasound Obstet Gynecol 1998; 11: 30–8.
25. Bland JM, Altman DG. Measurement error. BMJ 1996; 312: 1654. - Johnsen et al. 2006: Longitudinal reference charts for growth of the fetal head, abdomen and femur. Synnøve Lian Johnsen, Tom Wilsgaard, Svein Rasmussen, Rita Sollien, Torvid Kiserud. European Journal of Obstetrics & Gynecology and Reproductive Biology August 2006 Volume 127, Issue 2, Pages 172–185
"Altman and Chitty emphasizes that the appropriate study design and analysis are different for these three purposes [4]."
[4] Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet Gynecol 1993;3(6):378–84.
[5] Royston P, Altman DG. Design and analysis of longitudinal studies of fetal size. Ultrasound Obstet Gynecol 1995;6(5):307–12.
[25] Bland JM, Altman DG. Measurement error. Br Med J 1996;313 (7059):744.
[26] Royston P, Wright EM. Calculation of unconditional and conditional reference intervals from longitudinal measurements. Stat Med 1995;14:1417–36.
[27] ChittyLS,AltmanDG,HendersonA,Campbell S.Charts of fetal size. 3. Abdominal measurements. Br J Obstet Gyneacol 1994;101(2):125–31.
[28] Chitty LS, Altman DG, Henderson A, Campbell S. Charts of fetal size.2. Head measurements. Br J Obstet Gynaecol 1994;101(1):35–43.
[26] Royston P, Wright EM. Calculation of unconditional and conditional reference intervals from longitudinal measurements. Stat Med 1995;14:1417–36. - Johnsen et al. 2006b: Longitudinal reference ranges for estimated fetal weight. Synnøve Lian Johnsen, Svein Rasmussen, Tom Wilsgaard, Rita Sollien & Torvid Kiserud. Acta Obstetricia et Gynecologica Scandinavica Volume 85, 2006 - Issue 3 Pages 286-297 | Received 30 Aug 2004, Published online: 03 Aug 2009.
[5] Royston P, Altman DG. Design and analysis of longitudinal studies of fetal size. Ultrasound Obstet Gynecol 1995; 6: 307–12
[6] Altman DG, Chitty LS. Design and analysis of studies to derive charts of fetal size. Ultrasound Obstet Gynecol 1993; 3: 378–84
[20] Royston P, Wright EM. Calculation of unconditional and conditional reference intervals for foetal size and groowth from longitudinal measurements. Stat Med 1995; 14: 1417–36
Methodological Excellence is Similar to Music (i.e., good music)
When it was learned the BJOG "Systematic Review of Methodology..." article had identified Bergen Group for excellence in all methodology categories, it begged the obvious question: Were Bergen Group Led Zeppelin fans? Okay, sure, Bergen Group are likely Bach: Concerto for 4 Harpsichords in A minor fans, but Bergen Group are most decidedly Altman & Chitty et al. and Royston & Wright fans. Included above are key references cited by Bergen Group which make it clear Bergen Group were/are true fans and, themselves, recognized as next-level masters of of the music that is methodological excellence; excellence enabled from the privilege of standing on the shoulders of Altman & Chitty et al. and Royston & Wright, and others, all for the every-day-low-price of full, proper attribution. Consequently, Bergen Group's methodology is music; and, to get the most from this music metaphor, Bergen Group released their double-album, Johnsen et al. Live at Bergen (2004-2006), with sides 1 & 2 featuring "Fetal Head Biometry" and "Femur Length with Ratios," respectively, back to back on disc 1 and, sides 3 & 4 featuring "Fetal Metrics' Growth" and "Fetal Weight," respectively, back to back on disc 2, as numbered above, in manual sequence, of course; after all, Johnsen et al. Live at Bergen is a classic (available on vinyl). Bergen Group published a booklet (link below) which consolidates the techniques and methods of Johnsen et al. Live at Bergen, the liner notes, if you will.
- "Fosterbiometri: Fosteralder, størrelse og vekst - Referanseverdier for ultralydmålinger" : "Fetal Biometry: Fetal age, size and growth - Reference values for ultrasound measurements"
"INNLEDNING Ultralydmålinger av fosterets størrelse kan brukes til å beregne fosterets alder, fastsette termin og vurdere fosterets vekst og utvikling. For at ultralyd skal være et meningsfylt og nyttig verktøy i obstetrikken er det viktig at man bruker standardisert undersøkelsesteknikk og referansematerialer som er utarbeidet for det formål og den populasjonen de anvendes på. I dette heftet beskrives måleteknikker og metoder som kan brukes til vurdering av fosteralder og vekst, samt nye referansetabeller og vekstkurver utarbeidet for norsk populasjon."
"INTRODUCTION Ultrasound measurements of the fetus size can be used to calculate the age of the fetus, determine the term and assess the growth and development of the fetus. In order for ultrasound to be a meaningful and useful tool in obstetrics, it is important to use standardized research techniques and reference materials prepared for the purpose and the population to which they are applied. This booklet describes measurement techniques and methods that can be used to assess fetal age and growth, as well as new reference tables and growth curves prepared for the Norwegian population." (Source: "Fosterbiometri: Fosteralder, størrelse og vekst - Referanseverdier for ultralydmålinger" or "Fetal Biometry: Gestational age, size and growth - Reference values for ultrasound measurements" Synnøve Lian Johnsen and Torvid Kiserud. Section for Fetal Medicine & Ultrasound, Women's Clinic, Haukeland University Hospital; Section for Obstetrics and Gynecology, Department of Clinical Medicine, University of Bergen. Oktober 2006 ISBN-13:978-82-990918-7-9)
- "the basis for determining gestational age is not the end of the pregnancy, but its beginning."
(Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
Directorate of Health's Competence Regarding the Problematic, Unreliable BPD
In consideration of the overwhelming international evidence BPD is a problematic, unreliable predictor of GA during routine ultrasound exams, it is important to understand Bergen Group's Terminhjulet (or Term wheel) method does not depend on the 1-spacial-dimension BPD measurement for a direct estimation of GA during routine ultrasound exams. Bergen Group's Terminhjulet (or Forward wheel) method uses the more robust, 2-spacial dimensions HC measurement and, automatically, crosscheck HC & BPD with all available information, including, if available, LMPD/OTPD/SCID-based GA & EDD, for reasonableness, errors or efficacy. This is the practice of evidence-based medicine for determining fetal age and gestational age. Bergen Group considers all available information unlike NCFM eSnurra Group who implemented Directorate of Health's knowledge-obviated, medially & ethically flawed 2014 Recommendation within a government-mandated protocol of evidence-obviated medicine. So, why does Bergen Group crosscheck all the available evidence? Bergen Group answered this question in their article: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Norwegian Medical Association's Tidsskrift for Den norske legeforening (Tidsskr Nor Legeforen nr. 8, 2015; 135.).
Consequently, Torunn Janbu's statement of why the NCMF eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) was selected over Bergen Group's Terminhjulet (or Term wheel) method strains credulity and would be comical if it were not for the fact Directorate of Health caused (and causes) increased medical risks, critical medical mistakes and grievous medical harms to some of Norway's woman and their fetuses/babies, Laila and her baby among them. Moreover, NCFM eSnurra Group's exclusive, dubious dedication to, and irresponsible promotion of, the proven-to-be problematic and unreliable BPD measurement for the estimation of EDD and, therefrom, calculation of GA using the equivalent of Naegele's rule, in reverse, during routine ultrasound exams is a perfect example of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation; a Recommendation which selected NCFM eSnurra Group's "method" behind closed-doors and implemented same within a government-mandated protocol of evidence-obviated medicine "in an intentionally substandard fashion" after having been explicitly warned of the risks and consequences by Norway's medical experts, NGF, Bergen Group and others. Therefore, Directorate of health, in conjunction with NCFM eSnurra Group, implemented their knowledge-obviated, medically & ethically flawed 2014 Recommendation in conscious disregard of the identified risks and consequence. This was intentional recklessness and willful negligence which was, and remains, stone-cold criminal.
Wilful and Wanton Conduct Law and Legal Definition
In consideration of the overwhelming international evidence BPD is a problematic, unreliable predictor of GA during routine ultrasound exams, it is important to understand Bergen Group's Terminhjulet (or Term wheel) method does not depend on the 1-spacial-dimension BPD measurement for a direct estimation of GA during routine ultrasound exams. Bergen Group's Terminhjulet (or Forward wheel) method uses the more robust, 2-spacial dimensions HC measurement and, automatically, crosscheck HC & BPD with all available information, including, if available, LMPD/OTPD/SCID-based GA & EDD, for reasonableness, errors or efficacy. This is the practice of evidence-based medicine for determining fetal age and gestational age. Bergen Group considers all available information unlike NCFM eSnurra Group who implemented Directorate of Health's knowledge-obviated, medially & ethically flawed 2014 Recommendation within a government-mandated protocol of evidence-obviated medicine. So, why does Bergen Group crosscheck all the available evidence? Bergen Group answered this question in their article: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" published in the Norwegian Medical Association's Tidsskrift for Den norske legeforening (Tidsskr Nor Legeforen nr. 8, 2015; 135.).
- "We argue that critical mistakes may follow from the failure to include all available information when fetal age is assessed."
- "Terminhjulet suffers from a systematic bias that may cause too many pregnancies to be considered post-term, and some women may be given an erroneous EDD and an inaccurate fetal age." (Source: "One Norwegian national tool for estimating date of delivery and fetal age" Torunn Janbu, MD, PhD; Tidsskr Nor Legeforen nr. 9, 2016; 136)
- "may cause too many pregnancies to be considered post-term"
Yes, if Laila had been post-term instead of early, Laila's assigned NCFM eSnurra BPD-based EDD & GA would have allowed Laila to gestate for 44w+1 of "real" gestation time (a critical medical mistake) before any of Laila's medical professionals would have considered inducing labor, because grossly inaccurate NCFM eSnurra BPD-based EDD & GA are always correct, by government mandate, and may not be questioned. However, if Bergen Group's Terminhjulet (or Term wheel) method had been used, the more robust HC would have been among their ultrasound measurements and used to directly estimate GA and, therefrom, calculate a reasonable EDD, using the equivalent of Naegele's rule; and, Laila would not have endured an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications, and her baby would not have endured an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head.
"may be given an erroneous EDD"
Yes, again, Laila's assigned NCFM eSnurra BPD-based EDD was not just erroneous, it was grossly inaccurate, with a prediction error of -24 days, 3w+3, 4-days shy of a complete menstrual cycle/period, technically classified as a preterm by NCFM eSnurra Group's Gjessing et al. 2007. Moreover, Laila's assigned, grossly inaccurate NCFM eSnurra BPD-based EDD lagged Laila's factual LMPD-based EDD and her combined, fully corroborating, factual LMPD/OTPD/SCID-based EDD by 15 days and 14 days, respectively, which, of course, were ignored by NCFM eSnurra Group. However, if Bergen Group's Terminhjulet (or Term wheel) method had been used, the more robust HC would have been among their ultrasound measurements and used to directly estimate GA and, therefrom, calculate a reasonable EDD, using the equivalent of Naegele's rule; and, Laila would not have endured an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications, and her baby would not have endured an unidentified, prolonged, undiagnosed, untreated fetal growth restriction/malformation of her head.
"and an inaccurate fetal age"
Yes, Laila's baby was assigned an inaccurate fetal age because Laila was assigned a grossly inaccurate BPD-based eSnurra EDD and, therefrom, a grossly inaccurate GA was calculated, using the equivalent of Naegele's rule, in reverse, lagging Laila's combined, fully corroborating, factual LMPD/OTPD/SCID-based GA by 12 days. However, if Bergen Group's Terminhjulet (or Term wheel) method had been used, the more robust HC would have been among their ultrasound measurements and used to directly estimate GA and, therefrom, calculate a reasonable EDD, using the equivalent of Naegele's rule; and, Laila would not have endured an unwanted, unnecessary Cesarean section surgery delivery with a cascade of complications, , and her baby would not have endured a prolonged, undiagnosed, untreated FGR/malformation of her head.
"some women may be given an erroneous EDD and an inaccurate fetal age"
And, to follow this insidious, systemic problem even further, the erroneous, highly inaccurate, flat-out wrong NCFM eSnurra BPD-based GA at birth/deliver had been entered into Laila's baby's official national medical birth record at the Medical Birth Registry of Norway (MBRN). And, still, all of Laila's medical professionals are mandated to believe Laila's baby's GA = 37w+0 at delivery was accurate. Not one of Laila's medical professionals has ever admitted Helen's GA = 37w+0 at birth/delivery was inaccurate. Seriously, is there any better example than this for George Orwell's definition of the word doublethink. Moreover, the fact that this critical medical mistake made it all the way into Laila's baby's national medical birth record at MBRN is proof that these critical medical mistakes are silently and invisibly written off, unattributed, undocumented and unreported, as acceptable collateral damage of Directorate of Health's knowledge-obviated, medically & ethically flawed, intentionally reckless, willfully negligent 2014 Recommendation.
Consequently, Torunn Janbu's statement of why the NCMF eSnurra Group's method (i.e., the appropriated, plagiarized, misused Hutchon Method of PDEE) was selected over Bergen Group's Terminhjulet (or Term wheel) method strains credulity and would be comical if it were not for the fact Directorate of Health caused (and causes) increased medical risks, critical medical mistakes and grievous medical harms to some of Norway's woman and their fetuses/babies, Laila and her baby among them. Moreover, NCFM eSnurra Group's exclusive, dubious dedication to, and irresponsible promotion of, the proven-to-be problematic and unreliable BPD measurement for the estimation of EDD and, therefrom, calculation of GA using the equivalent of Naegele's rule, in reverse, during routine ultrasound exams is a perfect example of Directorate of Health's knowledge-obviated, medically & ethically flawed 2014 Recommendation; a Recommendation which selected NCFM eSnurra Group's "method" behind closed-doors and implemented same within a government-mandated protocol of evidence-obviated medicine "in an intentionally substandard fashion" after having been explicitly warned of the risks and consequences by Norway's medical experts, NGF, Bergen Group and others. Therefore, Directorate of health, in conjunction with NCFM eSnurra Group, implemented their knowledge-obviated, medically & ethically flawed 2014 Recommendation in conscious disregard of the identified risks and consequence. This was intentional recklessness and willful negligence which was, and remains, stone-cold criminal.
- "We hold the opinion that this recommendation is medically flawed and that the Directorate has conducted a muddled investigation process." (Source: "Flawed recommendation issued by the Norwegian Directorate of Health concerning the determination of fetal age" or "Helsedirektoratet gir feil anbefaling om bestemmelse av fosteralder" Cathrine Ebbing, MD, PhD, Synnøve Lian Johnsen MD, PhD, Jørg Kessler, MD, PhD, Torvid Kiserud, MD, PhD, Svein Rasmussen, MD, PhD., Nr. 8, 5 mai 2015, Tidsskr Nor Legeforen, 2015; 135:7401, DOI: 10.4045/tidsskr.15.0093)
- "In this instance we feel that the Directorate of Health has acted beyond their competence and that they have simplified the issues beyond all understanding." (Source: ibid.)
- "We argue that critical mistakes may follow from the failure to include all available information when fetal age is assessed." (Source: ibid.)
- "Both from a technical and procedural point of view NGF believes that Directorate of Health's handling of this matter is highly reprehensible, does not inspire confidence and unfortunately can be directly dangerous in relation to dealing with difficult clinical problems. NGF will therefore recommend its members deal with the recommendations given in the Guide in obstetrics in 2014 which is based on the best scientific knowledge after a long and thorough process, of which Directorate of Health was instrumental." (Source: NGF tar avstand fra Helsedirektoratets anbefaling for fastsetting av svangerskapslengde og termin, Norsk gynekologisk forening, Nyheter , 2014) (Note: The source is in Norwegian; this translation is via Google Translate.)
Wilful and Wanton Conduct Law and Legal Definition
- "A Willful and Wanton Conduct is a willful or wanton injury that must have been intentional or the act must have been committed under circumstances exhibiting a reckless disregard for the safety of others, such as a failure, after knowledge of impending danger, to exercise ordinary care to prevent it or a failure to discover the danger through recklessness or carelessness when it could have been discovered by the exercise of ordinary care. [Henslee v. Provena Hosps., 369 F. Supp. 2d 970, 977-978 (N.D. Ill. 2005)] " (Source: US Legal, Inc., USLegal.com: Legal Definitions: Willful and Wanton Conduct)
"Willful and wanton conduct means “acting consciously in disregard of or acting with a reckless indifference to the consequences, when the Defendant is aware of her conduct and is also aware, from her knowledge of existing circumstances and conditions, that her conduct would probably result in injury.” [Duncan v. Duncan (In re Duncan), 448 F.3d 725, 729 (4th Cir. Va. 2006)]" (Source: ibid.) - Medical Dictionary: willful negligence Malpractice Provision of health care in an intentionally substandard fashion, the most serious form of negligence, which may carry with it criminal charges. See Malpractice, Negligence. (Source: McGraw-Hill Concise Dictionary of Modern Medicine. S.v. "willful negligence." Retrieved September 17 2017 from http://medical-dictionary.thefreedictionary.com/willful+negligence)